Download presentation
Presentation is loading. Please wait.

1
Management conference Middle age man with nephrotic syndrome, ascitis and edema
Raika Jamali MD Digestive Disease Research Center Tehran University of Medical Sciences

2
A 49 years old man with progressive bilateral pedal edema and ascitis from 1 month ago.
History of DM for 4 years. Three months ago during the evaluation for excessive proteinuria inappropriate for diabetic nephropathy ,prolongation of PT was detected before kidney biopsy. Viral markers requested and was referred for liver function evaluation.

3
EXAM Vital signs were stable. No fever.
Mild anemia. Ichterus in sclera. Parallel collaterals in chest and upper abdomen which filled upward. Tense ascitis. liver span 14 cm. Moderate splenomegaly . No signs of chronic liver disease. Bilateral pedal edema.

7
WBC=6500 HB=10 PLT=245000 MCV=85 FBS=180 TG=200 AFP =60,92 AST=52 ALT=43 Bili T=5 Bili D=1.3 ALP=508 PT(INR)=2.6 PTT=38 Albumin=2.2 Protein=5.2
=2.6 PTT=38 Albumin=2.2 Protein=5.2.")
8
BUN=15 Cr=0.9 Uric Acid=4 U/A: 3+ protein 24 h urine protein: 7 gr /day

9
HCV Ab=suspicious HBs Ag=Neg HBs Ab=positive HBc Ab=positive HBV DNA and HCV RNA Titer : undetectable

10
Ascitic fluid RBC=20 WBC=70 Albumin=0.5
Cytology=negative for malignancy

11
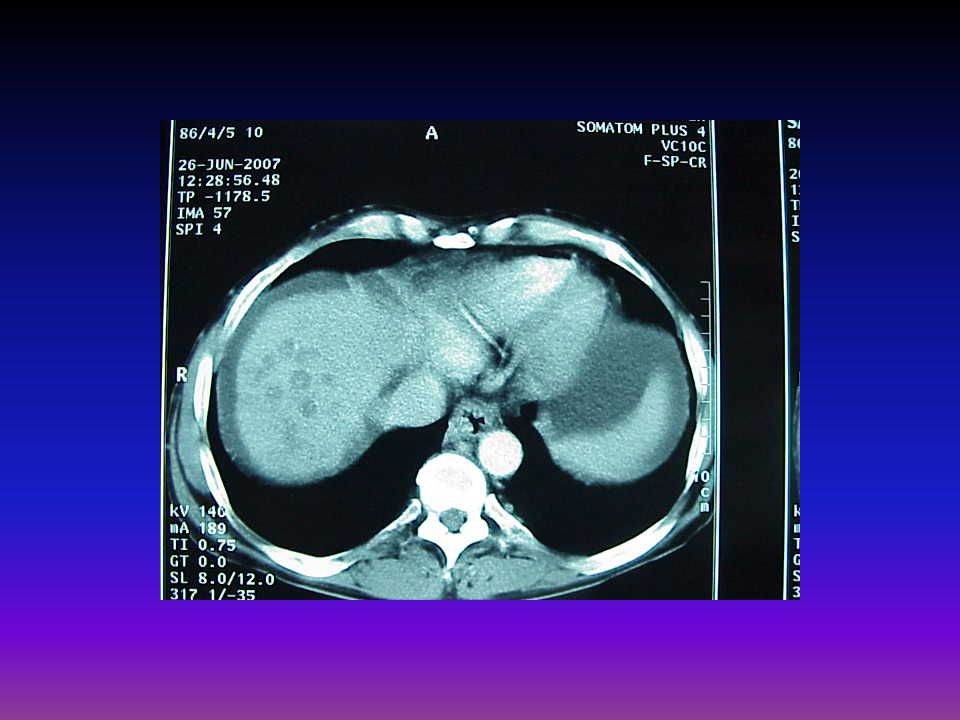
Sonography Liver was enlarged with hetrogenous echo pattern.
PV diameter 10 mm. Severe ascitis. Moderate splenomrgaly.

