Download presentation
Presentation is loading. Please wait.

1
Vascular Access at MUSC
Lynn Williams, RN Vascular Access Resource Nurse Specialty Nursing Department

2
Vascular Access Devices 2013
Objectives: Intro to Infusion Nursing Society (INS) Identify common types of venous access devices, inc general characteristics Discuss device selection & placement departments Review assessment, care and management of central venous access devices – C75 Central Venous Catheter Policy Identify potential complications and related interventions regarding a central venous access device
 Identify common types of venous access devices, inc general characteristics. Discuss device selection & placement departments. Review assessment, care and management of central venous access devices – C75 Central Venous Catheter Policy. Identify potential complications and related interventions regarding a central venous access device.")
3
Infusion Nursing Society (INS)
Recognized as the global authority in infusion nursing, dedicated to exceeding the public’s expectations of excellence by setting the standard for infusion care. The Standards of Practice are written to be applicable in all patient settings & address all patient populations. Be advised – the “Standards” is a legally recognized document.

4
General Characteristics of CVAD
Catheter Materials Polyurethane, Silicone, Impregnated, FDA approved for Power injection of IV contrast during radiological imaging French Sizes 1.2 fr – 15 fr Lumens Single, double, triple, & quad available *Golden rule – Less is more! Cuffed vs non-cuffed Valves Internal (tip) – Groshong External (hub) – PASV, Solo Power PICC With so many new products on the market it has become increasingly difficult for clinicians to keep abreast the nuances of each device. However, it is important that clinicians are knowledgeable re: the device design, purpose, limitations, warnings and precautions. Knowing what material the catheter is made of is important. Some catheter materials such as polyurethane are more thrombogenic than for ex. silicone. Patients at high risk for infection may benefit from those that are impregnated with antibiotic s ( Rifampin & Minocycline) or Silver. Catheters come in a variety of gauge sizes - from as small as 1.2 fr for the premature infant to 8 fr . – however, it is recommended to use the smallest gauge size to accommodate the prescribed therapy to reduce incidence of vein thrombosis. Catheters are available in single, double, triple and even quadruple lumens – however, studies show a direct correlation between number of lumens and risk of infection. Valves are built into the tip or external hub of catheters to prevent reflux of blood into the catheter to reduce catheter occlusion and use of heparin . Certainly, pts allergic to heparin could benefit from these catheters. 4 4
 – Groshong. External (hub) – PASV, Solo Power PICC. With so many new products on the market it has become increasingly difficult for clinicians to keep abreast the nuances of each device. However, it is important that clinicians are knowledgeable re: the device design, purpose, limitations, warnings and precautions. Knowing what material the catheter is made of is important. Some catheter materials such as polyurethane are more thrombogenic than for ex. silicone. Patients at high risk for infection may benefit from those that are impregnated with antibiotic s ( Rifampin & Minocycline) or Silver. Catheters come in a variety of gauge sizes - from as small as 1.2 fr for the premature infant to 8 fr . – however, it is recommended to use the smallest gauge size to accommodate the prescribed therapy to reduce incidence of vein thrombosis. Catheters are available in single, double, triple and even quadruple lumens – however, studies show a direct correlation between number of lumens and risk of infection. Valves are built into the tip or external hub of catheters to prevent reflux of blood into the catheter to reduce catheter occlusion and use of heparin . Certainly, pts allergic to heparin could benefit from these catheters")
5
Choosing the Best VAD for Each Patient
Diagnosis Prescribed therapy Duration of therapy Physical assessment Patient health history Support system/resources Case Managers Patient preference 5 5

