Download presentation
Presentation is loading. Please wait.

1
Interdisciplinary Behavioral Health Training in Primary Care (A HRSA Allied Health Supported Grant) Joseph H. Evans, PhD Munroe Meyer Institute University of Nebraska Medical Center Omaha, Nebraska

2
Interdisciplinary Behavioral Health Training in Primary Care Behavioral Health Disciplinary Partners –MMI Psychology Department –Marriage & Family Therapy Program (Family Medicine Department) –MMI Social Work Department Counseling Programs (Statewide)
 –MMI Social Work Department Counseling Programs (Statewide)")
3
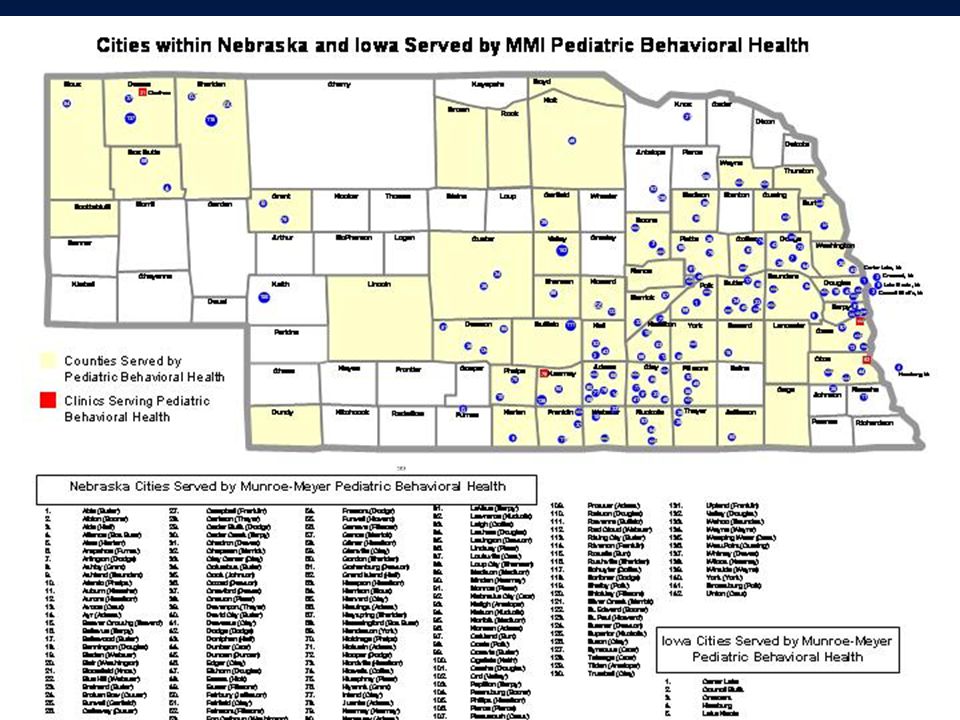
Rural Nebraska Mental Health Facts 88 of 93 counties are MH HPSAs 74% of MH professionals practice in Omaha and Lincoln 38 counties have 0 or 1 MH professionals Of 147 licensed psychiatrists, 113 are in Metro areas and 15 are in State facilities #s of NE MH professionals are lower than the national average, per capita Child-Adolescent therapists even fewer

4
One Solution: Integrated Behavioral Health in Primary Care Defined as –Provision of BH care within a primary health care setting –Integration of behavioral and physical health care services –Preventive and first line interventions for common behavioral/mental health problems presenting in primary care offices

5
Interdisciplinary BH Training in Primary Care Grant Grant Program Objectives –Improve and Extend the BH Training Model –Provide “Learning through Service Delivery” experiences in Underserved Areas –Evaluate Effectiveness of the Interdisciplinary BH Training Model and Disseminate Results –Improve Recruitment, Placement and Retention of BH professionals in Underserved Areas

6
Why Integrated BH Care? Physicians are “de facto” mental health providers. –60% of all care mental health visits occur in PC setting (Magill & Garrett, 1988) –25% pediatric PC visits include behavioral health concerns (Cooper, Valleley, Polaha, Begeny, Evans, in prep) –Pediatricians rank behavior most common problem (over ear infections) (Arndorfer, Allen, & Aljazireh, 1999)
 –25% pediatric PC visits include behavioral health concerns (Cooper, Valleley, Polaha, Begeny, Evans, in prep) –Pediatricians rank behavior most common problem (over ear infections) (Arndorfer, Allen, & Aljazireh, 1999).")
7
Interdisciplinary Community- Oriented Behavioral Health Training Internship Training in community primary care settings Interdisciplinary Rotation in roles of physicians, nurses, PTs, OTs, speech therapists, etc. Community Rotation in rural or urban underserved areas w/ docs, nurses, etc. Participation in Interdisciplinary Clinics for cerebral palsy, spina bifida, genetics, depression, neurobehavioral disorders, marital problems, etc.

