Download presentation
Presentation is loading. Please wait.

1
Practical Tips in β-blocker Therapy in CHF β-blocker Therapy in CHF CMCC 11 th 11 th September 2009 Rungsrit Kanjanavanit MD. Cardiovascular Div. Dept. of Medicine Faculty of Medicine, Chiang Mai Univ.

2
Circulation. 2009;119:1977-2016.

3
2551

4
βBβB / ARB

5
Utilization of HF medications in clinical practice Euro Heart Survey Komajda M et al. Eur Heart J 2003 %

6
Trials excluded patients with relative contraindications Not very old, mainly white men, no complicated medical history In real life, more than 75% have at least one relative contraindication Clinical trials VS Real world population

7
Co-morbidities CMU HF clinic 44.4 % had > 3 comorbidities

8
Not adhering to guidelines Can the difference between the real world patients and RCT’s solely explain these findings? No

9
83% of SOLVD-eligible were on ACEI Almost half of these received the target dose as recommended in the guidelines 54% of MERIT-HF-eligible were on β-blockers 10% of these received the target dose. 43% of RALES-eligible patients were on aldosterone antagonist Euro Heart Survey on Heart Failure Lenzen MJ et al. European Heart Journal (2005) 26, 2706–2713 ‘adherence’ related solely to physicians following guidelines, not to patient compliance or persistence.
 26, 2706–2713 ‘adherence’ related solely to physicians following guidelines, not to patient compliance or persistence..")
10
Barrier to β-blocker prescription Uninformed clinicians Perceived complexity in initiation and up-titration Lack of time and expertise for “micromanagement” required with complex regimen Risk of intolerance and worsening of HF symptoms with initiation Perceived delay in beneficial effects on outcomes Economic restraints – in some hospital,UC may not cover evidenced-based β-blocker for HF

11
1. Enalapril (20) ½ tab bid pc. 2. Bisoprolol (5) 1 tab OD. 3. Spironolactone (25) 1 tab OD. 4. Digoxin (0.25) ½ tab E.O.D. 5. Furosemide (40) 1 tab prn for dyspnea,edema or weight gain > 1 kg in 2 days 13. Warfarin (3) ½ tab o OD. Except Mon. and Wed. 14.Warfarin (5) ½ tab o OD. Only on Mon. and Wed. 6. Glibencarmide(5) 1½ tab bid ac 7. Metformin (500) 1 tab tid pc 8. Aspirin (300) 1 tab OD. 9. ISDN (10) 2 tab tid ac 10. Isordil (5) 1 tab SL prn 11. Amlodipine (10) 1 tab OD. 15.Lorazepam 1 tab prn hs. 16.Senekot 2 tab o hs 12. Atrovastatin (20) 1 tab pc evening Drugs Prescriptions of Mr. Had-enough POLYPHARMACY 17. Omeprazole (20) 1 tab o OD
 1 tab OD. 4. Digoxin (0.25) ½ tab E.O.D. 5. Furosemide (40) 1 tab prn for dyspnea,edema or weight gain > 1 kg in 2 days 13. Warfarin (3) ½ tab o OD. Except Mon. and Wed. 14.Warfarin (5) ½ tab o OD. Only on Mon. and Wed. 6. Glibencarmide(5) 1½ tab bid ac 7. Metformin (500) 1 tab tid pc 8. Aspirin (300) 1 tab OD. 9. ISDN (10) 2 tab tid ac 10. Isordil (5) 1 tab SL prn 11. Amlodipine (10) 1 tab OD. 15.Lorazepam 1 tab prn hs. 16.Senekot 2 tab o hs 12. Atrovastatin (20) 1 tab pc evening Drugs Prescriptions of Mr. Had-enough POLYPHARMACY 17. Omeprazole (20) 1 tab o OD.")
12
Patients with Sys HF

13
Patients with Sys HF without contraindication to β -blocker

14
Patients with Sys HF who are given β -blocker ( Doctor adherence to guideline)
")
15
Patients with Sys HF who are actually taking β -blocker ( Patients’ medical adherence )
")
16
Patients with Sys HF who are taking β - blocker at the target dose

17
We can do better !

18
β blocker in heart failure Contra-indication Strong indication

19
Tip # 1 Implementation of β blocker therapy -When? A simplified criteria 1. Edema free 2. Not requiring intravenous medication for HF

20
Which and what dose Starting dose(mg)Target dose(mg) Bisoprolol1.25 od10 od Metroprolol CR/XL12.5-25 od200 od Carvedilol3.125 bid25-50 bid Nebivolol1.25 od10 od Titration period – weeks to months
Target dose(mg) Bisoprolol1.25 od10 od Metroprolol CR/XL od200 od Carvedilol3.125 bid25-50 bid Nebivolol1.25 od10 od Titration period – weeks to months")
21
Tip # 2 How to use β blocker Start early but with low dose Double dose at not less than 2 weekly interval Aim for target dose or highest tolerated dose Some β blocker is better than no β blocker Monitor HR,BP,BW and signs of congestion Check blood chemistry 1-2 week after inhibition and 1-2 week after final dose titration

