Download presentation
Presentation is loading. Please wait.

1
Down Syndrome & Psychiatric Disorders Update Robert J. Pary, M.D. November 14, 2014 NADD

2
Disclosures None

3
By the end of the presentation, the participant will be able to List the usual developmental milestones in persons with Down syndrome Discuss the most common medical illnesses in persons with Down syndrome that impact behavior Discuss the most common psychiatric illnesses in persons with Down syndrome

4
Down syndrome One out of 800-1,000 live births Most common genetic cause of ID Etiology – trisomy 21 – 94% have extra chromosome – 5% translocation – 1% mosaicism Both normal and trisomic cells

5
Neuroanatomic differences and DS Lott, 2012 Fetal brain size is smaller Volumes of frontal and temporal lobe are reduced Neuronal contact, synaptic density and synaptic length are all abnormal

6
Neuroanatomic differences and DS Lott, 2012 Functional consequences of brain changes – Abnormal neuronal connectivity – Limiting processing of information

7
Age distribution of persons with DS in England & Wales in 2011 N=37090 Wu & Morris 2013 0-19 years11625 20-49 years19494 50-59 years4475 60-69 years 70+ years 1403 93

8
Age distribution of persons with DS in England & Wales in 2011 N=37090 Wu & Morris 2013 Baby with DS born in 1950 had a 1-yr survival < 50% Birth in 1970s, 1-year survival > 90% Average life expectancy for babies with DS born in 2011 was 51 years Median life expectancy was 58 years

9
I’m glad to have Down syndrome. I think it’s a good thing to have for all people that are born with it. I don’t think it’s a handicap. It’s a disability for what you’re learning because you’re learning slowly. It’s not that bad. There’s a lot of things I did a lot of other people don’t do. Kingsley, J., & Levitz, M Count Us In 1994

10
Like being in two different shows, going to a lot of conventions, award ceremonies like the Kennedy’s, and I’m a famous actor. First of all, when I was three, that’s when I started to be in the show ‘This is My Son’... When I was three through sixteen I was filming ‘Sesame Street’. Kingsley, J., & Levitz, M Count Us In 1994

11
Social Development and DS Compared to cognition and language, social development is a relative strength Factors contributing to enhanced social development – Innate characteristics of child with DS – Perceptions of parents and teachers – Decreased societal stigma Guaralnick et al., 2011

12
Social Development and DS Vulnerabilities to social competence – Social understanding – Emotional regulation when frustrated or facing challenging problems – Appropriate caution when meeting strangers – Limited verbal expression Guaralnick et al., 2011

13
Social Development and DS Child with DS’s desire for social interaction can overcome limited verbal expression Unstructured play in preschool may provide difficulties given that such play is often more complex Guaralnick et al., 2011

14
DS and Language More communicative gestures are preserved despite a generalized verbal impairment Vicari et al., 2013 Receptive language is typically stronger than expressive language, and vocabulary is stronger than syntax

15
DS and Language Children and adolescents with DS – Produce shorter and less complex utterances than would be expected based on nonverbal mental age – Syntax complexity may continue to improve into late adolescence and young adulthood Martin et al., 2009

16
DS and Language Communication strengths – Ability to stay on topic – Narrative skills – Ability to respond to requests for clarification in order to repair communicative breakdowns – Relatively strong whole-word recognition skills Martin et al., 2009

17
Down Syndrome & Speech Impairment Challenges – Difficulty initiating conversation – Challenges elaborating on topics – Trouble initiating repairs of communicative breakdowns – Voice – Sound production – Fluency and prosody – Intelligibility Kent & Vorperian, 2013

18
Down Syndrome & Speech Impairment Challenges in verbal communication can affect assessment of psychiatric disorders Language decline in later adulthood may be part of dementia

19
Down Syndrome & Speech Impairment Speech cannot be isolated from other aspects of communication or cognition Problems with speech must be viewed in a larger context of perceptual, motor and linguistic abilities. » Kent & Vorperian, 2013

