Download presentation
Presentation is loading. Please wait.

3
Response to questions Laboratory tests Ophthalmic test Ophthalmic treatments Prognosis How to fallow up

4
CRVO EVALUATION SYSTEMIC VASCULAR DISEASE:diabetes mellitus Hypertension, carotid insufficincy. OCULAR DISEASES:open angle glacuma, Ischmic optic neuropathy,pseudotumor cerebri Tilted optic nerve head,optic nerve head drusen HEMATOLOGIC ALTERATION:hyperviscosity Multiple myeloma,blood dyscrasias,anemia&… INFLAMMATORY/AUTOIMMUNE VASCULITIS: SLE MEDICATIONS:oral contraceptives,duretics, Hepatitis B vaccine, INFECTIOUS VASCULITIS:HIV,syphilis,herpes zoster OTHER:retrobulbar block,dehydration,pregnancy

5
CRVO EVALUATION SYSTEMIC WORKUP is not indicated in person older than60 years of age with known systemic Vascular risk factors for CRVO. younger patient are more likely to have predispo- Ing conditions resulting in thrombotic disease. A limited systemic workup may be considered in those with prior occlusion in the fellow eye, prior systemic thrombotic disease,family history of thrombosis,hematologic or rheumatologic.

6
CRVO EVALUATION:LAB.tests CBC,ESR,FBS,ANA,ANTIPHOSPHOLIPID Ab fasting plasma homocysteine level. In bilateral,simaltaneous CRVO or mixed-type retinal vascular occlusions should have detailed evaluation for a hypercogulable condition, as these persons may be at risk for future,non-Ocular thrombotic events.

7
OPHTHALMIC TEST IN CRVO Wide-angle FA 30 second after Iv injection of Sodium fluorescein. classification:perfused[less than 10 disc areas of capillary nonperfusion]non perfused[10 or more disc areas of retinal capillary nonperfusion] indeterminate [intraretinal hemorrhage prevent angiographic determination of perfusion status]. OCT

10
THERAPEUTIC OPTIONS IN CRVO MACULAR EDEMA Observation Corticosteroid therapy Intravitreal anti-VEGF therapy NEOVASCULARIZATION Laser photocoagulation Medical therapy ALTERNATIVE TREATMEHTS Chorioretinal venous anastomosis Tissue plasminogen activator Surgical treatments:vitrectomy,radial optic neurotomy,

11
MACULAR EDEMA OBSERVATION Widespread damage to the perifovealcapillary netwrk has been hypothesized to contribute to the lack of visual recovery.

13
MACULAR EDEMA CORTICOSTEROID THERAPY It is believed that corticosteroid maintain anti-Inflammatory effects with modulation of production of cytokines and growth factor including VEGF.steroid are also stabilize blood retinal barrier with reduction in vascular permeability. Eyes were treated with 1-mg IVTA every 4month for 1 year and observed significant improvement in visual acuity compared to observation. Primary ocular advers events included cataract formation and elevated Intraocular pressure. In chronic refractory CME sustained –release intravitreal dexamethasone delivery system,OZURDEX,was approved.

14
MACULAR EDEMA Intravitreal anti-VEGF therapy Combined anti-VEGF and corticosteroid

15
OCULAR NEOVASCULARIZATION Laser phothcoagulation CVOS recommended that PRP be delivered promptly after the development of NVI/NVA but not in eyes with nonperfused crvo. Prophylactic PRP may be done in special risk factors for developing NVI/NVA[male gender, short duration of CRVO,extensive retinal nonperusion,and extensive retinal hemorrhage]

16
Optociliary shunt

17
SYSTEMIC MEDICAL CONDITION Treatment of systemic vascular risk factors, coordination with the internist is strongly recommended Systemic anticoagulation such as asprin or heparin,cannot prevent or alter the natural history of CRVO but may help prevent nonocular thrombotic events,especially in individuals with known systemic vascular disease. Oral pentoxifylline is a potent vasodilator usedin systemic vascular diseases to improve perfusionto occluded vessels and enhance the development ofcollateral circulation.this drug reduct macular thickening but not change in VA or perfusion status. Hemodilation increased oxigen supply to the retina. Hemodilution is likely not appropriate for patient with anemia,renal insufficiency,or pulmonary insuffcieny.