8
Community-Based Training in Integrated Behavioral Health in Primary Care Mission Provision of Behavioral Health Training & Services in Underserved Rural and Urban Areas Attraction, Recruitment, Training, Placement and Retention of Behavioral Health Providers Training for Physicians and other Health Care Professionals in Underserved Community Settings Evaluation of Effectiveness

10
Integration of Behavioral Health into Primary Care Practice Advantages for Physicians: –Physicians have a “ready” referral source –Doctors can triage most “needy” patients –Coordinated care is possible –Patients are seen “in” the practice –15-20% more practice productivity

11
Columbus Community Hospital Pediatrics

12
Integration of Behavioral Health into Primary Care Practice Advantages for Patients: –Comfort in receiving MH care in your doctor’s office –Reduced stigmatization –Coordinated physical and mental health care –Reduced usage of inappropriate medical visits –Travel for rural patients/families is reduced

14
Integration of Behavioral Health into Primary Care Practice Advantages to MH Practitioners: –Consistent referral stream –Coordination of psychotropic medication and therapy approaches –Reduced/shared practice overhead –Physician availability for consultations regarding medical conditions affecting behavior

15
Hastings Behavioral Health Clinic

16
Barriers to an Integrated Primary Care Model Few MH training programs with interdisciplinary primary care focus MH training programs not located in university medical centers Scarcity of MH professionals interested in rural practice Lack of available incentives for rural MH practice “Carve out” MH insurance programs “Start-up” costs can be prohibitive

18
The UNMC/MMI Integrated Behavioral Health Model Rural Locations (1997-2004): –Columbus (1997-present) –Hastings (1999-present) –Fremont (1999-2002) –Plattsmouth (2000-present) –Nebraska City (2004-present) –Valley (2003-present) –Kearney (2004-present) –Chadron/Crawford/Gordon (2004-present)
: –Columbus (1997-present) –Hastings (1999-present) –Fremont ( ) –Plattsmouth (2000-present) –Nebraska City (2004-present) –Valley (2003-present) –Kearney (2004-present) –Chadron/Crawford/Gordon (2004-present)")
19
The UNMC Integrated Behavioral Health Model(cont’d) New Outreach Behavioral Health Clinics (introduced in 2005-06) –Crete (2005-present) –Lincoln (2005-present) –Creighton University Pediatrics (2005- present)
 New Outreach Behavioral Health Clinics (introduced in ) –Crete (2005-present) –Lincoln (2005-present) –Creighton University Pediatrics (2005- present)")
21
The MMI Integrated Behavioral Health Model Urban Locations (cont’d): –One World CHC (w/ FM) 2000-pres –Eagle Run (w/FM) 2002-present –Charles Drew CHC 2002-2005 –Papillion 2001-present –SONA Clinic (w/FM) 1998-present –Summit Plaza (w/FM) 1996-present –Lincoln Complete Childrens’ Care (2005) –Council Bluffs (IA) Cogley clinic (2002)
: –One World CHC (w/ FM) 2000-pres –Eagle Run (w/FM) 2002-present –Charles Drew CHC –Papillion 2001-present –SONA Clinic (w/FM) 1998-present –Summit Plaza (w/FM) 1996-present –Lincoln Complete Childrens’ Care (2005) –Council Bluffs (IA) Cogley clinic (2002)")
22
Behavioral Health Clinics Nebraska City Behavioral Health Clinic Est. 2004 at Physicians Clinic Kearney Behavioral Health Clinic Est. 2004 at Kearney Clinic, P.C. Chadron Behavioral Health Clinic Est. 2004 at Chadron Health Gordon Behavioral Health Clinic Est. 2004 at Gordon Clinic

23
The MMI Integrated Behavioral Health Model Components: –Co-location in the primary practice –Frequent contacts re: referrals with physicians and nurses –Cross-training sessions with the practice and the community –Relationships with community schools, courts, agencies, other providers –Provision of dx assessment info and clinical data for physicians (e.g., ADHD diagnostic protocols)
")
24
The MMI Integrated Behavioral Health Model Administrative Issues: –MH services are “value added” to the primary care practice –Licensing, credentialing, paneling, pre-authorizations, billing, collections -independent from rural office @ 1 st –Space and staff imposition minimal –Goal is to establish the “importance” of available MH services to physicians and their practices

25
Rural Impact - 2002

27
BHC Outreach Patient Visits

28
MMI Behavioral Health Outreach Clinics - Outcomes Training and Retaining Providers 54% trainees work in rural area after graduation 11 of 13 current rural outreach clinics directed/staffed by graduate of this training program - 9 at Ph.D. level Monthly meetings via teleconferencing to improve communication, decrease isolation, increase retention.

