Download presentation
Presentation is loading. Please wait.

1
Venous Stasis Dermatitis
Kenneth T. Kircher, DO FAOCD Advanced Dermatology, PLLC

5
Stasis Dermatitis (SD)
An inflammatory process (eczematous) Acute, subacute or chronic Occurs on lower legs Setting of venous insufficiency(VI) Poor flow of venous and lymphatic fluid from the legs and feet to the central circulation Many contributing factors May be accompanied by ulceration
 Acute, subacute or chronic. Occurs on lower legs. Setting of venous insufficiency(VI) Poor flow of venous and lymphatic fluid from the legs and feet to the central circulation. Many contributing factors. May be accompanied by ulceration.")
6
Anatomy and Physiology
Three types of vessels Arteries – high pressure, muscular wall Veins – low pressure, check valves, thin wall Lymphatics – low pressure, check valves, very thin wall The problem – humans are bipedal / gravity Veins and lymphatics rely on the pulsatile nature of arteries and the compressive action of muscle contraction to keep fluid moving up hill from check valve to check valve

8
Disruption of Homeostatic Balance
Damage to veins and/or lymphatics DVT, damage to valves/varicosities, trauma, DM Medications Calcium channel blockers Age related / social Immobility, sedentary, sleeping in a chair Total body fluid over load CHF, renal failure, thyroid disease, others

9
Role of Venous Insufficiency (VI)
Rarely purely venous or lymphatic Pooling of the blood in the veins Increases the hydrostatic pressure Fluid component of blood leaks into surrounding tissue causing edema (+/-pitting) There is a decrease in the O2 tension in tissue Many factors precipitate inflammation (fibrin) Cells of the skin are less healthy (in a milleu of increased waste and lower O2)
 There is a decrease in the O2 tension in tissue. Many factors precipitate inflammation (fibrin) Cells of the skin are less healthy (in a milleu of increased waste and lower O2)")
10
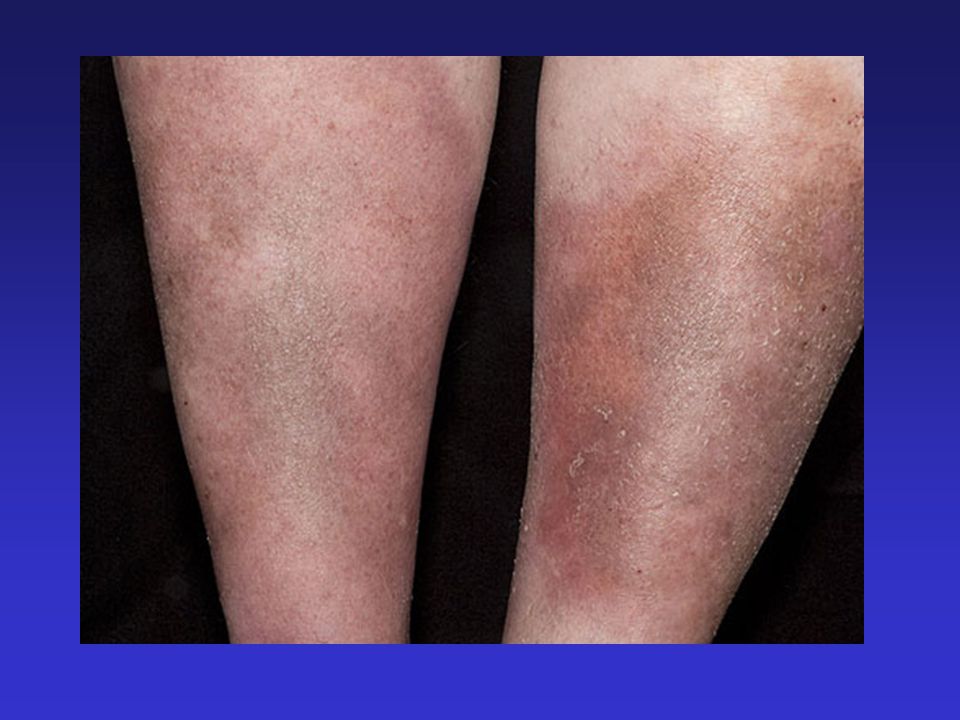
Moderate edema with mild stasis changes

11
Finally… Stasis Dermatitis
VI causes inflammation in the skin and soft tissue Compromised skin more susceptible to drying, irritation and trauma Micro breaks - increased allergy to topical agents ? Allergic response to an epidermal protein Created from increased hydrostatic pressure

