Download presentation
Presentation is loading. Please wait.

1
EEG, Sleep and sleep disorders
R. Hamish McAllister-Williams, MD, PhD, FRCPsych Reader in Clinical Psychopharmacology Newcastle University Consultant Psychiatrist Regional Affective Disorders Service Northumberland Tyne and Wear NHS Foundation Trust

2
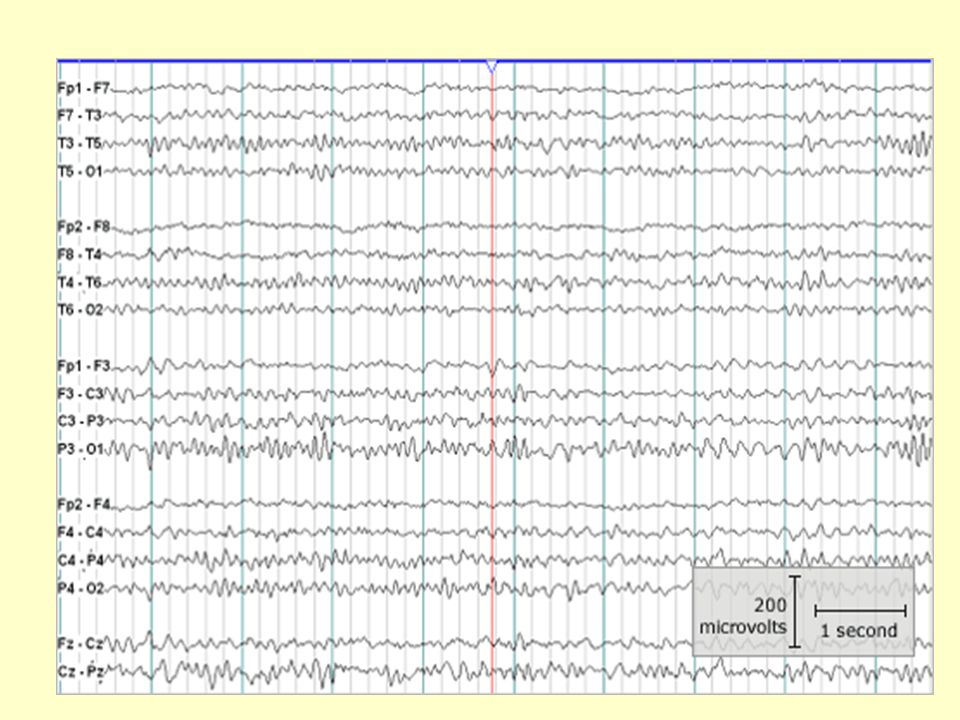
EEG

4
EEG electrode placements

7
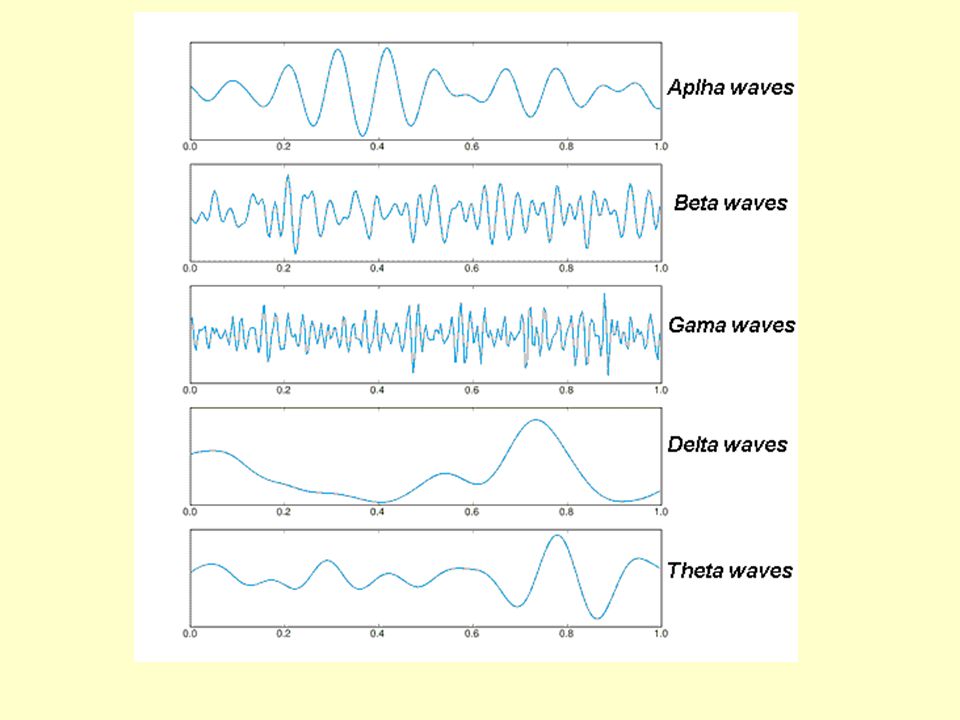
Type Frequency (Hz) Location Normally Pathologically Alpha 8 – 13 Beta
posterior regions of head, higher in amplitude on non-dominant side. Central sites at rest relaxed/reflecting closing the eyes Also associated with inhibition control, seemingly with the purpose of timing inhibitory activity in different locations across the brain. coma Beta 13 – 30 symmetrical distribution, most evident frontally; low amplitude waves alert/working active, busy or anxious thinking, active concentration benzodiazepines Gamma 30 – 100+ Somatosensory cortex Displays during cross-modal sensory processing Also is shown during short term memory A decrease in gamma band activity may be associated with cognitive decline

8
Type Frequency (Hz) Location Normally Pathologically Delta up to 4
frontally in adults, posteriorly in children; high amplitude waves adults slow wave sleep in babies Has been found during some continuous attention tasks subcortical lesions diffuse lesions metabolic encephalopathy hydrocephalus deep midline lesions Theta 4 – 8 Found in locations not related to task at hand young children drowsiness or arousal in older children and adults idling Associated with inhibition of elicited responses (has been found to spike in situations where a person is actively trying to repress a response or action) focal subcortical lesions metabolic encephalopathy deep midline disorders some instances of hydrocephalus