29
Outcome - Behavioral Health Trainees (2001-06) Psychology -U Nebraska at Lincoln -Mississippi State U -Syracuse U -Illinois State U -U Southern Mississippi -Xavier U -U Kansas -U Western Michigan Social Work –U Nebraska at Omaha Counseling –Wayne State College –U Nebr at Kearney –Chadron State College –Doane College Mar & Family Therapy –U Nebraska at Lincoln –BYU
 Psychology -U Nebraska at Lincoln -Mississippi State U -Syracuse U -Illinois State U -U Southern Mississippi -Xavier U -U Kansas -U Western Michigan Social Work –U Nebraska at Omaha Counseling –Wayne State College –U Nebr at Kearney –Chadron State College –Doane College Mar & Family Therapy –U Nebraska at Lincoln –BYU")
30
Outcome-Physicians Use of Empirical Assessment Protocols Measure% Present Pre- Protocol (N=76) % Present First Year After Training (N=28) % Present Third Year After Training (N=26) CBCL/Parent BASC 1%93% TRF/Teacher BASC 0%88%93% CPRS-R:S1%93% CTRS-R:S1%93%88% Parent ADHD-IV3%88%93% Teacher ADHD-IV1%88%93% ECBI3%93%88%
 % Present First Year After Training (N=28) % Present Third Year After Training (N=26) CBCL/Parent BASC 1%93% TRF/Teacher BASC 0%88%93% CPRS-R:S1%93% CTRS-R:S1%93%88% Parent ADHD-IV3%88%93% Teacher ADHD-IV1%88%93% ECBI3%93%88%")
31
MMI Behavioral Health Outreach Clinics - Outcomes 2005-06 Data –3 Publications in Refereed Journals –2 Journal Articles/Chapters in press –10 Presentations at National/Regional Conferences –3 Presentations at State Conferences –5 Presentations to Physician Groups –32 Community Presentations (Schools, Agencies, Parent Groups, etc) –11 Courses taught at Colleges/Universities (7 Rural)
 –11 Courses taught at Colleges/Universities (7 Rural)")
33
Patients Seen at Rural BHC - Percent In and Out of Town Percent

34
Fiscal Support for the MMI Integrated Behavioral Health Model HRSA Allied Health Training grant (2001-2007) HRSA Graduate Psychology Education grant (2004-2007) HRSA Quentin Burdick grant (1999-2002) Americorps State Formula grant (2004-2007) HRSA SEARCH grant (support from AHEC) Clinical revenue support University Faculty-time contributions
 HRSA Graduate Psychology Education grant ( ) HRSA Quentin Burdick grant ( ) Americorps State Formula grant ( ) HRSA SEARCH grant (support from AHEC) Clinical revenue support University Faculty-time contributions")
36
Integrated Behavioral Health Necessities: Interested Primary Care partner Willingness to participate in an education program for trainees Space (docs’ days off) Referrals available (Clinical experience is that 3 docs needed to support one MH professional) Administrative supports that can eventually be shifted to the practice
 Referrals available (Clinical experience is that 3 docs needed to support one MH professional) Administrative supports that can eventually be shifted to the practice")
37
The UNMC/MMI Integrated Behavioral Health Model Adjunct Service: The Pediatric Behavioral Telehealth Clinic –Initiated March, 2005 –60+ families served in 200+ visits to date –6-10 visits provided weekly –From 20+ remote sites as far as 452 miles from Omaha –Males and females ages 3 to 21 years

38
UNMC/MMI Rural Outreach Behavioral Health Care Program MMI Rural Beh Health Outreach Program Hastings Child/Adol Clinic** Columbus CCH Pediatrics Plattsmouth NMC Pediatrics Nebraska City Family Med Chadron Fam Med Clinic Requested Grand Island Peds Requested Norfolk Peds Requested Blair Comm Hosp Requested Lincoln LMEP Requested Crete Comm Hosp Kearney Pediatrics Fremont Pediatric Partners**

39
Integrated Behavioral Health Necessities Dedicated faculty/preceptors willing to travel to rural sites Students/graduates interested in rural practice (preferably from rural towns/training programs) Fiscal support for faculty and trainees Revenue support for travel/billing/ required equipment and supplies
 Fiscal support for faculty and trainees Revenue support for travel/billing/ required equipment and supplies")
40
Contact Information Joe Evans, PhD Director, Psychology Department at Munroe-Meyer Institute (MMI) and Professor, Dept of Pediatrics University of Nebraska Medical Center 985450 Nebraska Medical Center Omaha Nebraska 68198-5450 Phone: (402) 559-5758 E-mail: jevans@unmc.edu
 and Professor, Dept of Pediatrics University of Nebraska Medical Center Nebraska Medical Center Omaha Nebraska Phone: (402)")
41
QUESTIONS ?

Similar presentations











 Program A warm welcome from Dr. Thomas Roe, Co-Program Director.>")






 484-1908.>")
 Presentation to 3rd International Conference.>")




