Download presentation
Presentation is loading. Please wait.

1
The Child with Genitourinary Alterations
N422-Pediatrics Feb 2001 Linda Heath

2
Pediatric Differences
Kidney begins to reach adult functioning about 1 year of age Infants cannot concentrate urine as efficiently as older children and adults

4
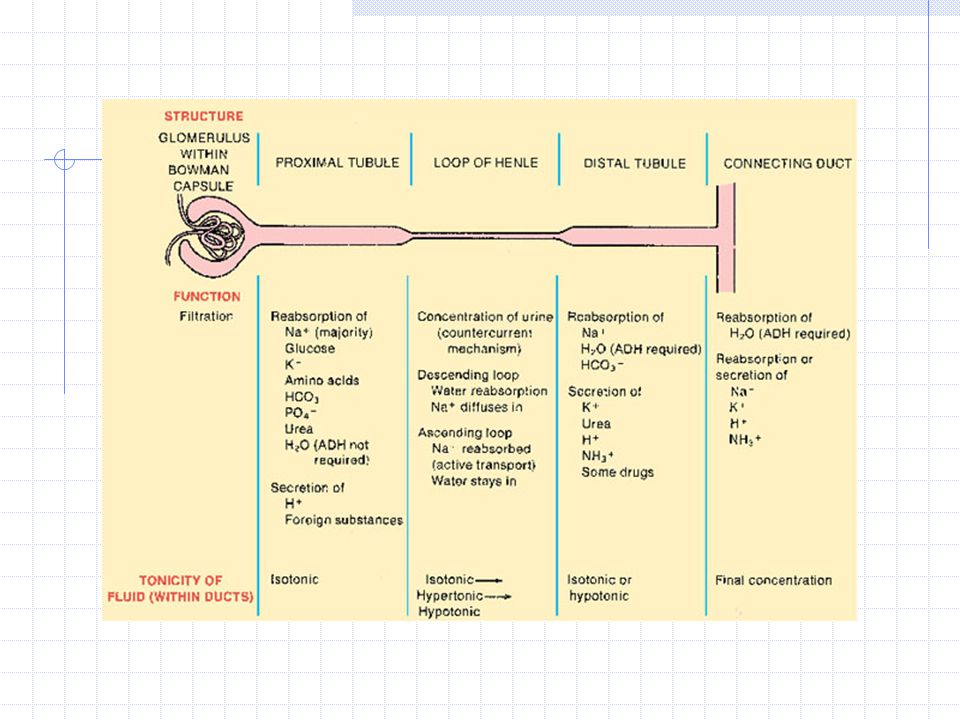
Review Genitourinary System
Maintain fluid & electrolyte balance through glomerular filtration, tubular reabsorption, and secretion Hormonal functions Produces renin in glomerulus—regulates BP Produces Erythropoietin—stimulates RBC production in bone marrow Metabolized Vitamin D—to active form which is important in calcium metabolism

6
Medications commonly used for GU Disorders
Diuril Produces diuresis Tofranil Treatment of nocturnal enuresis Lasix Treat edema Ditropan Antispasmodic.Relieves symptoms of bladder contractions Epoeitn Stimulates RBC production. Cyclosporine Used with corticosteroids to prevent rejection of transplanted organs

7
Common Tests CT scan Cystocopy IVP KUB Renal Arteriogram Renal Biopsy
BUN (Increases in renal insufficiency) Creatinine Serum Osmolality Urinalysis Specific Gravity pH Protein Glucose Ketones WBCs, RBCs Bacteria CT scan Cystocopy IVP KUB Renal Arteriogram Renal Biopsy Renogram Renal Ultrasound VCUG
 Creatinine. Serum Osmolality. Urinalysis. Specific Gravity. pH. Protein. Glucose. Ketones. WBCs, RBCs. Bacteria. CT scan. Cystocopy. IVP. KUB. Renal Arteriogram. Renal Biopsy. Renogram. Renal Ultrasound. VCUG.")
8
Urinary Tract Infections
Cystitis Pyelonephritis Incidence Assessment Evaluation Treatment Prevention

