Download presentation
Presentation is loading. Please wait.

3
Tuberculosis and the Eye- Epidemiology About one third of the world's population has latent tuberculosis, caused by Mycobacterium tuberculosis. From this pool, roughly 9 million cases of active tuberculosis emerge annually, resulting in 2-3 million deaths. Most new cases occur in the most populated nations. India and China, but the highest rates of disease are seen in sub- Saharan Africa, the Indonesian and Philippine archipelagos, Afghanistan, Bolivia, and Peru. In these regions case rates typically exceed 300 cases per 100 000 per year fection. The incidence of tuberculosis has increased in England and Wales over the past few years, with a current annual rate of 5000 to 6000 cases. For the year 2000, the Public Health Laboratory Service has had a 10.6% increase in notifications over 1999

4
Tuberculosis and the Eye- Epidemiology

5
Tuberculosis and the Eye- Contemporary Issues Although the incidence of tuberculosis declined in North America and western Europe throughout most of the latter half of the 20th century, case rates have increased over the past 10 years mainly because of immigration, HIV/AIDS, and the neglect of tuberculosis control programmes. It is recommended that all patients with tuberculosis undergo a test for HIV. Health workers are at risk of tuberculosis Treatment of active Tuberculosis gives cure rates above 95% provided that the strain of Mycobacterium tuberculosis is not multidrug resistant and that compliance is adequate. Non-adherence to treatment may decrease cure rates to 79% and increase the prevalence of multidrug resistant strains

6
Tuberculosis and the Eye- Contemporary Issues In 1992 the New York Post ran the headline: "TB timebomb. Homeless contaminate public areas in city." In April 1993 increasing rates of tuberculosis led to the World Health Organization declaring a global emergency. Tuberculosis has enjoyed a resurgence, allied as it is to economic and social fractures and the HIV epidemic.

7
Tuberculosis and the Eye- Contemporary Issues Globally, the most common opportunistic infection and the leading cause of death related to HIV infection is tuberculosis. The two main approaches to tuberculosis control are casefinding combined with treatment of active cases, and prevention of disease in infected people. A recent trial conducted in Zaire compared a six month therapeutic regimen (daily rifampin, isoniazid, pyrazinamide, plus ethambutol for two months followed by twice weekly rifampin plus isoniazid for four months) with a 12 month regimen The rate of relapse was higher after the shorter regimen, but survival was comparable. Prophylaxis of active disease with isoniazid for patients infected with HIV and tuberculosis is effective, but widespread implementation of such an approach in developing countries may not be feasible. The United States saw a resurgence of tuberculosis in the late 1980s and early 1990s that highlighted the devastating consequences of cutbacks in the infrastructure of tuberculosis control programmes. Several outbreaks of multidrug resistant tuberculosis occurred, primarily affecting people infected with HIV. In some areas, like New York city, as many as 19% of the cases of tuberculosis were attributable to multidrug resistant tuberculosis. Renewed attention to tuberculosis control has begun to deal with the problem in the USA.
 with a 12 month regimen The rate of relapse was higher after the shorter regimen, but survival was comparable. Prophylaxis of active disease with isoniazid for patients infected with HIV and tuberculosis is effective, but widespread implementation of such an approach in developing countries may not be feasible. The United States saw a resurgence of tuberculosis in the late 1980s and early 1990s that highlighted the devastating consequences of cutbacks in the infrastructure of tuberculosis control programmes. Several outbreaks of multidrug resistant tuberculosis occurred, primarily affecting people infected with HIV. In some areas, like New York city, as many as 19% of the cases of tuberculosis were attributable to multidrug resistant tuberculosis. Renewed attention to tuberculosis control has begun to deal with the problem in the USA..")
8
Tuberculosis and the Eye- Contemporary Issues HEALTH WORKERS Health and hospital workers vary in their risk of contracting and disseminating tuberculosis. Staff working with children or immunocompromised patients should have a chest radiograph before starting work. Mortuary workers, microbiology staff, and those caring for patients with tuberculosis should have a pre-employment chest radiograph and tuberculin test. Those who are tuberculin negative should be given BCG. Routine chest radiography during employment is not recommended. Other health workers should be given BCG vaccination, if indicated. Other specific precautions need not be taken.

9
Tuberculosis and the Eye- Pathology The tubercle bacillus was discovered by Robert Koch in 1882 Mycobacteria are Gram- positive, although they are not easily stained by this method. They are resistant to decolorization by mineral acids after staining with arylmethane dyes such as carbol fuchsin, hence the term acid-fast.