20
Speech problems in DS Anatomic differences in the vocal tract hearing acuity 2 nd recurrent otitis media Impaired speech perception Poor short-term memory Impaired vowel articulation Impaired motor function – Dysarthria – Apraxia » Kent & Vorperian, 2013

21
Verbal praxis skills & DS Reflects a difficulty in generating actions from memory Suggests some aspects of speech production disorders would be based on deficiencies in central processes » Kent & Vorperian, 2013

22
Speech & Language Interventions Language input should be based on a child’s receptive rather than expressive ability Persons with DS have > visual memory – Use of visually-oriented pictures and storybooks, may enhance learning Martin et al, 2009

23
Speech & Language Interventions Early intervention is more effective than later intervention for young children with DS – Even when intervention is delayed by only two months Martin et al, 2009

24
Speech & Language Interventions Prelinguistic skills training & parent education may be effective interventions for young children with DS who produce few words – teach young children to use coordinated eye gaze, vocalizations, and gestures through prompts – teach parents to be responsive to their children’s verbal and nonverbal behaviors Martin et al, 2009

25
Speech & Language Interventions For individuals with Down syndrome who are severely unintelligible, initial treatment targets may include more functional vocabulary, such as words for basic needs and names of family members Martin et al, 2009

26
Conversational recasting Develops more complex syntax Child’s utterance is reshaped by the communication partner (clinician, teacher, or family member) to include additional grammatical information Child says “doggy sleep,” the communication partner could elaborate “the doggy is sleeping” Martin et al, 2009
 to include additional grammatical information Child says doggy sleep, the communication partner could elaborate the doggy is sleeping Martin et al, 2009")
27
Speech & Language Interventions Augmentative communication (AAC) systems, such as sign language, visual schedules, pictures, object symbols, or computerized speech production – Delayed speech onset – Impaired speech intelligibility Martin et al, 2009
 systems, such as sign language, visual schedules, pictures, object symbols, or computerized speech production – Delayed speech onset – Impaired speech intelligibility Martin et al, 2009")
28
Psychopathology & Children and Adolescents with DS Are children/adolescents with DS at greater/lesser risk for psychiatric illness? It depends

29
Psychopathology & Children and Adolescents with DS Vicari et al., 2013 C/A with DS 18-23% Compared to general population – more – C/A in general population 8-18% Compared to those with ID - less – C/A with ID 30-40%

30
Challenging Behavior – Injures self – Injures others – Destroys property – Interferes with acquiring or performing developmentally appropriate skills (home, classroom, or work) – Prevents others from wanting to interact resulting in social isolation
 – Prevents others from wanting to interact resulting in social isolation")
31
Challenging Behavior in Children with DS Feeley & Jones 2008 Common – Stubborn and obstinate – Attention problems – Social withdrawal – Noncompliance – Compulsions – Escape motivated behavior

32
Challenging Behavior Applied behavior analysis can effectively decrease challenging behaviors in children with DS

33
Challenging Behavior in Children with DS Feeley & Jones 2008 Setting events – occurrences that can influence behaviors – Poor sleep – Illnesses

34
Challenging Behavior in Children with DS Feeley & Jones 2008 N is 5 yr with DS Some days N appears – Tired – Pushes away educational material (challenging behavior) Communication book (teachers and parents) or assess tiredness at school Assessed sleep
 Communication book (teachers and parents) or assess tiredness at school Assessed sleep")
35
Challenging Behavior in Children with DS Feeley & Jones 2008 On days with reported less sleep by parents – Teachers would alter plan that day – Instead of workbook page of counting – Game of counting bowling pins (N preferred)
")
36
Challenging Behavior in Children with DS Feeley & Jones 2008 C is 4 yr with DS who often refuses requests and drops to floor Functional assessment – occurred during transitions from an activity Reinforcing items – stickers, computer games, crayons, bubbles