 focal subcortical lesions. metabolic encephalopathy. deep midline disorders. some instances of hydrocephalus.")
9
EEG: Fast Fourier transformation (FFT) analysis
 analysis")
10
Clinical uses of the EEG
Detection (and localisation) of seizure activity To detect encephalopathy To determine depth of anaesthesia Adjunct test of brain death
 of seizure activity. To detect encephalopathy. To determine depth of anaesthesia. Adjunct test of brain death.")
11
EEG – spikes and waves

12
EEG – lithium induced changes

13
Sleep

14
Underlying physiology and pharmacology of sleep
Normal sleep Measurement of sleep and sleep architecture Structures and neurotransmitters involved in sleep regulation

15
How much sleep do we need?
we need as much as is necessary to stop us feeling fatigued or sleepy the next day to enable us to perform our daily routine adequately

16
How much sleep do we need?
Very variable from person to person, but 7-8 hrs common Less than 5 hours causes problems with performance in normal young volunteers in a lab* More than 10 hours sometimes causes ‘sleep drunkenness’ Many people prefer 2 sleep periods (siesta) Some people use naps to catch up Many normal people have shorter sleep on weekdays and make up the ‘sleep debt’ at weekends *Dinges et al (1997) Sleep 20(4):
 Some people use naps to catch up. Many normal people have shorter sleep on weekdays and make up the ‘sleep debt’ at weekends. *Dinges et al (1997) Sleep 20(4):")
17
Why do we sleep when we do?
Coincidence of 3 processes Circadian process (‘body clock’) Time since last sleep (wake-dependent drive, homeostasis) Low arousal (relaxing, winding down)
 Time since last sleep (wake-dependent drive, homeostasis) Low arousal (relaxing, winding down) ")
18
Circadian and homeostatic drives to sleep interact
wake sleep sleep wake sleep sleep wake sleepy alert noon noon midnight midnight noon noon midnight midnight noon noon