22
Dry and Warm Wet and Warm Dry and Cold Wet and Cold Fluid status Perfusion Dry Wet Warm Cold

23
Tip # 3 Patient came in with decompensated HF What to do Wet and warm IV diuretics No need to decrease dose of β-blocker Up-titrate dose of ACEi and β-blocker when stabilized Wet and cold Positive inotropic support (PDE inhibitors) Decrease the dose of β-blocker by 50% Reintroduction or up-titrate β-blocker when stabilized
 Decrease the dose of β-blocker by 50% Reintroduction or up-titrate β-blocker when stabilized")
24
B-CONVINCED Beta-blocker CONtinuation Vs. INterrupion in patients with Congestive heart failure hospitalizED for a decompensation episode EHJ (2009) 30,1-7 During ADHF, continuation of β-blocker is not associated with delayed or lesser improvement, but with higher rate of chronic prescription of β-blocker therapy after 3 months Keep β-blocker Stop β-blocker ADHF 69 78 HF improves at Day 3 92.8 % 92.3 % β-blocker at 3 months 90 % 76 % Plasma BNP, LOS, rehospitalization rate, death rate also similar
 30,1-7 During ADHF, continuation of β-blocker is not associated with delayed or lesser improvement, but with higher rate of chronic prescription of β-blocker therapy after 3 months Keep β-blocker Stop β-blocker ADHF HF improves at Day % 92.3 % β-blocker at 3 months 90 % 76 % Plasma BNP, LOS, rehospitalization rate, death rate also similar.")
25
Tip # 4 How to use Diuretics Lower the dose or stop before initiation of ACEi and spironolactone (avoid hypovolemia ) Increase the dose before initiation of β- blocker ( make sure there is no fluid retention )
 Increase the dose before initiation of β- blocker ( make sure there is no fluid retention )")
26
The most important tool in HF management Self daily weight monitoring : If weight increases > 1 kg within 1 or 2 days If weight increases > 1 kg within 1 or 2 days double the dose of diuretics, until returns to ideal BW double the dose of diuretics, until returns to ideal BW Weigh every morning Weigh every morning After going to toilet After going to toilet Before getting dressed Before getting dressed Before breakfast Before breakfast

27
Tip # 5 Dealing with low heart rate If < 50 bpm, halve dose of β-blocker Review other medications Drug interaction to look for : Digitalis Verapamil / diltiazem - should be discontinue Amiodarone

28
Tips # 6 Be persistant ! Minor setback can be overcome Any general sense of un-wellness will generally resolve in a few week More than 85% will tolerate β blocker

29
Tip # 7 Problem solving : Hypotension Asymptomatic low BP does not require any change in therapy. HypoPERFUSION not hypoTENSION is the concern. Dizziness,light-headedness and confusion D/C nitrates, CCB, other vasodilators reducing dose of the diuretics if no signs/symptoms of congestion

30
Tip # 8 Always measure supine and upright BP in every HF patients at every visit

31
Case ผู้ป่วยชาย อายุ 21 ปี ได้รับการวินิจฉัยเป็น DCM มาติดตามการรักษาหลังออกจาก โรงพยาบาลอาการดีขึ้น จาก NYHA III เป็น II ตรวจร่างกาย : HR 100 bpm BP 100/60 mmHg No lung crepitation No edema ผลการตรวจห้องปฏิบัติการ serum Cr 1.3 mg/dl, K 4.0 mg/dl การรักษาที่ได้รับ Ramipril 2.5mg/d Furosemide 40mg/d Digoxin 0.125mg/d

