Download presentation
Presentation is loading. Please wait.

1
Tharwat S Kandil Prof Of GI Surgery www.tharwat-kandil.com
Stomach Anatomy Tharwat S Kandil Prof Of GI Surgery

2
Anatomy The stomach is J-shaped, baglike organ that expands to store food Appears in week 5. A pliable, saccular organ. Located in the LUQ and epigastrium. Separated from the GI tract (2 locations).
.")
3
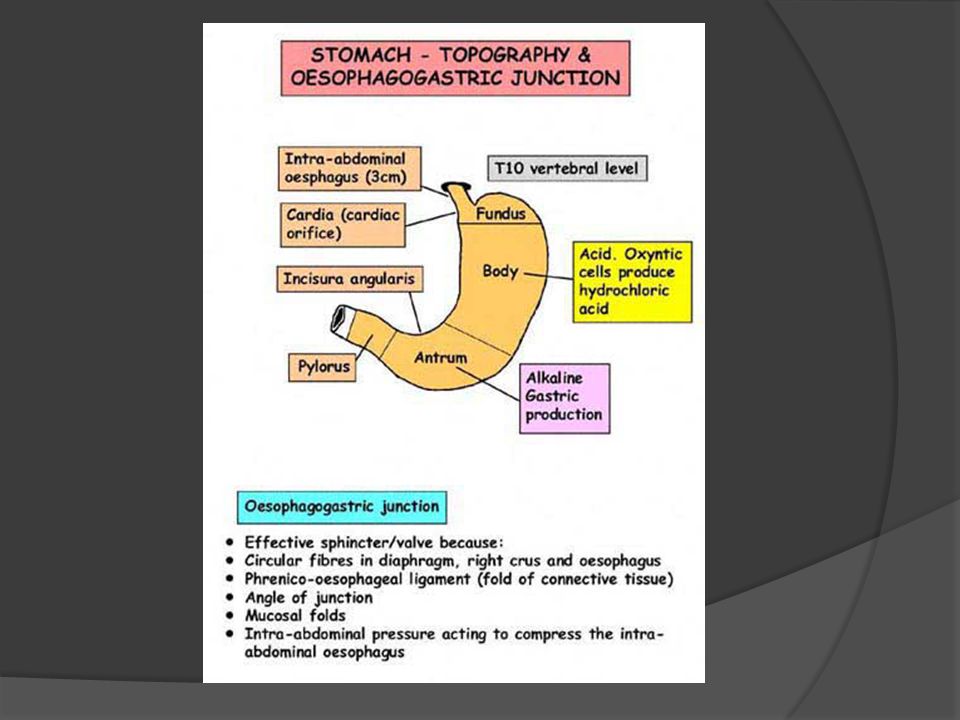
Gross Anatomy Proximal= Cardia (attaches to esophagus) attaches at the LES. Fundus= most superior portion, receives food. Body= largest portion, contains parietal, chief and ECL cells. Distal= antrum, contains the G cells.

4
Histologically The stomach is almost entirely covered with peritoneum.
The peritoneum forms the outer gastric serosa. Beneath the serosa is the muscularis propria (MP). The MP is made up of 3 layers of smooth muscle. inner oblique layer: This layer is responsible for creating the motion that churns and physically breaks down the food. It is the only layer of the three which is not seen in other parts of the digestive system. The antrum has thicker skin cells in its walls and performs more forceful contractions than the fundus.
. The MP is made up of 3 layers of smooth muscle. inner oblique layer: This layer is responsible for creating the motion that churns and physically breaks down the food. It is the only layer of the three which is not seen in other parts of the digestive system. The antrum has thicker skin cells in its walls and performs more forceful contractions than the fundus.")
5
The middle layer is the circular muscle and is the only “complete” layer of muscle
As you progress distally the middle layer of muscle begins to thicken and form the Pylorus Which functions as a true sphincter. This and the GE junction form the gastric “borders” and are the two “fixed” points of the stomach. The outer muscle layer (longitudinal) is contiguous with the outer layer of the esophagus.
 is contiguous with the outer layer of the esophagus.")
6
Within the layers of the MP, there is a rich plexus of autonomic nerves and ganglia .
The submucosa lies between the MP and the mucosa. It is a collagen rich layer of connective tissue and is the weakest/strongest layer of the gastric wall. The submucosa also contains the rich blood vessel network and the lypmhatics as well as Meissner’s plexus.