19
Sleep: arousal / alertness / worry
High arousal can overcome other drives to sleep Worry, stimulants Low arousal can overcome other drives to be awake Boredom, sedating drugs

20
Measuring sleep Subjective measures Objective measures
Ask the patient (include evening, bedtime, night, next day) Questionnaires Diary Objective measures Actigraphy – wrist-worn, measures movement
 Questionnaires. Diary. Objective measures. Actigraphy – wrist-worn, measures movement.")
21
Measuring sleep Polysomnography - measures continuous brain activity, eye movement, muscle activity (+ respiratory variables if required) Waveforms interpreted visually to produce hypnogram of sleep stages

22
Idealized normal hypnogram: first sleep cycle
awake REM Stage 1 ‘drowsy’ state, not perceived as fully asleep sounds seem far away eyes roll from side to side happens in front of TV, in lectures etc stage 1 stage 2 stage 3 stage 4 11.30pm 7.30am 1 2 3 4 5 6 7 8 hours

23
Idealized normal hypnogram: first sleep cycle
awake K complex sleep spindle REM stage 1 light sleep, ~50% of night breathing & heart slower, muscles more relaxed ‘falling’ sensations and sleep jerks happen some imagery stage 2 Stage 2 stage 3 stage 4 7.30am 1 2 3 4 5 6 7 8 hours

24
Idealized normal hypnogram: first sleep cycle
awake ‘restorative’ stage of sleep, if deprived will always be made up deep sleep, 20% of night in young adults slower heart / breathing, muscles relaxed, pale confused on waking straight from this stage some imagery REM stage 1 stage 2 stage 3 Stages 3,4 (Slow wave sleep) stage 4 11.30pm 7.30am 1 2 3 4 5 6 7 8 hours
 stage pm. 7.30am hours.")
25
Idealized normal hypnogram: first sleep cycle
EEG like alert waking awake lateral eye jerks REM REM (rapid eye movement sleep) cortex active (‘paradoxical sleep’) muscles paralysed eyes move rapidly from side to side heart rate, breathing, autonomic function as awake most dreaming (bizarre, storylike) stage 1 stage 2 stage 3 stage 4 11.30pm 7.30am 1 2 3 4 5 6 7 8 hours
 cortex active (‘paradoxical sleep’) muscles paralysed. eyes move rapidly from side to side. heart rate, breathing, autonomic function as awake. most dreaming (bizarre, storylike) stage 1. stage 2. stage 3. stage pm. 7.30am hours.")
26
Idealized normal hypnogram
awake REM stage 1 stage 2 stage 3 stage 4 11.30pm 7.30am 1 2 3 4 5 6 7 8 hours

27
Time asleep/time in bed
Normal hypnogram REM latency 70-90 min 1 2 3 4 5 6 7 8 hours awake movement REM stage 4 stage 3 stage 2 stage 1 Sleep efficiency Time asleep/time in bed 96%

28
Ascending arousal system
thalamus Basal forebrain, ACh VTA dopamine Pontine nuclei,ACh Hypothalamus, histamine,orexin Locus coeruleus, NA Raphe, 5HT