12
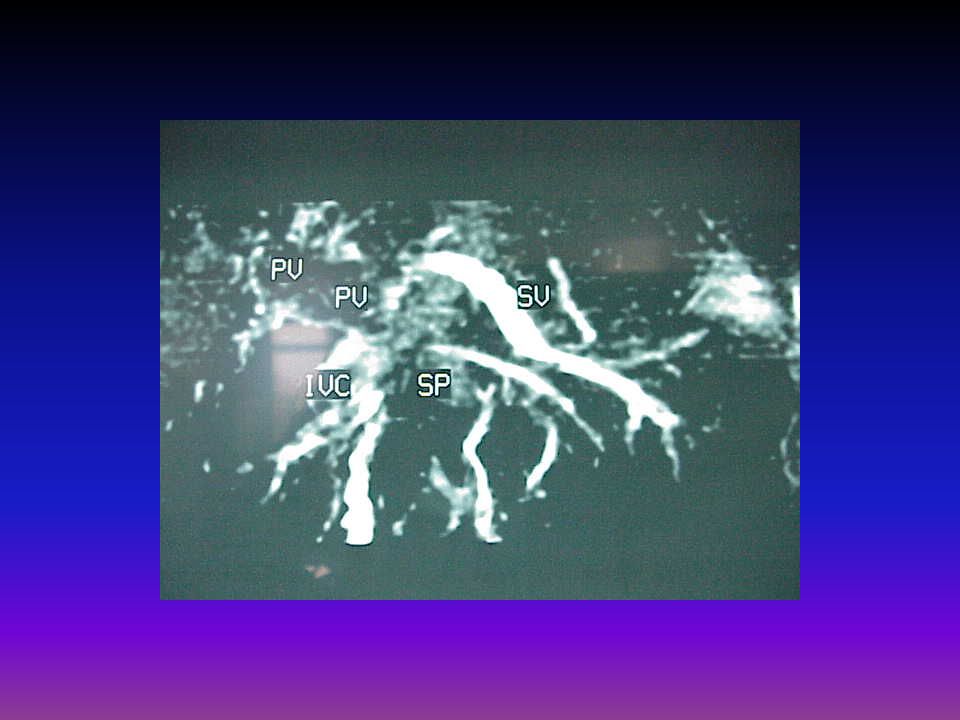
Color Doppler sonography
IVC and suprahepatic veins were occluded. Portal vein was occluded with collaterals in hilum. Renal veins were thrombosed. Splenic vein was patent.

13
Activated protein C resistance: 221(120)
B2 micro globulin : 10 (0-3) Anti cardiolipin Ab: normal Anti phospholipids Ab: normal Pr C: reduced Pr S: reduced Anti thrombin 3: normal homocysteine: normal Ham, sucrose test: normal CD 55,59: normal
 Anti cardiolipin Ab: normal. Anti phospholipids Ab: normal. Pr C: reduced. Pr S: reduced. Anti thrombin 3: normal. homocysteine: normal. Ham, sucrose test: normal. CD 55,59: normal.")
14
Endoscopy Fundal and esophageal varices were seen.
Snake skin appearance in fundus and body.