18
Response to questions BRVO Laboratory tests Ophthalmic test Ophthalmic treatments Prognosis How to fallow up

19
BRVO EVALUATION Systemic vascular diseases such as aterioscleros Diabetis,smoking,hyperlipidemia,glaucoma, and ocular inflammatory disease. antiphosphlipid AB,elevated plasma homocystein level and low serum folate. Short axial length In bilateral cases or cases involving young patients,systemic manifestation of infectious disease,inflammatory or autoimmune condition, neoplasm,or hypercoagulable states may be present.

20
DIAGNOSTIC WORKUP PARTICULAR ATTENTION to the history of glaucoma and sign of intraocular inflammation IN YOUNG:CBC,FBS,prothrombin time/partial thromboplastin time,lipid panel,homocysteine anticardiolipin AB,protein C/S IN OLDER than 60,additional workup isnot necessary since the majority are idiopathic or due to hypertension or atherosclerosis.

21
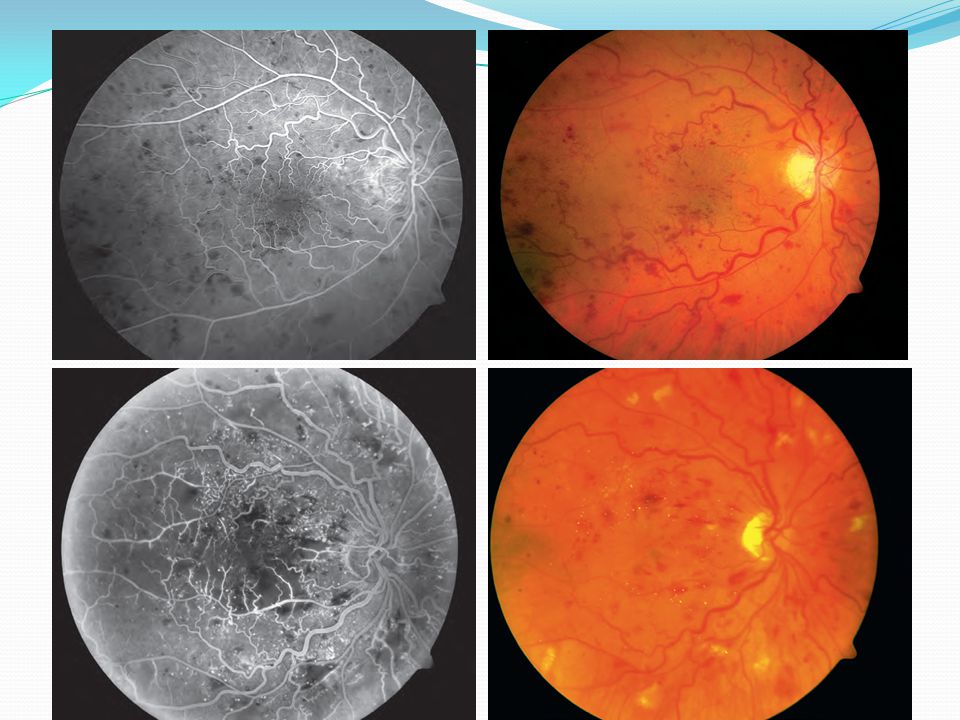
OPHTHALMIC TEST F/A For delineate the retinal vascular caharacteristic That may have prognostic significance :macular Leakage and edema,macular ischemia,and large Segments of capillary nonperfusion that may Portend neovascularization[ischemic BRVO>5 disc diameters nonperfusion] In chronic cases,when the hemorrhages have resolved,microvascular changes on F/Amay provide the only clues of a previous BRVO. When we have leakage and edema with cystoid involvement of the fovea,but no capillary nonperfusion, the macular edema is the cause of vision loss. when macular edema is present within the first6 month after a BRVO and there is little or no leakage on F/A,macular ischemia may be the cause of the macular edema and almost always spontaneously resorbs in the first year after occlusion,often with return of vision. OCT Used to monitor the response to treatment of macular edema and has been used in Place of F/A in some treatment trials for BRVO.
![OPHTHALMIC TEST F/A For delineate the retinal vascular caharacteristic That may have prognostic significance :macular Leakage and edema,macular ischemia,and large Segments of capillary nonperfusion that may Portend neovascularization[ischemic BRVO>5 disc diameters nonperfusion] In chronic cases,when the hemorrhages have resolved,microvascular changes on F/Amay provide the only clues of a previous BRVO.](http://images.slideplayer.com/12/3450827/slides/slide_21.jpg "When we have leakage and edema with cystoid involvement of the fovea,but no capillary nonperfusion, the macular edema is the cause of vision loss. when macular edema is present within the first6 month after a BRVO and there is little or no leakage on F/A,macular ischemia may be the cause of the macular edema and almost always spontaneously resorbs in the first year after occlusion,often with return of vision. OCT Used to monitor the response to treatment of macular edema and has been used in Place of F/A in some treatment trials for BRVO..")
22
Chronic case of BRVO