29
Ascending arousal system
thalamus

30
Inhibition of arousal system during sleep
- During sleep, projections from the VLPO nucleus in the hypothalamus (GABA, galanin) inhibit the main components of the arousal system
 inhibit the main components of the arousal system.")
31
Neurotransmitters and sleep in humans
Endogenous transmitter Maintains wakefulness Promotes sleep Agents promoting wakefulness Agents promoting sleep Agents causing sedation GABA agonists, positive allosteric modulators melatonin M1 and M2 agonists adenosine antagonist noradrenaline uptake blockers releasers (stimulants) a1 antagonists dopamine serotonin 5HT2 antagonists, 5HTP histamine H1 antagonists acetylcholine muscarinic antagonists orexin antagonists
 a1 antagonists. dopamine. serotonin. 5HT2 antagonists, 5HTP. histamine. H1 antagonists. acetylcholine. muscarinic antagonists. orexin. antagonists.")
32
Drugs and sleep in humans
Endogenous transmitter Maintains wakefulness Promotes sleep Examples of drugs promoting wakefulness Examples of drugs promoting sleep Examples of drugs causing sedation GABA Benzodiazepines Z drugs melatonin Melatonin, ramelteon adenosine caffeine noradrenaline atomoxetine amphetamines a1 antagonists dopamine uptake blockers releasers (stimulants) eg ropinirole serotonin SSRIs mirtazapine, olanzepine histamine ?H3 antagonists ? promethazine H1 antagonists acetylcholine muscarinic antagonists orexin antagonists
 eg ropinirole. serotonin. SSRIs. mirtazapine, olanzepine. histamine. H3 antagonists. promethazine. H1 antagonists. acetylcholine. muscarinic antagonists. orexin. antagonists.")
33
Sleep Disorders and their treatment

34
Sleeping and waking – what goes wrong
insomnia not enough sleep or sleep of poor quality hypersomnia excessive daytime sleepiness parasomnia unusual happenings in the night other, eg: circadian rhythm disorders restless legs syndrome Full classification in ICSD (2001) International Classification of Sleep Disorders - Diagnostic and Coding Manual, American Academy of Sleep Medicine, Chicago.
 International Classification of Sleep Disorders - Diagnostic and Coding Manual, American Academy of Sleep Medicine, Chicago.")
35
Sleeping and waking – what goes wrong
insomnia not enough sleep or sleep of poor quality hypersomnia excessive daytime sleepiness parasomnia unusual happenings in the night other, eg: circadian rhythm disorders restless legs syndrome Full classification in ICSD (2001) International Classification of Sleep Disorders - Diagnostic and Coding Manual, American Academy of Sleep Medicine, Chicago.
 International Classification of Sleep Disorders - Diagnostic and Coding Manual, American Academy of Sleep Medicine, Chicago.")
36
What is insomnia? A+B+C A Difficulty - initiating sleep,
- maintaining sleep, waking up too early or sleep is chronically non-restorative or poor in quality B Occurs despite adequate opportunity and circumstances for sleep C At least one form of daytime impairment i. Fatigue or malaise ii. Attention, concentration, or memory impairment iii.Social or vocational dysfunction or poor school performance iv.Mood disturbance or irritability v.Daytime sleepiness vi.Motivation, energy, or initiative reduction vii.Proneness for errors or accidents at work or while driving viii.Tension, headaches, or gastrointestinal symptoms in response to sleep loss ix.Concerns or worries about sleep Severity and duration criteria in DSM IV, ICD-10, ICSD International Classification of Sleep Disorders (ICSD)
")
37
Diagnosing insomnia: Preliminary questions for eliminating other sleep disorder as primary Are you a very heavy snorer? Does your partner say that you sometimes stop breathing at night? (obstructive sleep apnoea syndrome (OSAS)) Do your legs often twitch and can’t keep still in bed? Do you wake from sleep with jerky leg movements? (restless legs syndrome - RLS, periodic limb movements in sleep - PMLS) Do you sometimes fall asleep in the daytime completely without warning? Do you have collapses or extreme muscle weakness triggered by emotion, for instance when you’re laughing? (narcolepsy) Do you tend to sleep well but just at the “wrong times”; and are these sleeping and waking times regular? (circadian rhythm sleep disorder; evidence also from sleep diary) Do you have unusual behaviours associated with your sleep that trouble you or that are dangerous? (parasomnias) BAP consensus statement on evidence-based treatment of insomnia, parasomnias and circadian rhythm disorders 2010
) Do your legs often twitch and can’t keep still in bed Do you wake from sleep with jerky leg movements (restless legs syndrome - RLS, periodic limb movements in sleep - PMLS) Do you sometimes fall asleep in the daytime completely without warning Do you have collapses or extreme muscle weakness triggered by emotion, for instance when you’re laughing (narcolepsy) Do you tend to sleep well but just at the wrong times ; and are these sleeping and waking times regular (circadian rhythm sleep disorder; evidence also from sleep diary) Do you have unusual behaviours associated with your sleep that trouble you or that are dangerous (parasomnias) BAP consensus statement on evidence-based treatment of insomnia, parasomnias and circadian rhythm disorders")
38
Why treat insomnia? Impaired quality of life
Impaired daytime performance (objectively measured), accidents at work, road accidents ↑ absenteeism (associated with 13.6% of DOR - Hajak et al, 2011) ↑ risk of hypertension ↑ risk of first episode/relapse of depression
, accidents at work, road accidents. ↑ absenteeism (associated with 13.6% of DOR - Hajak et al, 2011) ↑ risk of hypertension. ↑ risk of first episode/relapse of depression.")
39
Algorithm for treatment of insomnia: Wilson et al. 2010 BAP Guidelines