6
List of drugs that d/t pH, osmolality or chemical structure, cause frequent IV restarts
Amphotericin-irritant All Penicillins – pH 10/hypertonic Bactrim - pH 10.0 Phenergan – pH 4.0 Calcium Gluconate – Hypertonic Potassium >20 KCL – Hypertonic Chemo Vesicants- pH PPN/TPN – Hypertonic Ciprofloxacin – pH 3.3 Rocephin – Irritant/hypertonic Dilantin – pH 12.0 Dobutamine – pH 2.5 Tobramycin – pH 3.0 Erthromycin – irritant Vancomycin – pH 2.4 Morphine(PCA) – pH 2.5
 – pH 2.5.")
7
Selection of Catheters and Sites

8
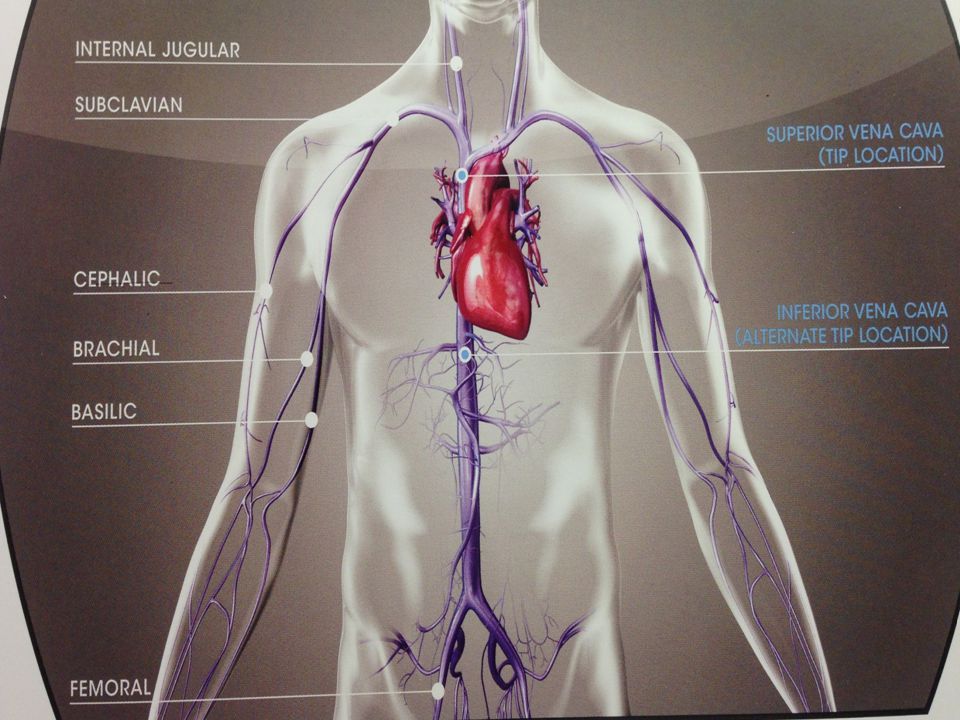
CDC Recommendations Catheters & Site selection
PIV vs PICC: Use a peripherally inserted central catheter (PICC) when the duration of IV Therapy will likely exceed six days Weigh the risks/benefits of placing a central venous device (CVD) at a recommended site to reduce infectious vs mechanical complications (IJ vs Subcl vs femoral)
 when the duration of IV Therapy will likely exceed six days. Weigh the risks/benefits of placing a central venous device (CVD) at a recommended site to reduce infectious vs mechanical complications (IJ vs Subcl vs femoral)")
9
Catheter & Site Selection cont’d
Choose a device with the minimum # of lumens/chambers essential for treatment Promptly remove catheters that are no longer essential

10
Central Venous Access Devices
Peripherally Inserted Central Catheters (PICC) Regular & cuffed/tunneled Non-tunneled/Non-cuffed Central Catheters Tunneled/Cuffed Central Catheters Implanted Ports – regular vs power There are four categories of central lines – each will be covered separately. 10 10
 Regular & cuffed/tunneled. Non-tunneled/Non-cuffed Central Catheters. Tunneled/Cuffed Central Catheters. Implanted Ports – regular vs power. There are four categories of central lines – each will be covered separately")
11
Departments that Place &/or Manage CVAD’s
VAIN Team Bedside PICC & difficult PIV insertion Screen all Adult IP PICC orders Adults Interventional Radiology Dept. Place all types of venous access devices All ages Infectious Disease PICC Service Place both cuffed & regular PICCs Bronch Lab, EP, Cath Lab OR/Surgeons All devices EXCEPT PICCs Pediatric Services Procedural area on 5th floor of CH – PICCs Bedside PICCs by specialized RNs in ICUs