12
Allergy to Topical Agents
More likely to have a positive patch test to topical products Common allergens Lanolin, benzocaine, parabens, neomycin, bacitracin (these should be avoided) Possible topical steroid allergy
 Possible topical steroid allergy.")
13
Stages of Eczematous Inflammation
Acute, subacute and chronic Do not have to develop in order Different clinical appearances

14
Acute Inflammation Tends to be more sudden in onset
May mimic cellulitis Boggy, +/-vesicle formation (poison ivy) Often weeps and crusts (yellowish serous exudate) May be accompanied by Id reaction eczematous rash with +/-vesicles on a distant body site
 Often weeps and crusts (yellowish serous exudate) May be accompanied by Id reaction. eczematous rash with +/-vesicles on a distant body site.")
15
Acute on mild chronic changes

16
Acute with chronic changes including depressed scars

17
Subacute Inflammation
More prolonged, insidious in onset Tends to be dryer, red, scaling Scale may be significant (suggesting longer duration) Most commonly seen in winter months with increasing dryness
 Most commonly seen in winter months with increasing dryness.")
18
Subacute

19
Subacute to chronic with excoriations

20
Chronic Inflammation Tends to be thicker, lichenified (accentuation of the skin lines, thickening of the skin, may have thick scale) Skin may have a cobblestoned texture Results from long standing inflammation and often chronic scratching Not the same as chronic stasis changes

21
Severe chronic dermatitis with hyperkeratosis

22
Chronic dermatitis with fibrosis and hyperkeratosis

23
Chronic SD Changes Due to repeated flares and long standing VI
Most common over the medial lower leg/ankle Skin becomes diffusely hyper-pigmented (hemosiderin deposition), may be thickened or atrophied with smooth shiny surface Scarring and fibrosis may present with hypo-pigmentation and avascuarization Atrophie blanche, inverted champagne bottle
, may be thickened or atrophied with smooth shiny surface. Scarring and fibrosis may present with hypo-pigmentation and avascuarization. Atrophie blanche, inverted champagne bottle.")
25
Moderate stasis changes

26
Chronic stasis changes showing lipodermatosclerosis changes (inverted champagne bottle)
")
27
Chronic stasis changes with vascular thrombosis

28
Chronic changes with ulcer

29
Ulcers Primarily occur on medial lower extremity
Thought to be due to venous reflux of perforating veins May lead to increased fibrin deposition and increased fibrosis of skin Tend to be shallow, painful or minimally painful, in a setting chronic VI changes, scarring, atrophie blanche

30
Ulcers - When To Biopsy Not responding to therapy (carefully measure)
Very long standing Unusual appearance Unsure of diagnosis DDx of Ulcers – arterial, neuropathic, infectious, immunologic, neoplastic, hematologic, infestations

31
Typical Clinical Course
Pts have a history of mild swelling of lower legs Begins in 30’s or 40’s or after child birth, a surgical procedure, DVT, trauma, weight gain and others Swelling gradually worsens over time Is exacerbated by high salt intake, prolonged standing it is worse at night and better in the morning

32
Clinical Course Continued
Legs get dry especially in winter Severe flares with burning itch are more common (acute on chronic inflammation) The color of the lower legs slowly changes darkening becoming chronically red brown Tissue becomes fibrosed or bound down feeling, areas of scar may appear Ulcers begin medially, healing slowly
 The color of the lower legs slowly changes darkening becoming chronically red brown. Tissue becomes fibrosed or bound down feeling, areas of scar may appear. Ulcers begin medially, healing slowly.")
33
History How severe Symptoms Prior treatment
Only in evening, gone in morning, all the time, drainage, history of ulcer Symptoms Burn, itch, fatigue, pain Prior treatment What are they applying (creams, topical antibiotics, peroxide etc)
")
34
History Review past medial history Medications
CHF, DM, neuropathy, DVT, trauma (surgery), varicosities, arthritis, poor mobility, protein loss Medications Calcium channel blockers, diuretics- compliance How long have they had swelling If recent, prolonged sitting or immobilization, pain in calf, unilateral or bilateral Social Do they sleep in a flat bed or sitting in a chair
, varicosities, arthritis, poor mobility, protein loss. Medications. Calcium channel blockers, diuretics- compliance. How long have they had swelling. If recent, prolonged sitting or immobilization, pain in calf, unilateral or bilateral. Social. Do they sleep in a flat bed or sitting in a chair.")
35
Physical Exam General exam Pitting edema Varicosities?
Pulmonary exam, cardiac exam as indicated Pitting edema +1 – 4 (subjective but I use 1 ~ slight, 2 ~ ¼ to ½ inch, 3 ~ ½ to ¾ inch, 4 ~> ¾ inch) How high does it go? (mid shin, knee, thigh) Does it appear to be on the verge of vesiculation or ulcer? Varicosities?
 How high does it go (mid shin, knee, thigh) Does it appear to be on the verge of vesiculation or ulcer Varicosities")
36
Physical Exam Continued
Chronic stasis changes Pigment changes, atrophie blanche, ulcer scars Is it hot, cool, tender Evidence of neuropathy (touch toes and sole or nylon bristle) Check pulses (may be hard to feel with severe edema), capillary refill Check both legs
 Check pulses (may be hard to feel with severe edema), capillary refill. Check both legs.")
37
Treatment of SD Treat underlying disease
Venous reflux, CHF Treat the underlying cause – blood is pooling in the TISSUE of the lower leg ***The bulk of fluid is in the tissue but the patient may be intravascularly euvolemic*** Treat the inflammation Reduce the inflammation and repair the skin