40
Individual hypnotic drugs (efficacy)
Significantly different from placebo Sleep onset latency Total sleep time Wake time after sleep onset Sleep quality Self-rated PSG Self-rated PSG Self-rated PSG Self-rated temazepam ()* ()* lormetazepam zopiclone zolpidem No zaleplon No No No No eszopiclone ramelteon (week 1 only) No PR melatonin Not measured No Not measured No PSG = polysomnography * formulation changed since studies, longer absorption time with current tablet cf gel capsule previous formulation
* ()* lormetazepam. zopiclone. zolpidem. No. zaleplon. No. No. No. No. eszopiclone. ramelteon. (week 1 only) No. PR melatonin. Not measured. No. Not measured. No. PSG = polysomnography. * formulation changed since studies, longer absorption time. with current tablet cf gel capsule previous formulation.")
41
Adverse effects of hypnotics1
Dose dependent effects on cognition NEXT-DAY DRIVING Epidemiology studies show that road accidents increase with benzos and zopiclone deficits in driving simulator performance with benzos and zopiclone no reported effects of zolpidem, zaleplon, PR melatonin REBOUND (worsening of sleep after stopping) except zaleplon, melatonin, ramelteon 1. Baldwin et al. J Psychopharm :
 except zaleplon, melatonin, ramelteon. 1. Baldwin et al. J Psychopharm :")
42
Benzodiazepine Dependency
Primary care attendees (n=1048)1 Self rated Severity of Dependence Scale Prevalence = 47% Random community sample of over 65’s (n=2785) 25.4% taking benzodiazepines Of these: 9.5% met DSM criteria for dependency 43% self reported being dependent De las Cuevas et al. 2003 Voyer et al. 2010
1. Self rated Severity of Dependence Scale. Prevalence = 47% Random community sample of over 65’s (n=2785) 25.4% taking benzodiazepines. Of these: 9.5% met DSM criteria for dependency. 43% self reported being dependent. De las Cuevas et al Voyer et al")
43
Hypnotics, excess mortality and dementia
Prospective study (20yr) in Sweden 1 regular hypnotic use ↑ all-cause mortality risk hazard ratios: men 4.54 ( ) / women 2.03 ( ) high association with suicide Retrospective study in US 2 prescription of hypnotic increased hazard ratio > threefold even if < 18 pills prescribed p.y. (dose response association) applied to several common hypnotics incl. antihistamines for high users: ↑ incident cancer, RR: 1.35 ( ) Prospective 15yr study in France3 New use of BZs associated with HR 1.6 ( ) for dementia 1. Mallon et al, Sleep Med. 2009; 10(3): 2. Kripke, BMJ 2012;2:e 3. Billioti de Gage et al. BMJ :e6231
 in Sweden 1. regular hypnotic use ↑ all-cause mortality risk. hazard ratios: men 4.54 ( ) / women 2.03 ( ) high association with suicide. Retrospective study in US 2. prescription of hypnotic increased hazard ratio > threefold. even if < 18 pills prescribed p.y. (dose response association) applied to several common hypnotics incl. antihistamines. for high users: ↑ incident cancer, RR: 1.35 ( ) Prospective 15yr study in France3. New use of BZs associated with HR 1.6 ( ) for dementia. 1. Mallon et al, Sleep Med. 2009; 10(3): Kripke, BMJ 2012;2:e Billioti de Gage et al. BMJ :e6231.")
44
Hypnotics – duration of treatment
Recommendation Use as clinically indicated (A) To stop medication try intermittent use at first if it makes sense, then try to stop at regular intervals – say every 3-6 months depending on ongoing life circumstances and with patient’s consent (D) CBT during taper improves outcome (A)
 To stop medication try intermittent use at first if it makes sense, then try to stop at regular intervals – say every 3-6 months depending on ongoing life circumstances and with patient’s consent (D) CBT during taper improves outcome (A)")
45
Cognitive-behavioural therapy works in chronic insomnia