13
Peripherally Inserted Central Catheters PICCs
Usually inserted using a vein in upper arm Can be used for most IV therapies and to obtain blood draws Select for pt’s requiring IV abx’s, TPN, poor IV access needing frequent blood draws Easily removed either at bedside while an IP or by a Home Health Nurse after discharge FYI – if pt has no insurance, they are unable to have device cared for at home

14
Adult PICC White Board All Adult PICC orders go to the VAIN team for evaluation and dept assignment for device insertion White Board provides info r/t which dept is assigned to insert PICC w/ comments Certain criteria dictate which dept is best suited to place the PICC: occlusion history, sedation, complicated diagnosis

15
Found on the Intranet

17
PICCs Placed at MUSC Cook Spectrum (polyurethane, Abx impregnated)
BARD Power PICC (polyurethane) Cook Silastic PICCs Cook Spectrum (polyurethane, Abx impregnated)
 Cook Silastic. PICCs. Cook Spectrum. (polyurethane, Abx impregnated)")
18
Centrally Inserted Catheter
Non-Tunneled CVC (no cuff) Short term, Acute care, percutaneous catheters Typically used for days – weeks for all types of IV therapy, blood draws, monitor central venous pressure in ICUs Example: PICCs, Acute single/dual/triple/Quad CVCs, Dialysis/aPheresis catheters Tunneled CVC (cuffed) Long term therapies – TPN, chemo Oncology, Cardiac, GI patients Dacron cuff provides catheter stability and serves as a barrier to prevent infection Examples: Cuffed PICCs, Chronic Dialysis/aPheresis catheters, Hickman, Broviac, Non-Tunneled catheters are temporary, short term catheters inserted percutaneously into the subclavian, jugular, and femoral veins. They can be inserted in an emergency situation at the bedside or in IR. Often, used if there are contraindications to using the veins of the upper arm for PICC insertion. Can easily be exchanged over a guidewire if infection is suspected or if multiple lumens no longer required. Tunneled catheters are surgically placed by tunneling the catheter under the skin from the vein entry point to an exit point on the chest. A nylon or Dacron cuff encircling the catheter provides catheter stabilization and serves as a barrier to infection as the tissue in the tract grows onto the cuff. These catheters are used when patients will require long-term therapy infusion. 18 18
 Short term, Acute care, percutaneous catheters. Typically used for days – weeks for all types of IV therapy, blood draws, monitor central venous pressure in ICUs. Example: PICCs, Acute single/dual/triple/Quad CVCs, Dialysis/aPheresis catheters. Tunneled CVC (cuffed) Long term therapies – TPN, chemo. Oncology, Cardiac, GI patients. Dacron cuff provides catheter stability and serves as a barrier to prevent infection. Examples: Cuffed PICCs, Chronic Dialysis/aPheresis catheters, Hickman, Broviac, Non-Tunneled catheters are temporary, short term catheters inserted percutaneously into the subclavian, jugular, and femoral veins. They can be inserted in an emergency situation at the bedside or in IR. Often, used if there are contraindications to using the veins of the upper arm for PICC insertion. Can easily be exchanged over a guidewire if infection is suspected or if multiple lumens no longer required. Tunneled catheters are surgically placed by tunneling the catheter under the skin from the vein entry point to an exit point on the chest. A nylon or Dacron cuff encircling the catheter provides catheter stabilization and serves as a barrier to infection as the tissue in the tract grows onto the cuff. These catheters are used when patients will require long-term therapy infusion")
19
Tunneled Non-tunneled
IJ entry site IJ entry site Subcutaneous Tunnel w/ cuff No subcutaneous Tunnel or cuff