37
Challenging Behavior in Children with DS – Antecedent Strategies Feeley & Jones 2008 Use before challenging behavior occurs Prespecified reinforcer – “your favorite game is ready on computer” Distractor as preferred item – Carry crayon supplies to next room; whistle blower Choice High probability request sequence, then low – “Touch nose (praise); touch ear (praise); give me five (praise); lets go to next room Collaboration
; touch ear (praise); give me five (praise); lets go to next room Collaboration")
38
Challenging Behavior in Children with DS Feeley & Jones 2008 Child with DS may not have necessary skill Child wants a break, but is unable to verbally ask for it Instead throws items to show that he is finished with activity

39
Challenging Behavior in Children with DS Feeley & Jones 2008 Child who is unable to say he is ready for a break – Can be taught replacement behavior » Sign for break » Tap teacher’s shoulder

40
Challenging Behavior in Children with DS Feeley & Jones 2008 M is 6 year old who hugs strangers M taught to shake hands with familiar adults instead M taught difference between familiar and unfamiliar adults M taught socially acceptable with peers (high five, thumbs up, fancy handshake)
")
41
Challenging Behavior Repetitive behavior that is rewarding physiologically is not necessarily OCD – Stealing – Hyperventilation – Masturbation – Overeating – Polydipsia – Smoking – Humming – Pacing Vicari et al. 2013

42
Health problems in adults with DS Alzheimer disease Celiac disease Congenital heart disease Depression Diabetes mellitus Eczema Eye or Hearing impairment Hypothyroidism Osteoarthritis Seizures Sleep apnea Henderson et al. 2006

43
Health conditions and DS Sleep Apnea Esbensen, 2010 Children - 30-55% Midfacial and lower jaw hypoplasia Position of tonsils and adenoids Hypotonia of upper airway Adults Obesity Increasing age

44
Health conditions and DS Sensory Impairments Esbensen, 2010 Vision – Up to 70% of adults have impairment – Nearly half go undiagnosed Hearing – Loss 30-40 yr earlier than general population – In one study up to 80% of care providers and GPs unaware of hearing loss

45
Health conditions and DS Musculoskeletal Esbensen, 2010 Degenerative osteoarthritis of spine – About 20% middle-age and 40% elderly – Difficult to detect - underreported – Numbness, weakness and pain Osteoporosis related to – Early menopause, physical inactivity, low muscle tone, decreased strength

46
Health conditions and DS Thyroid Dysfunction Esbensen, 2010 Risk increases with aging Up to 40% adults with abnormal thyroid function tests About 8% with active hypothyroidism

47
Point Prevalence affective disorder or OCD in adults with DS N= 186 Mantry et al 2008 OCD – Clinical 1 (0.5%) – DC-LD 1 (0.5%) – DCR- ICD-10 0 – DSM-IV-TR 0
 – DC-LD 1 (0.5%) – DCR- ICD-10 0 – DSM-IV-TR 0")
48
Point Prevalence affective disorder or OCD in adults with DS N= 186 Mantry et al 2008 Affective disorder – Clinical 5 (2.7%) – DC-LD 3 (1.6%) – DCR– ICD-10 2 (1.1%) – DSM-IV-TR 1 (0.5%)
 – DC-LD 3 (1.6%) – DCR– ICD-10 2 (1.1%) – DSM-IV-TR 1 (0.5%)")
49
Obsessive-Compulsive Behavior OCD in persons with DS (0.8-4.5%) is not higher than the general population In children, if OC symptoms occur abruptly, consider post-strep infection or PANDAS Vicari et al. 2013 Treatment is similar to general population

50
Obsessional slowness Individual who takes hours to bathe, to get dressed, or to eat Occurs in both men and women

51
Treatment for obsessional slowness SSRIs (fluoxetine, citalopram, sertraline, etc.) SNRIs (venlafaxine, etc.) PLUS pacing (giving rewards for taking gradually less time) – Taking 55 minutes to wash instead of 1 hour; then taking 50 minutes, etc.
 SNRIs (venlafaxine, etc.) PLUS pacing (giving rewards for taking gradually less time) – Taking 55 minutes to wash instead of 1 hour; then taking 50 minutes, etc.")
52
Mood disorders and DS Vicari et al., 2013 In adolescents and young adults, psychosocial stressors often recede onset of mood disorder Self care may deteriorate requiring assistance or prompting Somatic symptoms key to diagnosis

