Download presentation
Presentation is loading. Please wait.

1
ESRD N ETWORK 6: QAPI D EVELOPMENT FOR D IALYSIS P ROVIDERS Leighann Sauls RN, CDN Director, Quality Improvement

2
Do You Recognize this?

4
T HINK W ARM H APPY T HOUGHTS !

5
F ACT OR F ICTION The Network collects endless information from the dialysis facility for no good reason

7
L ET ’ S E XPLORE THE R OLE OF THE N ETWORK ESRD Network 6 Incorporated Name – Southeastern Kidney Council 1 of 18 Networks in the Country Legislation that Networks exist

8
W HAT W E D O - Network 6 – CMS Contractors Clinical Performance Measures Anemia Adequacy Immunization Access Nutrition Complaints and Grievances ESRD data forms Patient and Provider Education

9
W HAT DOES THAT MEAN FOR THE FACILITY ? Participation in Quality Improvement Projects Complaints and Grievances Data Collection ESRD Forms

10
C URRENT Q UALITY I MPROVEMENT I NITIATIVES Focus On Increasing AV Fistulas in South Carolina Increasing AVF in Network 6 overall Anemia Management Adequacy Increasing Immunizations Decreasing Complaints and Grievances Decreasing Involuntary Discharges

11
D EVELOPING A Q UALITY A SSESSMENT P ERFORMANCE I MPROVEMENT (QAPI) P ROGRAM
 P ROGRAM")
12
V626 C ONDITION STATEMENT The dialysis facility must develop, implement, maintain and evaluate an effective, data driven, quality assessment and performance improvement program with participation by the professional members of the interdisciplinary team.

13
V627 C ONDITION STATEMENT Effective QAPI (V627) …an ongoing program that achieves : Measurable improvement in health outcomes Reduction of medical errors
 …an ongoing program that achieves : Measurable improvement in health outcomes Reduction of medical errors")
14
V627 C ONDITION STATEMENT The dialysis facility must maintain and demonstrate evidence of its quality improvement and performance improvement program for review by CMS

15
V638 M ONITORING I MPROVEMENT The facility must: Continuously monitor its performance Take actions that result in performance improvement Track to assure improvements are sustained over time

16
W HAT IS QAPI? Quality Assessment Performance Improvement (QAPI) Under QAPI, the focus is on assessing outcomes to see whether good results are being achieved. More proactive approach to quality and to improvement.
 Under QAPI, the focus is on assessing outcomes to see whether good results are being achieved. More proactive approach to quality and to improvement..")
17
D IFFERENCE BETWEEN QI AND QAPI? Quality Improvement focuses on structure and process Quality Assessment Performance Improvement focuses on assessing outcomes

18
QAPI E LEMENTS The professional members of the facility’s interdisciplinary team (IDT), which must participate in QAPI activities, consist of a physician, registered nurse, masters-prepared social worker, and registered dietitian.
, which must participate in QAPI activities, consist of a physician, registered nurse, masters-prepared social worker, and registered dietitian.")
19
QAPI E LEMENTS There must be an operationalized, written plan describing the QAPI program scope including: Objectives Organization Responsibilities of all participants Procedures for overseeing the effectiveness of monitoring, assessing, and problem-solving activities.

20
QAPI E LEMENTS Within the facilities QAPI program, facilities are expected to use the community-accepted standards and values associated with clinical outcomes as referenced on the MAT (measures assessment tool).
.")
22
QAPI E LEMENTS If a facility has areas of that do not meet target levels (per MAT) or areas where the facility performance is below average (per data reports), the facility is expected to take action toward improving those outcomes.
 or areas where the facility performance is below average (per data reports), the facility is expected to take action toward improving those outcomes.")
23
QAPI E LEMENTS QAPI requires the use of aggregate patient data to evaluate the facility patient outcomes. Hemodialysis and peritoneal dialysis patients should be reviewed separately since factors affecting their clinical outcomes may be different; both groups of patients must be reviewed on an ongoing basis.