Suggested behaviors No clock-watching Bedroom for sleeping Scheduling time for planning, worrying etc early evening Behavioral techniques Sleep restriction Paradoxical intent Cognitions Working on attitudes and beliefs about sleep Changing negative automatic thoughts re: not falling asleep now dire consequences Sleep remained improved 1y later & 84% of patients were drug free Espie et al, Behav Res Ther, 2001; 39(1):45-60
:")
46
Sleeping and waking – what goes wrong
insomnia not enough sleep or sleep of poor quality hypersomnia excessive daytime sleepiness parasomnia unusual happenings in the night other, eg: circadian rhythm disorders restless legs syndrome Full classification in ICSD (2001) International Classification of Sleep Disorders - Diagnostic and Coding Manual, American Academy of Sleep Medicine, Chicago.
 International Classification of Sleep Disorders - Diagnostic and Coding Manual, American Academy of Sleep Medicine, Chicago.")
47
Hypersomnia - excessive daytime sleepiness
Common causes lack of sleep without any underlying disease (insufficient sleep syndrome) depression, neurological disorders, drug effects Caused by primary sleep disorder fragmentation of nocturnal sleep (e.g. by breathing related disorders such as obstructive sleep apnea, movement disorders or parasomnias) intrusion of sleep phenomena into the awake state (e.g. in narcolepsy) disturbances of circadian rhythms (e.g. in delayed sleep phase syndrome, shift work sleep disorder).
 depression, neurological disorders, drug effects. Caused by primary sleep disorder. fragmentation of nocturnal sleep. (e.g. by breathing related disorders such as obstructive sleep apnea, movement disorders or parasomnias) intrusion of sleep phenomena into the awake state (e.g. in narcolepsy) disturbances of circadian rhythms (e.g. in delayed sleep phase syndrome, shift work sleep disorder).")
48
Treatment of hypersomnia: Modafinil
wakefulness-promoting drug used to reduce excessive daytime sleepiness in narcolepsy 1 restores alertness only moderately mode of action reduces cortical GABA (catecholamine-dependent)2 increases histamine in TMN (indirectly)3 increases extracellular glutamate4 (also indirectly5) 1. Wise et al., Sleep, 2007; 30(12): 2. Tanganelli et al., Eur J Pharmacol. 1995; 273(1-2):63-71. 3. Ishizuka et al., Neurosci Lett. 2003; 339(2):143-6. 4. Ferraro et al., Neurosci Lett. 1998; 253(2):135-8 5. Perez de la Mora et al., Neurosci Lett. 1999; 259(3):181-5.
2. increases histamine in TMN (indirectly)3. increases extracellular glutamate4 (also indirectly5) 1. Wise et al., Sleep, 2007; 30(12): Tanganelli et al., Eur J Pharmacol. 1995; 273(1-2): Ishizuka et al., Neurosci Lett. 2003; 339(2): Ferraro et al., Neurosci Lett. 1998; 253(2): Perez de la Mora et al., Neurosci Lett. 1999; 259(3):")
49
Sleeping and waking – what goes wrong
insomnia not enough sleep or sleep of poor quality hypersomnia excessive daytime sleepiness parasomnia unusual happenings in the night other, eg: circadian rhythm disorders restless legs syndrome Full classification in ICSD (2001) International Classification of Sleep Disorders - Diagnostic and Coding Manual, American Academy of Sleep Medicine, Chicago.
 International Classification of Sleep Disorders - Diagnostic and Coding Manual, American Academy of Sleep Medicine, Chicago.")
50
Parasomnias Non-REM sleep REM sleep Night terrors
Sleepwalking Confusional arousals Bruxism Enuresis Sleep starts Sleep talking Head-banging REM sleep REM sleep behaviour disorder (RBD) Sleep paralysis Nightmares
 Sleep paralysis. Nightmares.")
51
Night terrors and sleepwalking
Usually strong family and childhood history Night terrors recurrent episodes of abrupt awakening, usually in first third of night, usually with a scream intense fear and signs of autonomic arousal unresponsiveness to comforting no detailed recall cause significant distress incidence ~ 2% adults Sleep walking rare to present for treatment unless injured self or others similar course to night terrors, often both in same subject