24
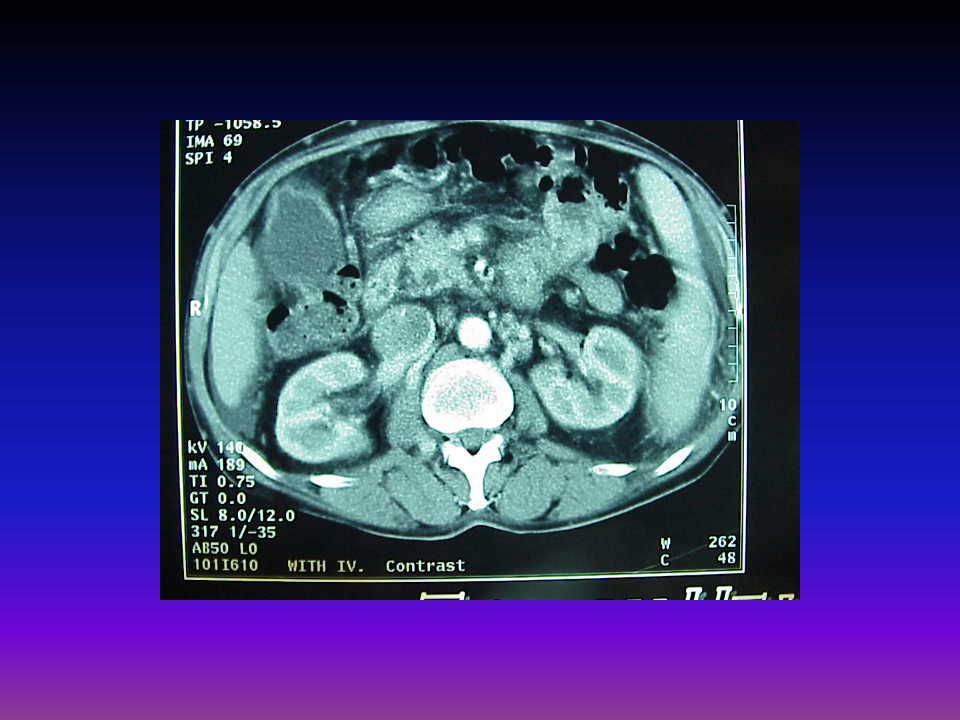
mottled appearance to the underperfused liver with collapsed portal veins,
ascites (small arrows) extensive retroperitoneal varices (large arrow). enlarged caudate lobe of the liver (large arrowhead) the collapsed small IVC (small arrowhead).
 extensive retroperitoneal varices (large arrow). enlarged caudate lobe of the liver (large arrowhead) the collapsed small IVC (small arrowhead).")
30
Follow Up The patient was treated with diuretic and concomitant albumin. Several abdominal paracentesis were performed. Heparin started and switched to warfarin. Proteinuria decreased during F/U. Ascitis and edema is partially controlled with diuretic. Hypercoagulability states were checked again which showed normal results.

31
Budd-Chiari syndrome more common in women third or fourth decade
most common symptoms is ascites (84%) and hepatomegaly (76%) obstruction was in the hepatic veins (62%) inferior vena cava (7%) portal vein thrombosis (14%) myeloproliferative disorder was present in 23% (polycythemia vera).
 and hepatomegaly (76%) obstruction was in the hepatic veins (62%) inferior vena cava (7%) portal vein thrombosis (14%) myeloproliferative disorder was present in 23% (polycythemia vera).")
32
Major causes of the Budd-Chiari syndrome
Myeloproliferative diseases Malignancy (Hepatocellular carcinoma) Infections and benign lesions of the liver Oral contraceptives Pregnancy Hypercoagulable Behcet's disease Membranous webs of IVC Idiopathic
 Infections and benign lesions of the liver. Oral contraceptives. Pregnancy. Hypercoagulable. Behcet s disease. Membranous webs of IVC. Idiopathic.")
33
Acute (20%) : (2% with fulminant hepatic failure) Subacute (40%): (having signs or symptoms for < 6 months and no evidence of cirrhosis) Chronic (40%): (having signs or symptoms for > 6 months with evidence of cirrhosis)
: (having signs or symptoms for > 6 months with evidence of cirrhosis)")
34
Acute most commonly in women (during pregnancy ) pain and hepatomegaly
Jaundice and ascites develop rapidly Liver function can deteriorate quickly, leading to hepatic encephalopathy DDx: ischemic, viral, malignant/infiltrative, and toxic hepatitis

35
Subacute and chronic disease
clinical manifestations depend upon the extent of occlusion, and the recruitment of collateral circulation. Chronic occlusion of the hepatic veins may be associated with hypertrophy of the caudate lobe. This cause compression of the intrahepatic portion of the IVC, leading to lower extremity edema