10
Vesicoureteral Reflux (VUR)
Backflow or reflux of urine from the bladder into the ureters and possibly to the kidney Urine returns to bladder after voiding UTI (urinary tract infection) is the most common clinical manifestation VCUG, renal scan Graded I – V Low dose prophylactic antibiotic therapy
 is the most common clinical manifestation. VCUG, renal scan. Graded I – V. Low dose prophylactic antibiotic therapy.")
11
Classification of Reflux

12
Glomerulonephritis Hematuria Proteinuria Edema Injury in glomerulus
Follows bacterial or viral infection (Strept) Hematuria Proteinuria Edema Renal insufficiency S&S of fluid overload
 Hematuria. Proteinuria. Edema. Renal insufficiency. S&S of fluid overload.")
13
Pathophys of Glomerulonephritis

14
Nsg Dx: Glomerulonephritis
Fluid volume excess r/t decreased U.O. Risk for activity intolerance r/t fatigue Risk for impaired skin integrity r/t edema and decreased activity Altered nutrition: less than body requirements r/t fluid and diet restrictions Anxiety r/t hospitalization, knowledge deficit of disease

15
Nephrotic Syndrome Primary Proteinuria Hypoalbuminemia Edema Secondary
Most common Disorder within glomerulus Proteinuria Hypoalbuminemia Edema Secondary Hepatitis SLE Heavy metal poisoning Cancer

16
Pathophys of Nephrotic Syndrome

17
Nephrotic Syndrome Edema
Noted in periorbital spaces and dependent areas of the body Child may awaken with facial edema, as the day progresses, edema becomes less noticeable

18
Nsg Dx: Nephrotic Syndrome
Risk for impaired skin integrity r/t edema and decreased circulation Risk for infections r/t urinary loss of gammaglobulins Risk for fluid volume deficit (intravascular) r/t proteinuria, edema, and effects of diuretics Fluid volume excess r/t decreased excretion of Na and water retention Anxiety (parental) r/t caring for child with chronic disease and hospitalization
 r/t proteinuria, edema, and effects of diuretics. Fluid volume excess r/t decreased excretion of Na and water retention. Anxiety (parental) r/t caring for child with chronic disease and hospitalization.")
19
Comparison Nephrotic Syndrome & Glomerulonephritis
3-4+ Proteinuria Microscopic Hematuria Low Serum Albumin Neg ASO & streptozyme Normotensive Electrolytes normal Glomerulonephritis 0-2+ Proteinuria Hematuria Normal Serum Albumin Positive ASO & strepto Frequently hypertensive Na (low), K (elevated)
, K (elevated)")
20
Enuresis Unable to control bladder function although reached an age at which control of voiding is expected “Nocturnal Enuresis”—Bed wetting Most will eventually outgrow with therapeutic intervention

21
Pathophys and etiology of Enuresis
Control of urination is r/t maturation of CNS By 5 years, most are aware of bladder fullness and can control voiding Daytime first with nighttime dryness later Girls seems to master before boys Children with primary enuresis may have delayed maturations of this part of CNS. They are not able to “sense” bladder fullness and do not awaken to void

22
Nsg Dx: Enuresis Situational low self-esteem r/t bedwetting or urinary incontinence Impaired social interaction r/t bedwetting or urinary incontinence Ineffective family coping: compromised r/t negative social stigma and increased laundry load

23
Cryptorchidism Undescended or “hidden” testicle
One or both testes fail to descend through inguinal canal into the scrotal sac Inguinal hernias are commonly associated with this Most infants with cryptorchidism will have spontaneous descent of their testes during the first year of life; Surgical intervention after that

24
Pathophys of Cryptorchidism
Fetal development: testes descend from the abdomen during 7th – 9th month gestation Failure to descend unknown ?abnormality of testis itself ?insufficient hormonal stimulation for the normal descent process Sperm production is decreased in undescended testis and increased risk of developing a malignancy when child receives adulthood

25
Nsg Dx: Crytorchidism Knowledge deficit (parental) r/t cause and management of cryptorchidism Anxiety r/t possible decreased fertility and increased risk of testicular malignancy