10
Tuberculosis and the Eye- Pathology Immune responses in tuberculosis may be either protective, leading to resolution of disease, or tissue destroying, leading to the pathological characteristics of active disease Both types of response are cell- mediated and there has been considerable controversy about whether protective and immunopathological responses are manifestations of the same mechanism, differing only in degree The characteristic histological lesion of tuberculosis is the granuloma, which consists of a chronic, compact aggregate of activated macrophages (epithelioid cells), some of which fuse to form multinucleate giant cells
, some of which fuse to form multinucleate giant cells")
11
Tuberculosis and the Eye- Pathology Mycobacterium tuberculosis uses a trick to invade cells. The body's immune system normally tags any invading bacteria with proteins that alert macrophages to consume it. One of these proteins, C2a, then floats in the blood with no known function. M tuberculosis manages to associate with this discarded C2a protein and use it to create a new label that helps the bacteria adhere to the macrophage and enter it. Once inside the macrophage, the mycobacteria multiply until the cell ruptures and the bacteria are then released to repeat the process

12
Tuberculosis and the Eye- Pathology The initial pulmonary lesion, the Ghon focus, together with the hilar lymphadenopathy, forms the primary complex of Ranke. Some bacilli are disseminated through lymphatics and blood, leading in some cases to meningeal, bone, and renal involvement.

13
Tuberculosis and the Eye-Standard Investigations CXR CultureSputum / urine culture / stain for AAFB (acid and alkali fast bacilli).Ziehl Neelsen stain or auramine-phenol fluorescent test are confirmatory Tuberculin hypersensitivity Mantoux Old Tuberculin = PPD (purified protein derivative) Biopsy
.Ziehl Neelsen stain or auramine-phenol fluorescent test are confirmatory Tuberculin hypersensitivity Mantoux Old Tuberculin = PPD (purified protein derivative) Biopsy")
14
Tuberculosis and the Eye-Standard Investigations Chest X Ray Reactivation tuberculosis

15
Tuberculosis and the Eye-Standard Investigations Radiological changes, though sensitive, are rather non-specific. Tuberculosis may cause virtually any radiological abnormality and atypical pictures are not uncommon, especially in HIV-positive and other immunocompromised persons. Bacteriological confirmation should always be sought.

16
SARCOIDOSIS AND TUBERCULOSIS Sarcoidosis and tuberculosis have several clinical and pathological features in common. Sarcoid often features cutaneous anergy. Both diseases are characterised by the formation of granulomas. These are usually caseating in tuberculosis, but areas of necrosis can occur in sarcoidosis. This overlap makes it difficult to distinguish between the two conditions in some cases, such as that of our patient. In addition, there are occasional well characterised cases in which both diseases seem to coexist,eading to suggestions that the association is causal. Moreover tuberculosis may become apparent after the treatment of sarcoidosis with corticosteroids, but this association is relatively rare. Isolation of mycobacterial DNA from sarcoid tissue using the polymerase chain reaction has been reported, but these data have not been consistently replicated and their significance remain uncertain. Winterbauer RH, Kraemer KG. The infectious complications of sarcoidosis. Arch Intern Med 1976;136:1356-62. [Medline][Medline] Fidler HM, Rook GA, Johnson NM, McFadden J. Mycobacterium tuberculosis DNA in tissue affected by sarcoidosis. BMJ 1993;306:546-9. [Medline][Medline] Bocart D, Lecossier D, De Lassence A, Valeyre D, Battesti JP, Hance AJ. A search for mycobacterial DNA in granulomatous tissue from patients with sarcoidosis using the polymerase chain reaction. Am Rev Respir Dis 1992;145:1142- 8. [Medline][Medline]

17
SARCOIDOSIS AND TUBERCULOSIS Neurosaroid- Meningeal biopsy by small burr hole and the use of the operating microscope is a procedure of low morbidity

18
Tuberculosis and the Eye- Ocular Manifestations Uveitis commonest Systemic disease is often apparent Eyelids- lupus vulgaris (nodules surrounded by erythema) Orbit- cellulitis, dacryoadenitis, dacryocystitis, osteomyelitis, abscess Conjunctiva- rarely affected, phlyctenular conjunctivitis described in some texbooks as allegic manifestation along with erythema nodosum. Cornea- phlyctenular keratoconjunctivitis, interstitial keratitis (unilateral, sectorial, superficial vascularisation) Sclera- episcleritis, nodular scleritis Uveitis- chronic granulomatous anterior uveitis, multifocal choroiditis, exudative retinitis, Vasculitis, optic nerve oedema, papilloedema
 Sclera- episcleritis, nodular scleritis Uveitis- chronic granulomatous anterior uveitis, multifocal choroiditis, exudative retinitis, Vasculitis, optic nerve oedema, papilloedema.")
19
Tuberculosis and the Eye- Ocular Manifestations Phlyctenular conjunctivitis, which may occur in some children within 1 year of the primary infection, consists of small, multiple, yellow or grey conjunctival nodules near the limbus, with a sheaf of dilated vessels.