52
Nightmares associated with psychotropic medications
cholinesterase inhibitors beta-blockers SSRIs esp paroxetine levodopa GHB

53
Treatment of nightmares
Psychological treatments effective (1b) focus on guided imagery, pleasant images exposure - writing down dreams changing the ‘ending’ A few case series show beneficial effects of the alpha-1 adrenergic blocker prazosin in reducing nightmares related to PTSD in both military and civilian settings 1 Raskind et al, Biol Psychiatry. 2007; 61(8):928-34
 focus on guided imagery, pleasant images. exposure - writing down dreams. changing the ‘ending’ A few case series show beneficial effects of the alpha-1 adrenergic blocker prazosin in reducing nightmares related to PTSD in both military and civilian settings 1. Raskind et al, Biol Psychiatry. 2007; 61(8):")
54
REM behaviour disorder
Violent complex behaviour at night Subject recall 80-90% 2 abnormalities lack of atonia during REM sleep increased vividness and/or nasty content of dreams

55
REM behaviour disorder
Incidence unknown (prob <1%), identified in 1980s, increasingly recognised Older age group, steady rise after 55 Idiopathic or associated with Parkinson’s disease (~50% of PD pts) , Lewy body dementia (~70%) , multiple system atrophy (>90%) RBD may be the first manifestation of these disorders, antedating the onset of parkinsonism, cerebellar syndrome, dysautonomia, and dementia by several years. M >> F (80-90% male except for those with MSA)
, identified in 1980s, increasingly recognised. Older age group, steady rise after 55. Idiopathic or associated with Parkinson’s disease (~50% of PD pts) , Lewy body dementia (~70%) , multiple system atrophy (>90%) RBD may be the first manifestation of these disorders, antedating the onset of parkinsonism, cerebellar syndrome, dysautonomia, and dementia by several years. M >> F (80-90% male except for those with MSA)")
56
Drugs which probably provoke symptoms of RBD
all SSRIs venlafaxine mirtazapine imipramine, clomipramine (only reported in narcoleptic patients with RBD) bisoprolol tramadol
 bisoprolol. tramadol.")
57
Drugs that relieve symptoms of RBD
No prospective or controlled studies Evidence based on case series (level IV) drug No of patients Very effective Partially effective No effect Side effects clonazepam 1-4mg 67 79% 11% 10% ? 38 55% 32% 13% 35% 110 82% 17% 1% 25% melatonin 3 -12mg 6 N=5 N=1 15 N=3 N=10 N=2 14 N=6 N=4
 drug. No of patients. Very effective. Partially effective. No effect. Side effects. clonazepam 1-4mg % 11% 10% % 32% 13% 35% % 17% 1% 25% melatonin 3 -12mg. 6. N=5. N= N=3. N=10. N= N=6. N=4.")
58
Sleep paralysis Intrusion of REM atonia (and sometimes dream imagery) into awake state Isolated prevalence ~3% (?) lifetime, unknown current, 20% in panic disorder and GAD May be genetically determined Exacerbated by irregular sleep routine /sleep deprivation alcohol anxiety / tension
 lifetime, unknown current, 20% in panic disorder and GAD. May be genetically determined. Exacerbated by. irregular sleep routine /sleep deprivation. alcohol. anxiety / tension.")
59
Treatment of sleep paralysis
No proven treatment Clinical experience: improved by better sleep hygiene (inc. alcohol) reduced anxiety practical strategies for signalling to partner - sensory input stops it