26
Hypospadius Congenital anomaly
Actual opening of the urethral meatus is “below” the normal placement on the glans of the penis Goal of surgery: to make urinary & sexual function as normal as possible and improve appearance of penis

27
Pathophys of Hypospadias
Incomplete development of urethra in utero Exact cause unknown (? R/T genetic, environmental and hormonal influences) Displacement of urethral meatus does not usually interfere with urinary continence Stenosis of opening can occur causing problems with partial obstruction of outflowing urine. This might result in hydronephrosis or UTIs Ventral placement of urethral opening might interfere with fertility in the mature male, if left uncorrected
 Displacement of urethral meatus does not usually interfere with urinary continence. Stenosis of opening can occur causing problems with partial obstruction of outflowing urine. This might result in hydronephrosis or UTIs. Ventral placement of urethral opening might interfere with fertility in the mature male, if left uncorrected.")
28
Nsg Dx: Hypospadius Knowledge deficit (parental) r/t diagnosis, surgical correction, & post-op care Risk of infection r/t indwelling catheter Impaired physical mobility r/t surgical procedure of penis

29
Bladder Extrophy Congenital anomaly
Extrusion of bladder to the outside of the body through defect in lower abdominal wall May be associated with genital anomalies or defects of anus

30
Pathophys of Bladder Exstrophy
Result of inappropriate growth during embryonic development Degree of deformity depends on when the disruption occurs during fetal development. The earlier in development the more severe the deformity Most infants with bladder exstrophy have normal kidneys but may be at risk for kidney damage due to VUR and bladder dysfunction, which may occur after surgical reconstruction

31
Nsg Dx: Bladder Exstrophy
Impaired tissue integrity r/t exposed bladder mucosa Knowledge deficit (parental) r/t diagnosis and anomaly Risk for Infection r/t anatomical defect, surgical procedures, and probable abnormal bladder function Body image disturbance r/t physical appearance of lower abdomen and genitalia
 r/t diagnosis and anomaly. Risk for Infection r/t anatomical defect, surgical procedures, and probable abnormal bladder function. Body image disturbance r/t physical appearance of lower abdomen and genitalia.")
32
Acute Renal Failure Sudden severe loss of kidney function
Kidneys can no longer filter waste products, regulate fluid volume, nor maintain chemical balance Uncommon in the pediatric patient Most children with ARF regain renal function

33
Pathophys of ARF Prerenal ARF Intrarenal ARF Postrenal ARF
Decreased perfusion of kidney Decreased blood flow and ischemia cause cell swelling, cell injury, and poss cell death Causes: dehydration, perinatal asphyxia, hypotension, septic shock, hemorrhagic shock, and renal artery obstruction Intrarenal ARF Actual damage to kidney tissue Causes: aminoglycosides, contrast dye, obstruction, HUS, glomerulonephritis, pyelonephritis Postrenal ARF Obstruction of urine outflow causing decreased renal function due to pressure within kidney Causes: obstruction problems within kidney, neurogenic bladder, stones, tumor, edema

34
Dialysis

35
Chronic Renal Failure ESRD & Kidney transplant

36
Nsg Dx: ARF Fluid volume excess r/t kidney dysfunction
Risk for infection r/t invasive procedures and fluid overload Altered family process r/t child hospitalized with serious disorder Altered nutrition: less than body requirements r/t anorexia and decreased intake due to restrictions Knowledge deficit r/t disease process, therapy, and prognosis

37
Hemolytic Uremic Syndrome (HUS)
Anemia Thrombocytopenia Acute renal failure E.coli 0157:H7

38
Pathophys of HUS Prodrome of GI symptoms E. coli 0157:H7
Bacteria grow and multiply in intestines Bacteria produce toxin that damages the endothelial cells of capillary walls leading to inflammation. Significant in renal glomeruli Occlusion of glomeruli decreases filtration and results in ARF Vascular process of HUS can affect any organ Anemia results damaged RBC as they pass through occluded vessels and are removed from circulation by spleen Thrombocytopenia occurs because the platelets get trapped within the small vessels

Similar presentations










 RENAL DISEASE: OVERVIEW AND ACUTE RENAL FAILURE Pathophysiology of Disease: Chapter 16 (388-394) Jack.>")