7
The mucosa consists of 3 layers:
Surface epithelium (columnar). Lamina propria Connective tissue layer that supports the surface epithelium. Muscularis mucosae (probably the reason for rugal folds). The MM is the boundary for invasive/noninvasive gastric cancer.
. Lamina propria. Connective tissue layer that supports the surface epithelium. Muscularis mucosae (probably the reason for rugal folds). The MM is the boundary for invasive/noninvasive gastric cancer.")
8
The stomach presents two openings, two borders or curvatures, and two surfaces.
Openings.—The opening by which the esophagus communicates with the stomach is known as the cardiac orifice, and is situated on the left of the middle line at the level of the tenth thoracic vertebra. The short abdominal portion of the esophagus (antrum cardiacum) is conical in shape and curved sharply to the left, the base of the cone being continuous with the cardiac orifice of the stomach. The right margin of the esophagus is continuous with the lesser curvature of the stomach, while the left margin joins the greater curvature at an acute angle, termed the incisura cardiaca.
 is conical in shape and curved sharply to the left, the base of the cone being continuous with the cardiac orifice of the stomach. The right margin of the esophagus is continuous with the lesser curvature of the stomach, while the left margin joins the greater curvature at an acute angle, termed the incisura cardiaca.")
9
The pyloric orifice communicates with the duodenum, and its position is usually indicated on the surface of the stomach by a circular groove, the duodenopyloric constriction. This orifice lies to the right of the middle line at the level of the upper border of the first lumbar vertebra.

10
Curvatures.—The lesser curvature (curvatura ventriculi minor), extending between the cardiac and pyloric orifices, forms the right or posterior border of the stomach. It descends as a continuation of the right margin of the esophagus in front of the fibers of the right crus of the diaphragm, and then, turning to the right, it crosses the first lumbar vertebra and ends at the pylorus. Nearer its pyloric than its cardiac end is a well-marked notch, the incisura angularis, which varies somewhat in position with the state of distension of the viscus; it serves to separate the stomach into a right and a left portion. The lesser curvature gives attachment to the two layers of the hepatogastric ligament, and between these two layers are the left gastric artery and the right gastric branch of the hepatic artery.

11
The greater curvature (curvatura ventriculi major) is directed mainly forward, and is four or five times as long as the lesser curvature. Starting from the cardiac orifice at the incisura cardiaca, it forms an arch backward, upward, and to the left; the highest point of the convexity is on a level with the sixth left costal cartilage. From this level it may be followed downward and forward, with a slight convexity to the left as low as the cartilage of the ninth rib; it then turns to the right, to the end of the pylorus.

12
Directly opposite the incisura angularis of the lesser curvature the greater curvature presents a. dilatation, which is the left extremity of the pyloric part; this dilatation is limited on the right by a slight groove, the sulcus intermedius, which is about 2.5 cm, from the duodenopyloric constriction. The portion between the sulcus intermedius and the duodenopyloric constriction is termed the pyloric antrum.

13
At its commencement the greater curvature is covered by peritoneum continuous with that covering the front of the organ. The left part of the curvature gives attachment to the gastrolienal ligament, while to its anterior portion are attached the two layers of the greater omentum, separated from each other by the gastroepiploic vessels.