37
cirrhosis may develop in the chronically congested liver, resulting in portal hypertension
encephalopathy is infrequent Hepatopulmonary syndrome (28%) liver biochemical tests are usually mildly abnormal
 liver biochemical tests are usually mildly abnormal.")
38
DIAGNOSIS Chronic or subacute Budd-Chiari syndrome should be considered in unexplained liver dysfunction, particularly if ascites is a principal feature, or if risk factors for Budd-Chiari syndrome exist. Clinical: Splenomegaly, venous collaterals Edema of the lower extremities suggests occlusion of the inferior vena cava Signs of right-sided congestive heart failure (such as jugular venous distension)
")
39
Acute : hepatomegaly, RUQ pain, ascites
Accuracy of noninvasive imaging modalities depends upon: duration of disease, location of the clot. Portal vein thrombosis limits therapeutic options and has a poor prognosis

40
Doppler ultrasonography
Screening test hepatomegaly, splenomegaly, ascites, intraabdominal collaterals, caudate lobe hypertrophy, atrophy of other hepatic lobes, compression of IVC Thickening, irregularity, stenosis, or dilation of the walls of the hepatic veins Abnormal flow in the major hepatic veins or IVC

41
CT scan Delayed or absent filling of the three major hepatic veins
Patchy flea-bitten appearance of the liver Rapid clearance of dye from the caudate lobe Narrowing and/or lack of opacification of the inferior vena cava

42
Magnetic resonance imaging
typical distorted "comma-shaped" intrahepatic collaterals unremarkable ultrasound examination but in whom the suspicion is high Venography Gold standard for diagnosis plan therapeutic interventions . Determine pressure gradient above and below the entrance of the hepatic veins into the inferior vena cava

43
Accurately define the extent or characteristics of the hepatic venous flow
Compression of the intrahepatic IVC, leads to sluggish flow in hepatic veins. As a result, the hepatic veins can be undetectable during ultrasound Doppler studies, although they may be patent and amenable to therapy

44
Liver biopsy Can be diagnostic in the acute or subacute form
Features include centrizonal congestion, necrosis, and hemorrhage Cirrhosis may be present in the chronic form Determine prognosis and guide therapy Cirrhotics are less likely to benefit from revascularization procedures

45
thrombotic process in Budd-Chiari syndrome may not involve all the hepatic veins.
Thus, the distribution of the typical pathologic findings may be focal or patchy. As a result, some patients require biopsy of both the right and the left lobes of the liver. laparoscopic approach may be better suited Perfom Bx when there is confusion regarding the diagnosis and plan treatment accordingly

46
TREATMENT Prevent the propagation of the clot
Decompress the congested liver Prevent complications (malnutrition, portal hypertension) _________________________________ Medical treatment (supportive care, anticoagulation, thrombolysis), Radiologic procedures (angioplasty, TIPS,) Surgical intervention (shunting procedures , transplantation).
 _________________________________. Medical treatment (supportive care, anticoagulation, thrombolysis), Radiologic procedures (angioplasty, TIPS,) Surgical intervention (shunting procedures , transplantation).")
47
Medical therapy Diuretics and a low sodium diet
large-volume paracenteses Improve nutritional status Underlying cause should be investigated Myeloproliferative disorder may benefit from treatment with aspirin and hydroxyurea

48
Anticoagulation alone is unlikely to lead to sufficient recanalization of occluded vessels to avoid the progression of liver disease. A trend for a benefit of anticoagulation on survival in less severe disease. Medical therapy : 1) Chronic or subacute Budd-Chiari syndrome with well compensated liver disease at the time of presentation. 2) When other types of therapy are not feasible
 Chronic or subacute Budd-Chiari syndrome with well compensated liver disease at the time of presentation. 2) When other types of therapy are not feasible.")
49
Risk of anticoagulation should also be considered, especially in patients who present with bleeding complications Patients receiving only medical therapy should be monitored closely for disease progression (liver biopsies annually )and portal hypertension complications (looking for varices)
and portal hypertension complications (looking for varices)")
50
Thrombolytic therapy In acute form which blood clots are younger than three to four weeks Do not use thrombolytic agents in: patients who have extensive clot involving the IVC or a clot of unknown age.