24
QAPI E LEMENTS Data related to patient outcomes, complaints, medical injuries, and medical errors (clinical variances, occurrences and adverse events) should be used to identify potential problems and to identify opportunities for improving care.
 should be used to identify potential problems and to identify opportunities for improving care.")
25
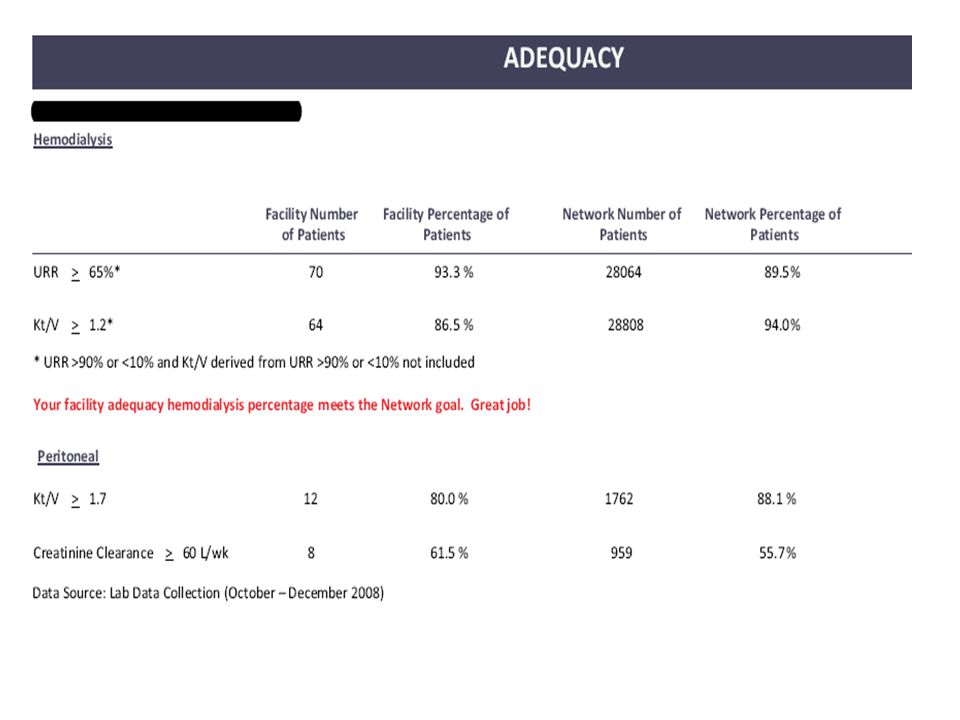
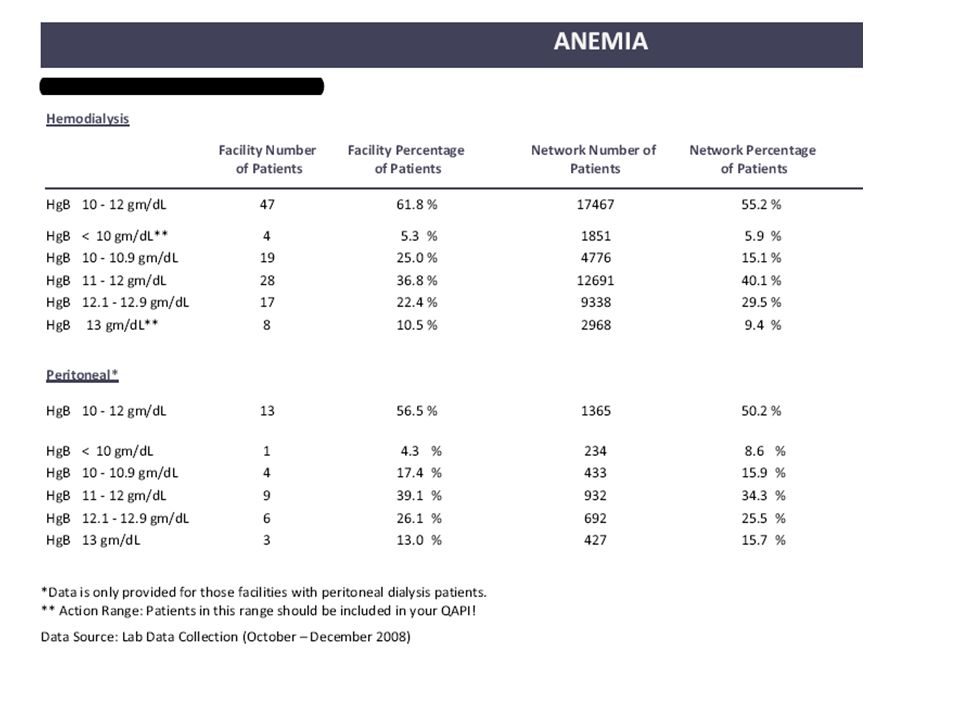
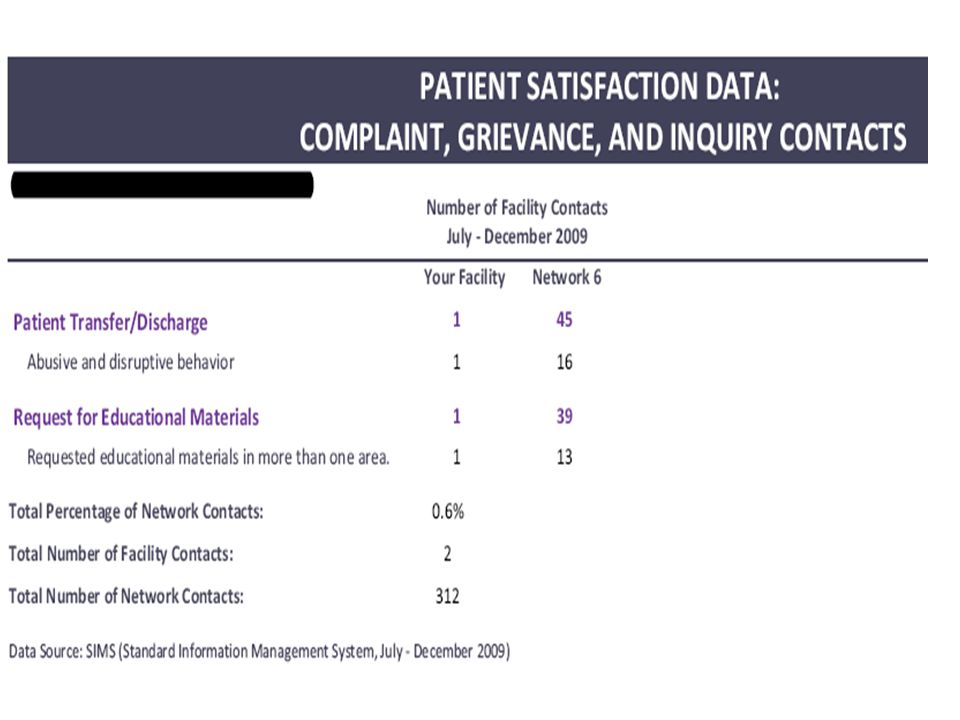
QAPI P ERFORMANCE M EASURES INCLUDE : (V629) AdequacyKt/V, URR (V630) NutritionAlbumin, body weight (V631) Bone diseasePTH, Ca+, Phos (V632) AnemiaHgb, Ferritin (V633)Vascular access Fistula, catheter rate (V634) Medical errors Frequency of specific errors V635) Reuse Adverse outcomes (V636) Pt satisfaction Survey scores (V637) Infection control Infections, vaccination status
 AdequacyKt/V, URR (V630) NutritionAlbumin, body weight (V631) Bone diseasePTH, Ca+, Phos (V632) AnemiaHgb, Ferritin (V633)Vascular access Fistula, catheter rate (V634) Medical errors Frequency of specific errors V635) Reuse Adverse outcomes (V636) Pt satisfaction Survey scores (V637) Infection control Infections, vaccination status")
26
A VAILABLE D ATA E LEMENTS CMS Dialysis Facility Reports (DFR) Facility Specific Data Outcomes Report Facility Produced Data Clinical Variance Reports Trending Reports from various facility systems
 Facility Specific Data Outcomes Report Facility Produced Data Clinical Variance Reports Trending Reports from various facility systems")
27
H OW TO DO IT … Identify the problem Review collective patient data; Look at trends Steady improvement or stable outcomes Abrupt or steady decline in outcomes Identify any commonalities among patients who do not reach the minimum expected targets; One vehicle accident may not indicate you are a bad driver….. However…10 accidents a year may cause your insurance company to make some changes in your plan!