20
Tuberculosis and the Eye- Case Presentation DOB 1974, 31 Years, male Pulmonary Tuberculosis Presented with recurrent vitreous haemorrhage R and L, Referred from Wolverhampton Rx Rifampicin, Isoniazid, Pyridoxine

21
Tuberculosis and the Eye- Case Presentation VA RE 6/5 LE6/5 Bilateral vitreous haemorrhages No obvious new vessels FFA and ICG 12/11/2002 Bilateral PRPs following angiography Now non complaint

22
Right Fundus

23
Left Fundus

24
Colour Fundus photography- multiple vascular lesions associated with vitreous haemorrhage

26
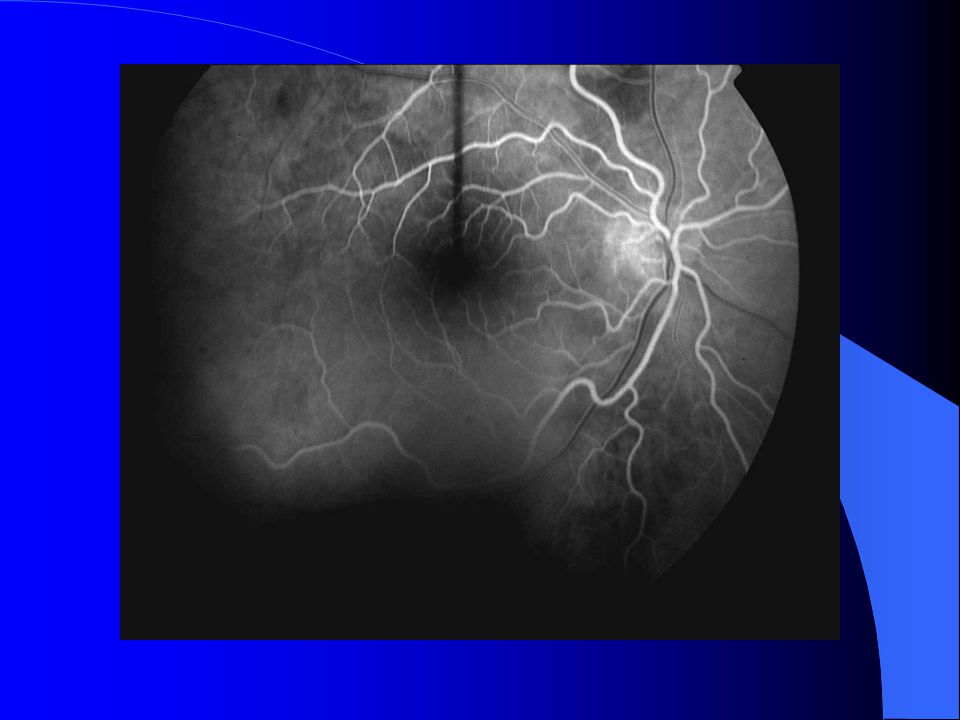
Flourescein Angiography RE NV’S AND VASCULAR LEAKAGE, VASCULAR REMODELLING, NO CMO, DISC HYPERFLOURESEN -CE LE MULTIPLE NV’S-NO CMO

27
Flourescein Angiography

34
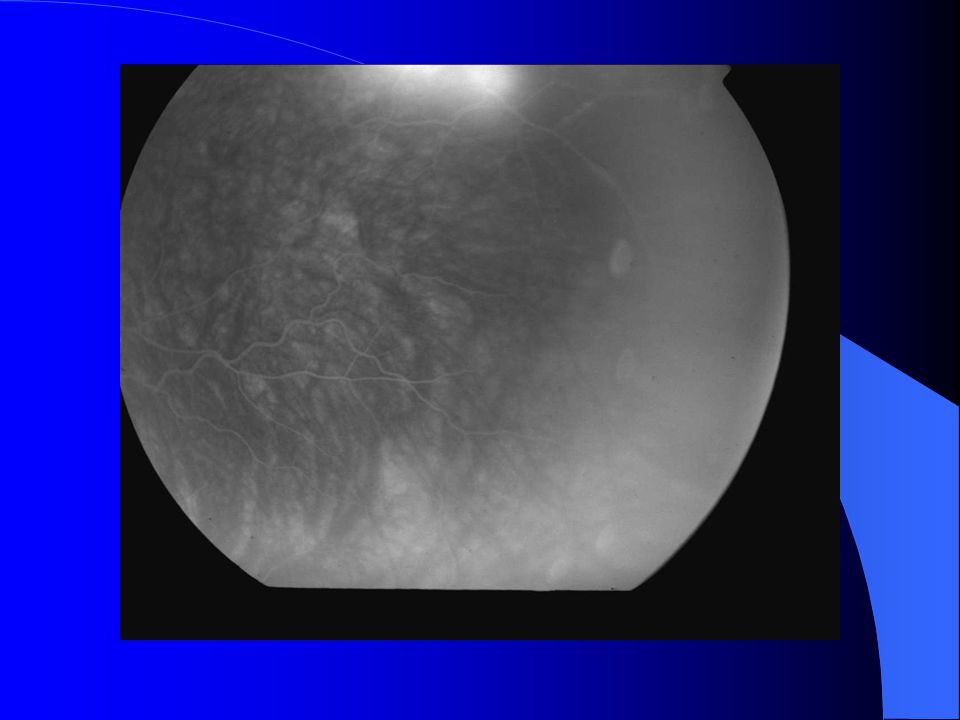
Tuberculosis and the Eye- Case Presentation ICG-delayed choroidal filling