51
Radiologic treatment Angioplasty Stenting
Transjugular intrahepatic portosystemic shunt

52
Surgical therapy Restore hepatic venous drainage using shunt surgery
Because of the availability of TIPS, few vascular surgeons routinely perform shunt surgery. Underlying cause of the thrombotic diathesis should be identified and treated prior to considering shunt surgery. Unlikely to be beneficial in patients who have cirrhosis, Such patients are best managed with liver transplantation.

53
survival following shunt surgery depends upon the extent of liver damage prior to surgery, and the continued patency of the shunt Maintenance of shunt patency often requires anticoagulation deterioration in patients following shunt surgery should be investigated by angiography to determine whether the shunt has thrombosed, which may be corrected by angioplasty.

54
Liver transplantation
who are not candidates for radiologic or surgical decompression or who have decompensated cirrhosis protein S, protein C, or antithrombin III deficiency may also be cured of their clotting tendency by liver transplantation, Survival following OLT depends upon the underlying cause of the Budd-Chiari syndrome and the patients condition at the time of the transplant

55
Budd-Chiari syndrome during nephrotic relapse in a patient with resistance to activated protein C clotting inhibitor Am J Kidney Dis.

56
It has long been known that patients with nephrotic syndrome have a hypercoagulable state, which explains the association between nephrotic syndrome, renal vein thrombosis, and thromboembolism. However, the Budd-Chiari syndrome has never been reported in nephrotic patients. This is the first report of such an association that, most likely, depended on a primary resistance to activated protein C

57
Budd-Chiari syndrome and inferior vena cava thrombosis in a nephrotic child.
Pediatr Nephrol.

58
We observed Budd-Chiari syndrome in a boy aged 2 years 6 months with nephrotic syndrome due to hepatic vein and inferior vena cava thrombosis, confirmed by Doppler imaging. Normal values of the routine hemostatic parameters proved that they are of little predictive value for the thrombotic state.

59
Immediate heparin infusion was initiated
Immediate heparin infusion was initiated. High doses of heparin up to 59 IU/kg per hour were required for efficient anticoagulation. A remission of the nephrotic syndrome was achieved with vincristine. Oral anticoagulation with a vitamin K antagonist was continued for 6 months. Doppler imaging then indicated full re-establishment of the blood flow through the affected vessels.

60
The favorable outcome was due to the immediate heparin infusion and prompt remission of the nephrotic syndrome. Doppler imaging was an important tool for non-invasive diagnosis and follow-up.

61
Thromboembolic complications in children with nephrotic syndrome in Bulgaria (1974-1996).
Pediatr Nephrol.

62
Over a period of 22 years, 447 children with nephrotic syndrome (NS) have been retrospectively studied for clinically apparent thromboembolic complications (TEC). The incidence of TEC is 2% (9/447). TEC were predominantly venous (81% venous vs. 19% arterial). The most commonly affected vessels were deep leg veins, IVC, SVC, mesenteric artery, and hepatic veins (Budd-Chiari syndrome).
. TEC were predominantly venous (81% venous vs. 19% arterial). The most commonly affected vessels were deep leg veins, IVC, SVC, mesenteric artery, and hepatic veins (Budd-Chiari syndrome).")
63
Etiology based prevalence of Budd-Chiari syndrome in eastern India
J Assoc Physicians India.

64
Idiopathic membranous obstruction and stricture of IVC are the commonest cause of BCS in the eastern part of India. Hepatocellular carcinoma is also a common cause, presenting in the fulminant form. Ultrasonography may be a helpful screening test for BCS, IVC and hepatic vein catheterisation is essential for a complete work up of these patients.

65
Budd-Chiari syndrome--a case report
Nepal Med Coll J.

66
A 21year old male presented with abdominal pain for 2 months and abdominal distension and swelling of lower limbs for 1 month. US showed coarse echotexture of liver and intraluminal filling defect of IVC Confirmation of diagnosis was done by inferior venacavography. The patient had nephrotic syndrome as the risk factor for thrombosis. The patient underwent portocaval shunt with significant symptomatic relief.

Similar presentations















 and the portal vein ( 75% of vascularization).>")






 that progresses to cirrhosis Replacement of liver tissue.>")