20
Implantable Ports

21
Implantable Ports Chest, Arm, Thigh, Abdomen
Implanted Ports - Plastic, stainless steel or titanium housing attached to a catheter implanted under the skin Chest, Arm, Thigh, Abdomen Completely under skin – swimming permitted when not accessed once the incision has totally healed Requires special non-coring needles to access Available as power injectable Can remain in place for years Sickle cell, Oncology, Rheumatoid Arthritis, intermittent long term tx’s Subcutaneous implanted ports consist of a reservoir made of plastic, titanium or stainless steel with a self-sealing slicone septum attached to a radiopaque catheter. The catheter is tunneled but instead of exiting the chest it is attached to the reservoir and placed in a surgically created SQ pocket. Accessed with a Huber non-coring right angle needle – the smallest gauge size needle to accommodate the infusion should be used to prolong the life of the port. Nurses must assess which needle length is a perfect fit for the individual patient. May change as swelling goes down post insertion and with weight loss. If it is too short or too long the needle can back out of the silicone and infiltrate the infusion under the skin. Important to get swelling down and flush port before it clogs! Topical anesthetic creams can be used to minimize patient discomfort. – most pts request to be left on for 1 hour. Reminder, most pre-filled syringes are not sterile on the outside and should not be dropped on the sterile field when priming the huber needle. To meet the needs of patients requiring CT scans with contrast, ports have been developed to withstand the high pressures of power injectors, identified by ridges on the surface of the port or radiographic markings. When using power injectors, special noncoring needles that have the tubing attached must be used to ensure that the tubing and connections will not rupture or separate. 21 21

22
Identifying Power Ports
Prior to a fluoroscopic exam requiring power injection of contrast: Clinical staff (radiology techs, RNs) will positively ID device Manufacturers ID card, arm bracelet, key tag Manufacturers sticker found on IR/OR document Image – view “CT” marker on port chamber Radiologist to review prior image before being used If no prior image, an image of the appropriate anatomic area will be done & reviewed by Radiologist Radiology Dept. has a process they follow to confirm if a device is power injectable.
 will positively ID device. Manufacturers ID card, arm bracelet, key tag. Manufacturers sticker found on IR/OR document. Image – view CT marker on port chamber. Radiologist to review prior image before being used. If no prior image, an image of the appropriate anatomic area will be done & reviewed by Radiologist. Radiology Dept. has a process they follow to confirm if a device is power injectable.")
24
Port Needle Sets

25
Before Meds can be administered via CVAD:
Verify tip location using fluoroscopy For newly placed devices Transferred patients with an indwelling central venous catheter If there is a known or questionable change in catheter position Migration or dislodgement suspected Securement device has become dislodged S/S: No blood return &/or unable to flush If no blood return, device is not to be used until evaluated/treated for clot/thrombus or mechanical issues! Extremely important to verify initial tip placement and assess whether the tip position may have changed before administering medications. Solutions or medications with a pH <5 or >9 predispose the vein intima to irritation. Some examples are Doxycycline Ph 1.8, Dopamine Ph 2.5, Levaquin Ph 3.0, Tobramycin 3.0, Cipro Ph 3.3, Potassium 4.0, Phenergen 4.0, Vanco 2.4 – 4.5, Bactrim 10, Acyclovir 11, Dilantin To put that into perspective, I like to compare the pH of medications to things such as Gastric acid pH 1.5 – 2.0, Vinegar pH 2.9, and on the other end of the spectrum Ammonia pH 11.5. Continuous chemotherapy should be given via central line to prevent possible infiltration. Both cytotoxic and noncytotoxic (such as Nafcillin) have the potential for being categorized as irritants and vesicants because of chemical nature – this may have nothing to do with pH or osmolality. The vein intima can also be traumatized by the administration of hyperosmolar solutions (an osmolality >600) such as TPN, IVIG preparations 25
 have the potential for being categorized as irritants and vesicants because of chemical nature – this may have nothing to do with pH or osmolality. The vein intima can also be traumatized by the administration of hyperosmolar solutions (an osmolality >600) such as TPN, IVIG preparations. 25.")
26
IV Flush Orders Practitioner must write order for heparin flushes
Standard Adult and Pediatric flush orders Each device has a standard flushing protocol including 0.9% sodium chloride and heparin If heparin is contraindicated, consider alternative, such as argatroban or tPA When patient is admitted with a device, initiate the order for RN to get heparin