28
N OW W HAT ? Develop Plan that results in improvement of care Identify Opportunity for Improvement Set Specific goal for Improvement Define and Measure Root Causes – PRIORITIZE! Identify Interventions Identify Person(s) responsible Date Process began Date/Frequency of Re-measurement Outcomes-Measurement results
 responsible Date Process began Date/Frequency of Re-measurement Outcomes-Measurement results.")
29
T HEN WHAT ? Work together – entire IDT Write clear statement identifying problem Use numerical “measurable” goal Set specific time range to meet goal Assure goal is obtainable within specified time range Use smaller goals in step by step fashion until ultimate goal is reached Example : GOAL: Reduce number of catheter patients to <10% by December 2010 Or …Reduce number of catheter patients by 2% each month

30
A ND MORE Identify Root Causes: For Example: If a data report shows that the facility’s ranking for hemodialysis adequacy is below the expected average Facility must demonstrate QAPI review of global factors that might affect adequacy Brainstorming with IDT Data/Spreadsheets to “measure” barriers

31
D EVELOP A CTION AND I NTERVENTIONS Focus on process What process can you change or create that will have a positive impact? Make actions barrier-specific How will changes impact the root cause? Choose one or two actions which will have the greatest impact (Rapid cycle improvement) Review available best practices Will they work in your facility? Discuss how you will monitor new processes How will you know if changes are an improvement?
 Review available best practices Will they work in your facility. Discuss how you will monitor new processes How will you know if changes are an improvement .")
32
C HANGE P ROCESSES Example: Facility determines inadequate BFR’s are highest priority root cause for patients not achieving adequacy Facility reviews current process and determines new process is needed NEW PROCESS > Daily audit checksheet: Nurse rounds after initiation of each shift to assure BFR and other prescription parameters are met Allows action to be taken immediately rather than waiting for monthly lab review to reveal a problem

33
E VALUATE Graph monthly data Review trends for improvement Discuss and document changes in monthly QAPI meetings What’s working? What’s not working?

34
PDCA

35
F OOD FOR THOUGHT Data reported is only as good as the data entered in the electronic or hard copy collection tools. This takes participation and cooperation of all staff.

36
Q UALITY IS NOT O NE S IZE F ITS A LL – INDIVIDUALIZE !

37
W HERE DO YOU GET DATA FOR YOUR QAPI?

48
C OMMENTS, Q UESTIONS, I DEAS – EMAIL THEM TO INFO @ NW 6. ESRD. NET Remember – We are Here to Help You !

Similar presentations

















 Texas Rules for ESRD Facilities What They Mean for the Renal Dietitian.>")