14
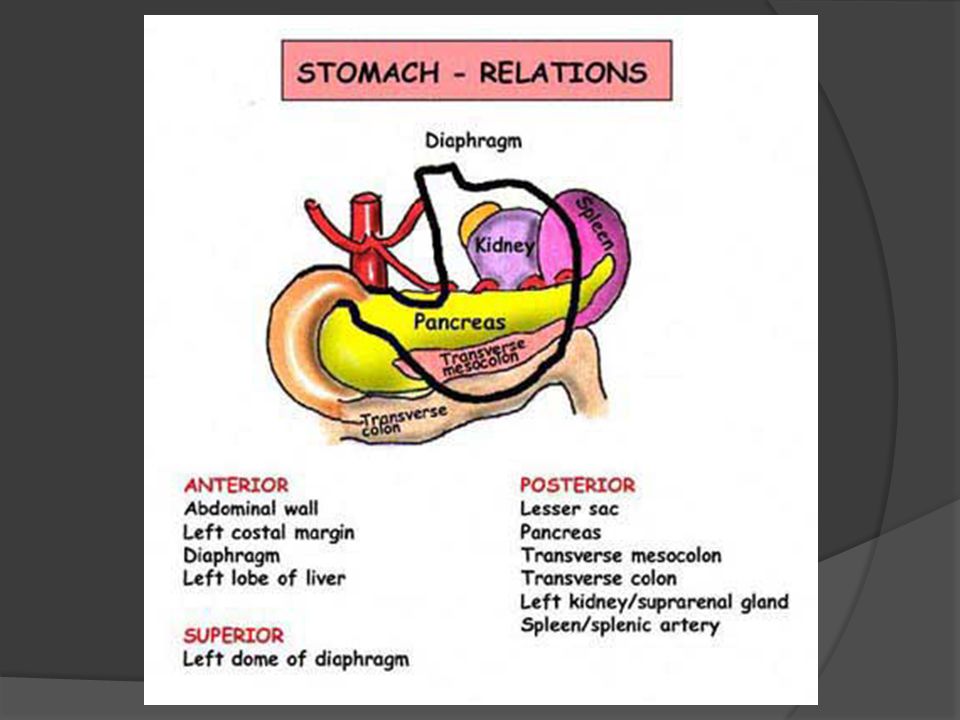
Surfaces.—When the stomach is in the contracted condition, its surfaces are directed upward and downward respectively, but when the viscus is distended they are directed forward, and backward. They may therefore be described as anterosuperior and postero-inferior. Antero-superior Surface.—The left half of this surface is in contact with the diaphragm, which separates it from the base of the left lung, the pericardium, and the seventh, eighth, and ninth ribs, and intercostal spaces of the left side. The right half is in relation with the left and quadrate lobes of the liver and with the anterior abdominal wall. When the stomach is empty, the transverse colon may lie on the front part of this surface. The whole surface is covered by peritoneum.

15
The Postero-inferior Surface is in relation with the diaphragm, the spleen, the left suprarenal gland, the upper part of the front of the left kidney, the anterior surface of the pancreas, the left colic flexure, and the upper layer of the transverse mesocolon. These structures form a shallow bed, the stomach bed, on which the viscus rests. The transverse mesocolon separates the stomach from the duodenojejunal flexure and small intestine. The postero-inferior surface is covered by peritoneum, except over a small area close to the cardiac orifice; this area is limited by the lines of attachment of the gastrophrenic ligament, and lies in apposition with the diaphragm, and frequently with the upper portion of the left suprarenal gland

17
Cell Types, 1 Parietal: Mucus: Chief: Location: Body
Function: secrete acid and intrinsic factor Mucus: Location: Body, Antrum Function: mucus production Chief: Function: produce Pepsin

18
Cell Types, 2 Surface epithelium: ECL: G cells: Location: Diffuse
Function: produce mucus, bicarb, prostaglandins(?) ECL: Location: Body Function: Histamine production G cells: Location: Antrum Function: Gastrin production
 ECL: Location: Body. Function: Histamine production. G cells: Location: Antrum. Function: Gastrin production.")
19
Cell Types,3 D cells: Gastric mucosal interneurons: Entric Neurons:
Location: Body, Antrum Function: produce Somatostatin Gastric mucosal interneurons: Function: produce Gastrin-releasing peptide Entric Neurons: Location: Diffuse Function: CGRP, others production