24
TREATMENT OPTIONS IN BRVO MEDICAL TREATMENT LASER TREATMENT STEROID TREATMENT ANTI-VEGF TREATMENT FAVOR[ILUVIEN] STUDY SURGICAL MANAGEMENT[vitrectomy with or Without sheathotomy]
![TREATMENT OPTIONS IN BRVO MEDICAL TREATMENT LASER TREATMENT STEROID TREATMENT ANTI-VEGF TREATMENT FAVOR[ILUVIEN] STUDY SURGICAL MANAGEMENT[vitrectomy with or Without sheathotomy]](http://images.slideplayer.com/12/3450827/slides/slide_24.jpg "TREATMENT OPTIONS IN BRVO MEDICAL TREATMENT LASER TREATMENT STEROID TREATMENT ANTI-VEGF TREATMENT FAVOR[ILUVIEN] STUDY SURGICAL MANAGEMENT[vitrectomy with or Without sheathotomy]")
25
Medical treatment In most cases anticoagulant therapy has not been shown to be beneficial in either the prevention or the management of BRVO.Since thes systemic administration of anticoagulants can be associated with systemic complication, and could,in theory,increase the severity of intraretinal hemorrhage occurring in the acute phase,such therapy is not recommended.

26
Laser treatment

27
Steroid treatment Triamcinolone Corticosteroid inhibit the expression of VEGF and reduce macular edema.Significant side-effects,including cataract and Glaucoma. 1mg IVTA every 4 months reduced macular edema but not recommended as first –line therapy and considered in patients where macular grid laser or other therapies are ineffective,as the treatment was found to be relatively safe,especially in pseudophakic eyes. Dexamethasone implant. FAVOR[ILUVIEN] sustained-release non-erodable,intravitreal implant for patients with macular edema due to BRVOorCRVO of>3 months,duration in phase 2 trial.

28
prognosis BRVO:1/3 to1/2 of patients have return of vision to 20/40 or better without any therapy. 31-41 ℅ of patients with ischemic BRVO developed neovascularization or vitreous hemmorrhage,compared with11 ℅ of patients With nonischemic BRVO.decreased vision for over 1 year as a result of macular edema are much less likely to regain vision spontaneously. When macular edema is present within the first 6 months after a BRVO and there is little or no leakage on FA,macular ischemia may be the cause of the macular edema.this edema always resorbs in the first year after the occlusion, often with return of vision.

29
CRVO prognosis A perfused CRVO have better initial and final VA A nonperfused CRVO have poor VA and large areas of retinal capillary nonperfusion were significant factors associated with an increased risk of developing NVI/NVA. Initial VA was highly correlated with degree of nonperfusion and prognosis.

30
Follow up In CRVO eye with initial acuity of 20/40 or better were generally examined every1-2 MO for 6 MO,then annually if stable. Eye with initial acuity worse than 20/200 were Seen monthly for the initial 6 MO,then bimonthly For the next 6 MO. Eyes with 20/50 and20/200 have an intermediate risk of developing NVI/NVA and were also typically examined monthly for the first 6 MO.

31
BRVO FOLLOW UP In BRVO initially,patents followed closely every MO or2 MO for macular edema and/or NVE. Once macular edema stabilized or resolved interval can be extended to 3-6 MO or even longer for stable chonic cases. Patients with previously untreated retinal nonperfusion >5disc diameters followd at closer intervals[3 months]due to the increased risk for neovascular complication.

Similar presentations






 Waxman MD PhD>")



 for Macular Edema Secondary to Central Retinal Vein Occlusion Mahmood J Showail.>")


 Giovanni Caboto Club October 3, 2012>")



Observation occult CNV also requires close follow – up.every 3 month 2) Laser coagulation 3) Surgery.>")