36
THERAPEUTICS It is recommended that all patients with tuberculosis undergo a test for HIV. Supplements of pyridoxine (vitamin B6)not to exceed a daily dose of 50 mgare suggested for patients taking isoniazid to prevent peripheral neuritis. Particular attention should be given to patients at risk of neuropathy, including patients who are malnourished or pregnant. Baseline liver function tests and periodic and regular monitoring are advocated in view of the potential hepatotoxicity of isoniazid, rifampicin, and pyrazinamide. The risk of major liver damage is less than 1%, but mild asymptomatic increases in transaminase blood concentrations are seen in up to 20% of patients. Doses of ethambutol should be carefully adjusted in patients with renal impairment. Patients taking ethambutol should have their visual acuity checked initially and serially monitored (Snellen acuity and Ishihara colour). They should be instructed to report promptly any perceived disturbances in their vision.
not to exceed a daily dose of 50 mgare suggested for patients taking isoniazid to prevent peripheral neuritis. Particular attention should be given to patients at risk of neuropathy, including patients who are malnourished or pregnant. Baseline liver function tests and periodic and regular monitoring are advocated in view of the potential hepatotoxicity of isoniazid, rifampicin, and pyrazinamide. The risk of major liver damage is less than 1%, but mild asymptomatic increases in transaminase blood concentrations are seen in up to 20% of patients. Doses of ethambutol should be carefully adjusted in patients with renal impairment. Patients taking ethambutol should have their visual acuity checked initially and serially monitored (Snellen acuity and Ishihara colour). They should be instructed to report promptly any perceived disturbances in their vision..")
37
ETHAMBUTOL Ethambutol is bacteriostatic for M. tuberculosis in the dosages that can safely be given, and is used to prevent the emergence of strains resistant to other drugs. It should be avoided in the treatment of patients with impaired renal function as it may accumulate and cause serious ocular toxicity. It should not be given to young children or any patient unable to report early symptoms of ocular toxicity. The British Thoracic Society recommends that renal function and visual acuity should be assessed before the drug is prescribed, the recommended dosage should not be exceeded, any history of eye disease should be recorded, the patient should be told that the drug may rarely affect vision and drugs should be stopped immediately should vision become impaired, patients complaining of visual disturbance during chemotherapy should be referred to an ophthalmologist for detailed examination, and the family practitioner should be told what information and instructions have been given to the patient. All these precautions and pieces of advice to the patient should, of course, be recorded in the case notes.

38
EALE’S DISEASE Obliterative vasculitis affecting the peripheral retina M>F, 30-40yrs India, Pakistan and Middle East 50% have TB or have been exposed to TB bacillus. No definite cause but there is a definite association with the Tubercle bacillus perhaps mediated by a hypersensitivity to tuberculin protein. Presents with vitreous haemorrhages or floaters. Sheathed vessels especially veins with peripheral non- perfusion and NVE, NVD and rarely rubeosis Anterior chamber activity, vitritis and CMO Associated vestibuloauditory dysfunction –

39
Outcome The overall mortality for all forms of tuberculosis in Great Britain is about 8 per cent, varying from under 1 per cent for children and young adults to over 30 per cent in those aged 75 years or more. Mortality is higher for patients with extensive disease, smear positivity and cavitation. Mortality appears to be the same in both sexes, even though males are twice as likely to develop pulmonary disease. Most deaths occur early in treatment: a recent study showed that over two-thirds of deaths due to pulmonary tuberculosis occurred within 4 weeks of starting chemotherapy.

Similar presentations
























 Gram (+) rod (bacilli). Acid-fast Pulmonary.>")