20
The stomach serves a variety of functions:
Storage. Because of its accordion like folds (called rugae), the wall of the stomach can expand to store two to four liters of material. Temporary storage is important because you eat considerably faster than you can digest food and absorb its nutrients. Mixing. The stomach mixes the food with water and gastric juice to produce a creamy medium called chyme.
, the wall of the stomach can expand to store two to four liters of material. Temporary storage is important because you eat considerably faster than you can digest food and absorb its nutrients. Mixing. The stomach mixes the food with water and gastric juice to produce a creamy medium called chyme.")
21
Physical breakdown. Three layers of smooth muscles (rather than the usual two) in the muscularis externa churn the contents of the stomach, physically breaking food down into smaller particles. In addition, HCl denatures (or unfolds) proteins and loosens the cementing substances between cells (of the food). The HCl also kills most bacteria that may accompany the food.
 in the muscularis externa churn the contents of the stomach, physically breaking food down into smaller particles. In addition, HCl denatures (or unfolds) proteins and loosens the cementing substances between cells (of the food). The HCl also kills most bacteria that may accompany the food..")
22
Chemical breakdown. Proteins are chemically broken down by the enzyme pepsin. Chief cells, as well as other stomach cells, are protected from self-digestion because chief cells produce and secrete an inactive form of pepsin, pepsinogen. Pepsinogen is converted to pepsin by the HCl produced by the parietal cells. Only after pepsinogen is secreted into the stomach cavity can protein digestion begin. Once protein digestion begins, the stomach is protected by the layer of mucus secreted by the mucous cells.

23
Controlled release. Movement of chyme into the small intestine is regulated by a valve at the end of the stomach, the pyloric sphincter.

25
Arterial Supply The stomach is supplied by many arteries : 1- short gastric arteries - branches of the splenic artery - supply the fundus of stomach 2-left gastro epiploic artery - branch of the splenic artery - supply the greater curvature of the stomach . 3- left gastric artery which is a direct branch of the coeliac trunk that arises from the aorta . supplies the lesser curvarture. 4- right gastric artery which is a branch of the common hepatic artery - supplies the lesser curvature. 5- right gastro epiploic artery which is a branch of the gastro duodenal artery which is again a branch of the common hepatic artery- supplies the greater curvature

26
Arterial Supply

27
Venous Drainage

28
Lymphatic Drainage

29
Nerve Supply The vagus nerve is composed of both motor and sensory fibers, and has a more extensive course and distribution than any of the other cranial nerves, since it passes through the neck and thorax to the abdomen.

30
Nerve Supply Branches of Distribution.—The branches of distribution of the vagus are: In the Jugular Fossa… Meningeal. Auricular. In the Neck………… Pharyngeal. Superior laryngeal. Recurrent. Superior cardiac. In the Thorax………. Inferior cardiac. Anterior bronchial. Posterior bronchial. Esophageal. In the Abdomen……. Gastric. Celiac. Hepatic.

31
Nerve Supply The Gastric Branches (rami gastrici) are distributed to the stomach. The right vagus forms the posterior gastric plexus on the postero-inferior surface of the stomach and the left the anterior gastric plexus on the antero-superior surface. The Celiac Branches (rami cæliaci) are mainly derived from the right vagus: they join the celiac plexus and through it supply branches to the pancreas, spleen, kidneys, suprarenal bodies, and intestine. The Hepatic Branches (rami hepatici) arise from the left vagus: they join the hepatic plexus and through it are conveyed to the liver.
 are distributed to the stomach. The right vagus forms the posterior gastric plexus on the postero-inferior surface of the stomach and the left the anterior gastric plexus on the antero-superior surface. The Celiac Branches (rami cæliaci) are mainly derived from the right vagus: they join the celiac plexus and through it supply branches to the pancreas, spleen, kidneys, suprarenal bodies, and intestine. The Hepatic Branches (rami hepatici) arise from the left vagus: they join the hepatic plexus and through it are conveyed to the liver.")
32
Nerve Supply

33
Thanks for your attention

Similar presentations
>")


