38
Treat ‘Tissue’ Fluid Overload
Compression and elevation – most important Compression hose – knee high is usually OK Mild (Class I) mm Hg Moderate (Class II) 30 – 40 mm Hg Severe (Class III) 40 – 50 or even 60 mm Hg Need to be Mod to be covered by ins Hard to get on, uncomfortable, hard to manage especially if arthritis, poor mobility, elderly
 mm Hg. Moderate (Class II) 30 – 40 mm Hg. Severe (Class III) 40 – 50 or even 60 mm Hg. Need to be Mod to be covered by ins. Hard to get on, uncomfortable, hard to manage especially if arthritis, poor mobility, elderly.")
39
After two days of ACE wrap

40
Treating ‘Tissue’ Fluid Overload
Compliance – always an issue Tubey grips Elastic stocking that comes in 3 sizes, Rx to fold over in a double layer, pts have to be measured OTC Hose Light, easier to get on, less uncomfortable , come in colors Wearing less effective hose is more effective than not wearing more effective hose

41
Treating ‘Tissue’ Fluid Overload
Elevation Reversing the venous pooling of blood and aids in lymphatic drainage Feet should be above the buttocks Recliners are great (ask where they sleep) Elevate bottom 1/3 of mattress with news print or suit case or foam wedge (under the mattress) to a height of inches (‘no leg on a pillow’)
 Elevate bottom 1/3 of mattress with news print or suit case or foam wedge (under the mattress) to a height of inches (‘no leg on a pillow’)")
42
Treating ‘Tissue’ Fluid Overload
***Diruetics*** Decrease the intravascular volume, but most of the fluid is extravascular, so… though helpful in fluid overload (CHF) they alone are NOT THE ANSWER Many patients on diuretics have a decreased intravascular volume and persistent edema
 they alone are NOT THE ANSWER. Many patients on diuretics have a decreased intravascular volume and persistent edema.")
43
Unna Boot A zinc oxide impregnated gauze, covered with cotton cling and then a double layer of coban Applied in the office and left on 3 – 7 days. Covers skin with a moist and soothing dressing Zinc is a cofactor in wound healing Supplies compression Takes away compliance as an issue

44
Unna Boot How to apply Best to apply after leg has been wrapped as to minimize edema (seldom done) Zinc gauze is wrapped from the foot to above the calf and just below the knee Next a thin layer of cotton cling (+/-) Finally a layer of coban (short stretch disposable wrap), pull to full stretch and then release to 50% ? Too tight, have the patient back in 2 – 3 hours
 Finally a layer of coban (short stretch disposable wrap), pull to full stretch and then release to 50% Too tight, have the patient back in 2 – 3 hours.")
45
Modified Unna Boot Apply clobetasol ointment, followed by cling and coban Good for short duration (2-4 days) Decreases inflammation I bill as for an Unna boot