 reduced anxiety. practical strategies for signalling to partner - sensory input stops it.")
60
Sleeping and waking – what goes wrong
insomnia not enough sleep or sleep of poor quality hypersomnia excessive daytime sleepiness parasomnia unusual happenings in the night other, eg: circadian rhythm disorders restless legs syndrome Full classification in ICSD (2001) International Classification of Sleep Disorders - Diagnostic and Coding Manual, American Academy of Sleep Medicine, Chicago.
 International Classification of Sleep Disorders - Diagnostic and Coding Manual, American Academy of Sleep Medicine, Chicago.")
61
Circadian rhythm disorders
Sleep disorders where there is a mismatch between circadian rhythms and required sleep-wake cycle sleeplessness when trying to sleep at a time not signalled by the internal clock excessive sleepiness when needing to be awake Some circadian disorders (jetlag and shift work disorder) are due to an individual lifestyle, including work and travel schedules, that conflicts with the internal clock. Others are: delayed sleep phase syndrome: difficulty falling asleep till early hours and preferred late waking up time free running sleep disorder where there is a daily increment of sleep and wake times (getting later each day). Much rarer – advanced sleep phase syndrome 61
 are due to an individual lifestyle, including work and travel schedules, that conflicts with the internal clock. Others are: delayed sleep phase syndrome: difficulty falling asleep till early hours and preferred late waking up time. free running sleep disorder where there is a daily increment of sleep and wake times (getting later each day). Much rarer. – advanced sleep phase syndrome. 61.")
62
Restless legs syndrome
(i) an urge to move the legs, usually accompanied or caused by uncomfortable and unpleasant sensations in the legs; (ii) the urge to move or unpleasant sensations begin or worsen during periods of rest or inactivity such as lying or sitting (iii) the urge to move or unpleasant sensations are partially or totally relieved by movement, such as walking or stretching, at least as long as the activity continues; (iv) the urge to move or unpleasant sensations are worse in the evening or night than during the day or only occur in the evening or night. (There may also be periodic limb movements in sleep - stereotyped jerks of legs or less often arms, occurring every seconds during sleep and sometimes causing arousal from sleep) 62
 an urge to move the legs, usually accompanied or caused by uncomfortable and unpleasant sensations in the legs; (ii) the urge to move or unpleasant sensations begin or worsen during periods of rest or inactivity such as lying or sitting. (iii) the urge to move or unpleasant sensations are partially or totally relieved by movement, such as walking or stretching, at least as long as the activity continues; (iv) the urge to move or unpleasant sensations are worse in the evening or night than during the day or only occur in the evening or night. (There may also be periodic limb movements in sleep - stereotyped jerks of legs or less often arms, occurring every seconds during sleep and sometimes causing arousal from sleep) 62.")
Similar presentations




>")



, Assoc MAPS>")

 Necessary for Physical and Mental Health $50 Billion / Year in Lost Productivity Occupies 1/3 of our Lives.>")