53
Depressed mood may be described by others as a change from what is usually observed Sad facial expression Absence of facial expression Rarely smiles or laughs Cries or appears tearful

54
Irritable mood Acts grouchy or has angry facial expression Angry affect + onset/increase in behaviors Assaultive Spitting Self-injuring Yelling or swearing Disruptive or destructive

55
Suicidal ideation in persons with ID Charlot et al. DM-ID 2007 Recurrent thoughts of death – Often talking about death or people who died – Morbid preoccupations – Unfounded physical complaints accompanied by fears of death

56
Treatment of depression Walker et al. 2011 Sobering findings in major peer- reviewed literature – No randomized-controlled studies of antidepressants – No case reports in English in 21 st C – No studies of psychotherapy in persons with DS – No case reports on ECT in > 20 years

57
Treatment of depression Walker et al. 2011 What is known Compared to known practice guidelines, persons with DS, are treated suboptimally – Patients were not treated to remission –still were having persistent depressive symptoms – When one drug failed, alternative not tried – Unknown whether work with cognitive-behavior therapy in persons with mild ID will also work with persons with DS

58
APA Practice guideline (general population) 2010 Treatment of acute phase aims for remission of depressive symptoms Mild to moderate MDD – Antidepressant alone – Psychotherapy alone – Both antidepressant and psychotherapy
 2010 Treatment of acute phase aims for remission of depressive symptoms Mild to moderate MDD – Antidepressant alone – Psychotherapy alone – Both antidepressant and psychotherapy")
59
APA Practice guideline (general population) 2010 Antidepressants for most patients Selective serotonin reuptake inhibitor (SSRI) Serotonin norepinephrine reuptake inhibitor (SNRI) Mirtazapine Bupoprion
 2010 Antidepressants for most patients Selective serotonin reuptake inhibitor (SSRI) Serotonin norepinephrine reuptake inhibitor (SNRI) Mirtazapine Bupoprion")
60
APA Practice guideline (general population) 2010 ECT is treatment of choice in persons with SEVERE depression who have not responded to psychotherapy or to pharmacotherapy – Especially if psychotic or catatonic – Not eating/drinking nutritional effects
 2010 ECT is treatment of choice in persons with SEVERE depression who have not responded to psychotherapy or to pharmacotherapy – Especially if psychotic or catatonic – Not eating/drinking nutritional effects")
61
Psychosis and DS Vicari et al., 2013 Some evidence that psychosis is rare in persons with DS (as is bipolar dx) Is there some resiliency factor in DS? No published studies to the authors knowledge on psychotic-like experiences and at risk mental states in DS

62
Alzheimer disease and DS Head et al., 2012 Not everyone with DS develops AD Typical AD brain changes occur by 40 yr – Senile plaques – Neurofibrillary tangles Clinical signs of dementia more commonly observed > 50 yr

63
Clinical signs of AD and DS Head et al., 2012 Memory can be affected early Changes in personality and behavior may signal early manifestations of AD Adults who had good social skills show socially deficient communication Diagnosis of dementia can be difficult

64
Seizures and DS Lott, 2012 Onset of seizures > 45 yr more likely to herald dementia As many as 80 + % of adults with DS and AD Probably associated with rapid cognitive decline