46
The Last Thing on Unna Boots
Teach your nurse how to do it well Coding for Unna boot 29508 Medicare allowable: $43.16 (Kingston region)
")
47
Decreasing Inflammation (‘Dermatology Part’)
Topicals Class I or II steroid in an ointment base Clobetasol (class I) (My ‘go to’) Fluocinonide (Lidex) (class II) Ointments are less likely to cause contact allergy Apply BID for 10 – 14 days No other topicals - except Vaseline if needed
 (My ‘go to’) Fluocinonide (Lidex) (class II) Ointments are less likely to cause contact allergy. Apply BID for 10 – 14 days. No other topicals - except Vaseline if needed.")
48
Decreasing Inflammation
Systemic cortisones Infrequently used because topicals work well and side effects Used for Id reaction (widely distributed eczematous reaction) Consider infection Culture it! – especially for an odiferous or non healing ulcer Don’t ‘jump to antibiotics’
 Consider infection. Culture it! – especially for an odiferous or non healing ulcer. Don’t ‘jump to antibiotics’")
49
Maintenance Care Compression and elevation Skin care
Negotiate a means to maintain minimal edema Education, education, education Compliance , compliance, compliance – its always an issue Skin care Moisturize with Vaseline only Limit steroid to 1-2 days per week, BID up to 10 days for flare

50
Ulcer Treatment Consider culture or biopsy if NOT responding
All biopsies carry a risk of worsening the ulcer Wound care Avoid debridement, vaseline, non-stick dressing Compressed with (ACE wrap, coban, hose) Try to avoid adhesives Diagram and measure length and widths Treat surrounding skin
 Try to avoid adhesives. Diagram and measure length and widths. Treat surrounding skin.")
51
Patient after 6 months at wound care

52
After two months of tubey grips 24/7 and vaseline BID

53
Case I 52 YO woman, works as a toll collector, sits on a stool or stands 8 hours a day Swelling in legs worsening over last year, better in morning Legs get red and are now slightly discolored Not using moisturizer, no other topicals Itch at times

54
Moderate edema with mild stasis changes

55
Case I Treatment Hose (education) Elevate (education)
Mild to moderate especially for prolonged standing or sitting (sell it) (OTC for compliance and esthetics) Elevate (education) When able, bottom 1/3 of bed… recurring dividend Moisturize (education) Cream or vaseline especially in winter
 (OTC for compliance and esthetics) Elevate (education) When able, bottom 1/3 of bed… recurring dividend. Moisturize (education) Cream or vaseline especially in winter.")
56
Case II 48 YO obese female with history of leg edema following child birth now with chronic swelling, stands at auto parts counter 8 hrs per day Worsening, has swelling in morning, pain Has not had an ulcer Severe redness and itch at times Uses OTC anti-itch cream, polysporin

58
Case II Treatment Hose (education) Elevation (education)
Mod compression all day maybe tubey grips HS Elevation (education) Over lunch, evening, bed (be realistic) Topical (education) Moisturize daily with Vaseline Clobetasol Ung for flares BID up to days
 Over lunch, evening, bed (be realistic) Topical (education) Moisturize daily with Vaseline. Clobetasol Ung for flares BID up to days.")
59
Case III 72 YO male, DMII and arthritis
Many year history of swelling, worse now, pain, oozing at times, R > L legs Ulcer 3 years ago, healed at wound center Wears old hose sometimes – don’t help Using peroxide to dry up the legs Sleeps in a bed

60
Note cut socks

61
Case III Treatment New hose (education) Elevation (education) Topicals
Moderate (rubber gloves, cuff), OTC, tubey grips Elevation (education) Recliner, bed (dividend), whenever sitting Topicals Bathe regularly, clobetasol ointment BID for 2 weeks then vaseline daily FU – 2 weeks (education, compliance)
, OTC, tubey grips. Elevation (education) Recliner, bed (dividend), whenever sitting. Topicals. Bathe regularly, clobetasol ointment BID for 2 weeks then vaseline daily. FU – 2 weeks (education, compliance)")
62
Case IV 72 YO morbidly obese female with long standing swelling and scaling, recently worse, history of CHF takes Lasix 20 mg BID (+/-), arthritis Leg is oozing fluid, non painful ulcer No hose Lives alone and sleeps sitting in a chair No topicals

65
Case IV Treatment Hose (education) Elevation (education)
Clobetasol ung and Ace wrap today, to leave on over night and Una Boot in the AM Elevation (education) Recliner, bottom 1/3 of bed (be persistant) Topicals to be addressed as per case III Medical ? Change Lasix to 40mg QD, when?, ? Echo etc FU 4 – 7 days, ? Visting or office nurse visit
 Recliner, bottom 1/3 of bed (be persistant) Topicals to be addressed as per case III. Medical. Change Lasix to 40mg QD, when , Echo etc. FU 4 – 7 days, Visting or office nurse visit.")
66
Thank you ! Questions?

Similar presentations


























 Low blood pressure (hypotension) is pressure so low it causes symptoms or signs due to the low flow of blood through the.>")