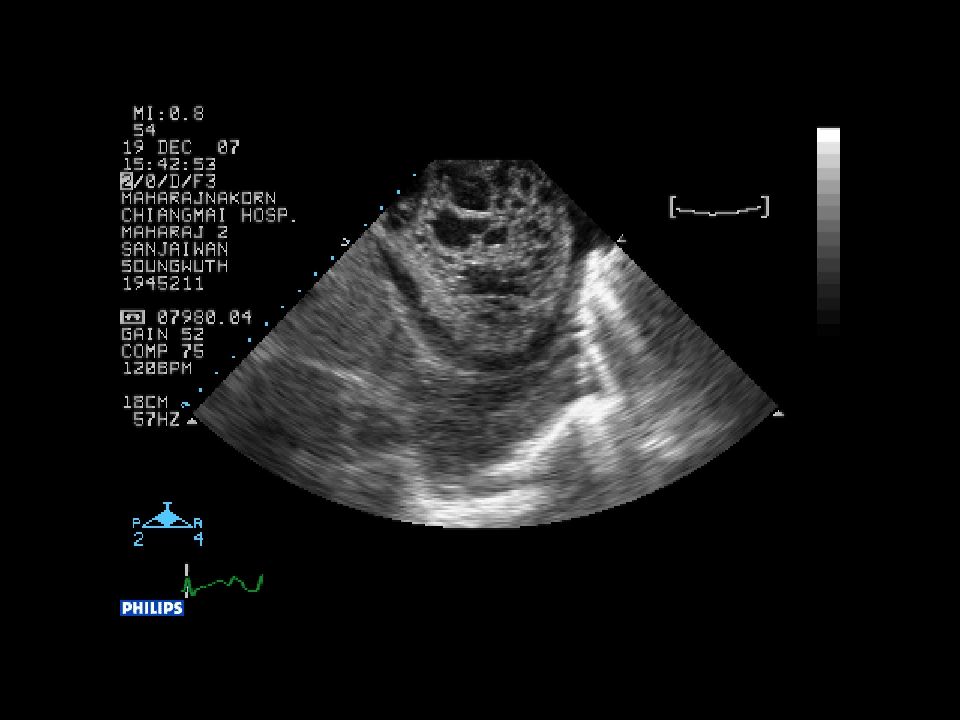
34
LV & RV Non-compaction

35
What would you do? 1. Increase dose of ramipril (target dose 10mg/d) 2. Add very low dose β-blocker 3. Increase dose of digoxin (to control HR) 4. Leave him with this regimen (now asymptomatic)
 4. Leave him with this regimen (now asymptomatic).")
36
ATLAS (Assessment of Treatment with Lisinopril and Survival) 3164pt. NYHA II-IV, LV EF <30% F/U 45.7mo Low (2.5-5.0mg) High (32.5-35mg) Mortality (%) 44.9 42.5 CV mortality (%) 40.2 37.2 Hospitalization (no.)* 4327 3819 HF hospitalization(no)* 1576 1999 Circ.1999;100:2312-2318 ATLAS : low dose VS high dose NNT to avoid rehospitalization = 4
 High ( mg) Mortality (%) CV mortality (%) Hospitalization (no.)* HF hospitalization(no)* Circ.1999;100: ATLAS : low dose VS high dose NNT to avoid rehospitalization = 4.")
37
LVESVI: Change From Baseline * P < 0.05, ** P < 0.001 EnalaprilCarvedilol-10 -8 -6 -4 -2 0 2 4 ****** *** LVESVI (ml/m 2 ) M6 M12 M18M6 M18 M12 M6 M12M18 Carvedilol & Enalapril CARMEN Study
 M6 M12 M18M6 M18 M12 M6 M12M18 Carvedilol & Enalapril CARMEN Study")
38
LVEF: Change From Baseline * P < 0.05; ** P < 0.01; *** P < 0.001 Enalapril Carvedilol & Enalapril Carvedilol 0 1 2 3 4 5 LVEF (%) ********* ******** * M6 M12 M18M6 M18 M12 M6 M12M18 CARMEN Study
 ********* ******** * M6 M12 M18M6 M18 M12 M6 M12M18 CARMEN Study")
39
Comparing two different strategies in patients receiving low dose ACEi Increasing ACEi to maximal doses Adding β-blocker Effect on symptoms No change Improved Effect on risk of death 8% reduction 30-40% reduction Effect on risk of death and hospitalization 12% reduction 20-40% reduction ATLAS MERIT HF

40
Combined use of low doses of several drugs is preferred to a large dose of a single agent. Tip # 9

41
Six patterns of taking medication among patients treated for chronic illnesses who continue to take their medications 1/6 N Engl J Med 2005;353:487-97

42
“ Good drugs do not work on patients who do not take them ” C. Everett Koop, M.D. Tip # 10 Fact

43
Inadequate education poor self-motivation poor compliance forgetfulness poor family support drugs side effect Complexity of the medication regimen Excessive cost Depression

44
Patient education Self management Heart transplant Revascularization Resynchronization Therapy Pharmacologic Therapy “ filling the in the care of chronic diseases ” Disease management program Low tech – high touch therapy G A P Pyramid of HF care

45
10 Practical Tips - Summary 1. A simplified criteria when to start 2. How to titrate and what to monitor 3. Do not stop blocker when patients come in with ADHF unless inotropes is needed (low output syndrome) 4. Know how to use diuretics effectively 1. Flexible regimen 2. Dealing with diuretic resistance
 4. Know how to use diuretics effectively 1. Flexible regimen 2. Dealing with diuretic resistance.")
46
10 Practical Tips - Summary 5. Dealing with low heart rate 6. Be persistent 7. Hypotension VS hypoperfusion 8. Measure both supine and upright BP in every HF patients at every visit 9. Combined use of low to moderate doses of several drugs is preferred to a large dose of a single agent 10. Nurses are doctor’s best friend

47
Thank you

Similar presentations


:>")
 trial.>")


>")








>")



 inhibitors ARBs (angiotensin receptor blockers) Beta-blockers Spironolactone Diuretics (water.>")