65
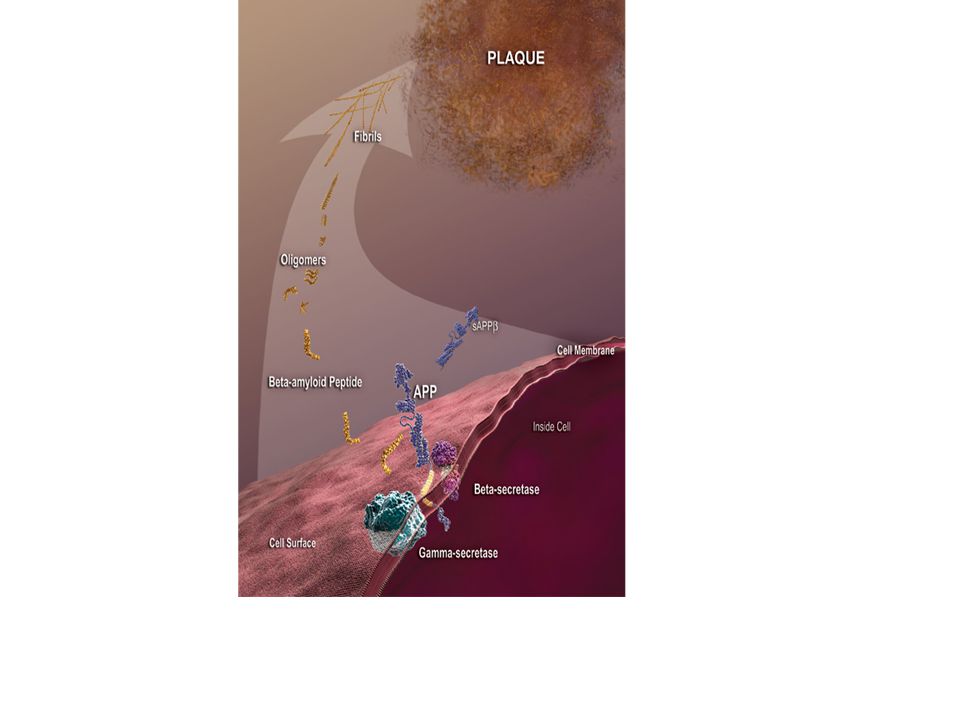
AD, Aβ and DS Head et al., 2012 Amyloid precursor protein (APP) is on Chromosome 21 APP is cleaved by beta- and gamma- secretases to release beta-amyloid peptide (Aβ)
 is on Chromosome 21 APP is cleaved by beta- and gamma- secretases to release beta-amyloid peptide (Aβ)")
66
Amyloid precursor protein Genetics home reference

68
AD, senile plaques and DS Head et al., 2012 Senile plaques contain Aβ Aβ – toxic to neurons Aβ – hypothesized as cause of dementia

69
FDA-approved treatments for AD – N-Methyl-D-aspartate (NMDA) receptor antagonist Memantine – Cholinesterase Inhibitors Donepezil Galantamine Rivastigmine Tacrine (rarely used because of liver damage)
 receptor antagonist Memantine – Cholinesterase Inhibitors Donepezil Galantamine Rivastigmine Tacrine (rarely used because of liver damage)")
70
Alzheimer disease and DS Head et al., 2012 FDA-approved treatments for AD have had moderate to little success in persons with DS

71
DYRK1A dual-specificity tyrosine-(Y)- phosphorylation regulated kinase 1A Genetics Home Reference
- phosphorylation regulated kinase 1A Genetics Home Reference")
72
AD, DYRK1A and DS Lott, 2012 Contributes to early-onset neurofibrillary degeneration Enhances phosphorylation of amyloid precursor protein DYRK1A mediated hyper- phosphorylation of tau may provide functional link between AD and DS

73
Tau Neuronal microtubule-associated proteins Maintains the cytoskeleton and axonal transport Aggregation of tau in filamentous inclusions – Common feature of neurofibrillary tangles in Alzheimer disease Genetics Home Reference

74
Future direction – Amyloid-Associated depression? Amyloid-β precursor protein (APP) is on chromosome 21 APP can be cleaved to 40 (Aβ-40) or 42 (Aβ-42) amino acid peptides Possible prodrome to developing Alzheimer disease in elderly adults Sun X et al. 2008
 is on chromosome 21 APP can be cleaved to 40 (Aβ-40) or 42 (Aβ-42) amino acid peptides Possible prodrome to developing Alzheimer disease in elderly adults Sun X et al")
75
Depression and Alzheimer Disease in DS Tsiouris et al., 2014 Depressive disorders are the most common psychiatric disorders in adults over 45 years Symptoms of depression and Alzheimer disease overlap Frequency of depression in DS & AD double those with DS but no AD