27
Dialysis/aPheresis catheters
Locked with high-dose heparin Refer to IV Flush Orders Adults: Use 1000u/ml heparin Pediatrics: Use 100u/ml heparin May only be accessed by nurses trained to do so (ICU, aPheresis & Dialysis RNs) Renal service must be consulted before using catheter. If no longer being used for aPheresis &/or dialysis, the Renal MD MUST transfer care to RNs on unit.
 Renal service must be consulted before using catheter. If no longer being used for aPheresis &/or dialysis, the Renal MD MUST transfer care to RNs on unit.")
28
Post-Insertion Complications
Catheter Dislodgement Catheter Migration Air Embolism Catheter-related Bloodstream Infection Venous Thrombosis Catheter Occlusion The patient is at risk for a number of complications as long as the catheter remains in place . The nurse /pateint and/or caregiver must constantly monitor for sx’s and sx’s of complications, be proactive to prevent complications from occurring and be knowledgeable of which actions to take in the event of their occurrence. 28 28

29
Catheter Dislodgement
Stabilization devices (Statlock, sutures, securement dressings) are used to prevent catheter from falling out, catheter tip malposition, and migration of bacteria If displacement is suspected, CXR is required to verify tip placement S/S of dislodgement – catheter malfunctioning, securement device lose, device is semi-pulled out Do not try to re-insert the device Even with stabilization devices or sutures, catheters can fall out, be pulled out or become dislodged. Nursing assessment should should include measurement of the length of the external part of the catheter at the time of placement as a baseline; tunneled catheters should be palpated to assess for coiling and exposure of the dacron cuff. Difficulty with apiration or infusion, leaking of solution from exit site, edema or burning sensation, or pain with infusion can also indicate a displaced catheter. CXR is required if catheter tip displacement is suspected 29 29
 are used to prevent catheter from falling out, catheter tip malposition, and migration of bacteria. If displacement is suspected, CXR is required to verify tip placement. S/S of dislodgement – catheter malfunctioning, securement device lose, device is semi-pulled out. Do not try to re-insert the device. Even with stabilization devices or sutures, catheters can fall out, be pulled out or become dislodged. Nursing assessment should should include measurement of the length of the external part of the catheter at the time of placement as a baseline; tunneled catheters should be palpated to assess for coiling and exposure of the dacron cuff. Difficulty with apiration or infusion, leaking of solution from exit site, edema or burning sensation, or pain with infusion can also indicate a displaced catheter. CXR is required if catheter tip displacement is suspected")
30
Catheter Migration Tip can spontaneously migrate into right atrium or internal jugular May result from coughing, ventilator, forceful flushing, heavy lifting, hypertension S/S = Inability to flush, infuse or aspirate “Ear gurgling” or “running stream” while catheter is being flushed Get a chest x-ray Catheter tip placement is always confirmed after insertion and before using to administer medications. However, the tip can spontaneously migrate into an adjacent vein resulting from changes in intrathoracic pressure associated with coughing or sneezing, mechanical ventilators, forceful flushing as with power injection, or heavy lifting. Some indicators that the tip may have migrated include: inability to flush, infuse or aspirate; ear gurgling or running stream heard when the catheter is flushed. Also, complaints of headache or pain, swelling, redness or discomfort in the shoulder, arm or neck may indicate catheter migration. If suspected, venographic studies should be performed. Infusing medications into these other areas can result in venous thrombosis. Generally, can be repositioned by guidewire exchange. 30 30