76
Depression and Alzheimer Disease in DS Tsiouris et al., 2014 Not clear what role depressive disorders have in precipitating or enhancing Alzheimer disease Tsiouris et al. argue that antidepressant meds, especially SSRIs – Increase neurogenesis – Enhance cognitive & physical recovery following a stroke

77
Depression and Alzheimer Disease in DS Tsiouris et al., 2014 Retrospective review 357 adults DS Age at 1 st visit 17 y – 66 y (mean 46y) 17 had mosaicism 160 diagnosed with dementia by end of study 80/157 with dementia also treated with antidepressant
 17 had mosaicism 160 diagnosed with dementia by end of study 80/157 with dementia also treated with antidepressant")
78
Depression and Alzheimer Disease in DS Tsiouris et al., 2014 Mean age of dementia onset was about 15 months later in those that had received antidepressants Mean survival did not significantly differ in those that took versus those that didn’t take antidepressants

79
Depression and Alzheimer Disease in DS Tsiouris et al., 2014 Of the patients with dementia, those on antidepressants were significantly more likely to also be prescribed cholinesterase inhibitors

80
Future Trends Agonists at alpha 7 nicotinic acetycholinergic receptor Rationale – Amyloid binds to this receptor – May improve memory and cognition Deutsch et al., 2014

81
Future Trends Stereriosomer of inositol – scyllo-inositol can block the development of amyloid-beta (Aβ) plaques in the brains of transgenic mice wikipedia – Under investigation in clinical trial
 plaques in the brains of transgenic mice wikipedia – Under investigation in clinical trial")
82
Future Trends Nicotine treatment of cognitive decline in persons with DS Non-smoking adults with DS 7 mg or 14 mg (after 7 d) nicotine patch Total 28 days ClinicalTrials.gov Identifier:NCT01778946
 nicotine patch Total 28 days ClinicalTrials.gov Identifier:NCT")
83
Future Trends A Study of RG1662 in Individuals With Down Syndrome ClinicalTrials.gov Identifier:NCT01436955 Hoffman-LaRoche Study completed N=35

84
References Charlot L et al. Mood Disorders in (Ed) R Fletcher et al. Diagnostic Manual- Intellectual Disability NADD Press Kingston, NY 2007 Deutsch SL et al. 2014 Pro Neuro-Psychoph & Biol Psy 54:131-9 Esbensen AJ 2010 Int Rev Res MR 39:107-126 Head E et al. 2012 Curr Geront Geriatric Res Article ID 412536 Feeley KM & Jones EA 2008 DS Res Pract 12:153-163 Guaralnick MJ et al., 2011 AJIDD 116:48-64 Henderson A et al. 2007 Br J GP 57:50-54. Kent RD & Vorperian HK 2013 J Sp Lang Hear Res 56:178-210 Lott IT 2012 Prog Brain Res 197:101-121 Mantry D et al. 2008 JIDR 52:141-155 Sun X et al. 2008 Arch GP 65(5):542-560. Tsiouris JA et al. 2014 J Clin Psychiatry 75:731-7 Vicari S et al. 2013 Psychiatric Genetics 23:95-107 Walker JC et al. 2011 Res Dev Dis 32:1432-40
: Tsiouris JA et al J Clin Psychiatry 75:731-7 Vicari S et al Psychiatric Genetics 23: Walker JC et al Res Dev Dis 32:")
Similar presentations





![Introduction to Biopsychology [PSB 4002] Professor Robert Lickliter DM 260 / 305-348-3441 website: dpblab.fiu.edu.](/15/4574384/big_thumb.jpg "Introduction to Biopsychology [PSB 4002] Professor Robert Lickliter DM 260 / 305-348-3441 website: dpblab.fiu.edu.>")