31
Catheter Tip Malposition
right jugular The picture shows a catheter tip that has migrated into the right jugular vein. 31

32
Catheter Related Bloodstream Infections (CRBSI)
During CVC insertion – use maximal sterile barrier precautions: Cap, mask, sterile gown, sterile gloves, sterile full body drape Put mask on if removing a dressing to inspect a site Prep skin using Chlorhexidine gluconate w/ alcohol – allow to dry!! Assess catheter necessity daily!

33
Venous Thrombosis Diagnosed via Vascular Ultrasound What do you do??
Before removal, consider this: Is the catheter functioning normally? Are symptoms manageable? Can patient receive anticoagulant treatment? Does patient have known occluded vessels that will compromise a new device plcmt in the future? Consider patients condition, long term treatment and the need for the existing device

34
Occlusion Management Partial Occlusion: device flushes, no blood return Total Occlusion: No flush or aspiration via device Both types of occlusions can safely be treated with Cathflo Activase (alteplase) If mechanical malfunction has been ruled out, order Cathflo for catheter occlusion Follow Occlusion Management guidelines (Appendix B in C75 Policy)
 If mechanical malfunction has been ruled out, order Cathflo for catheter occlusion. Follow Occlusion Management guidelines (Appendix B in C75 Policy)")
35
Device Removal RNs have to demonstrate competency to remove a non-tunneled catheter. RN competency is based on skill & frequency of performance ONLY dialysis or ICU RNs w/ demonstrated competency may remove large bore catheters (dialysis/aphersis) ONLY MDs and non-surgical specialist that are credentialed may remove cuffed devices, including PICCs.
 ONLY MDs and non-surgical specialist that are credentialed may remove cuffed devices, including PICCs.")
36
Air embolism = entry of a bolus of air into the vascular system; can occur during placement or after device removal Reduce the risk of embolism: Place the patient in Trendelenberg position to increase intrathoracic pressure, unless not tolerated or contraindicated Have patient hold breath and gently bear down (Valsalva). Sx’s & Sx’s include: palpitations, resp distress, hypotension, arrhythmias,
. Sx’s & Sx’s include: palpitations, resp distress, hypotension, arrhythmias,")
37
Non healing site over port!

38
Post port plcmt – bruising!

39
Extravasation

40
CDC Recommendations Educate/training clinicians who insert/maintain cath’s – *SIM Lab program being developed Use maximal sterile barrier precautions Use >0.5% chlorhexidine skin prep w/ alcohol (ChloraPrep = 2% = isopropyl alcohol) Avoid routine replcmt of CVCs as strategy to prevent infection Periodically assess knowledge of & adherence to guidelines
 Avoid routine replcmt of CVCs as strategy to prevent infection. Periodically assess knowledge of & adherence to guidelines.")
41
Central Venous Catheter Policy
Owner: Central Venous Access Committee Multidisciplinary team Purpose: Provide guidelines for the insertion & care of all VADs For all staff that handle or insert a Central VAD Includes: 8 Appendix Included: References, VAD Occlusion Mgmt, IV Flush Orders (Peds/Adults), CVL Guideline, Ethanol Lock Info Sheet, VAIN Team Guidelines
, CVL Guideline, Ethanol Lock Info Sheet, VAIN Team Guidelines.")
42
Lynn Williams, RN Vascular Access Resource Nurse 792-1143 11109
Questions??? Lynn Williams, RN Vascular Access Resource Nurse 11109

Similar presentations












>")
 Management of Central Venous Access Devices 2. HICKMAN CATHETER.>")

 involves injecting a medication directly into the blood via venous access devices IV products must be sterile.>")



 449-9330>")

