Download presentation
Presentation is loading. Please wait.

1
ACT+FAP TREATMENT OF BORDERLINE PERSONALITY DISORDER Michel André Reyes Ortega PhD * ** *** Angélica Nathalia Vargas Salinas MA * ** *** Edgar Miranda Terres MA ** *** Iván Arango de Montis MD ** María de Lourdes García Anaya MD, PhD ** * Association for Contextual Behavioral Science Mexico Chapter ** Instituto Nacional de Psiquiatría Juan Ramón de la Fuente Muñiz *** Instituto de Ciencias Conductual Contextuales y Terapias Integrativas

2
PSYCHOTHERAPY IMPACTS ON BPD Retrospective studies (15 years) McGlashan (1986) Plakun et al. (1985) Stone (1990) Paris et al. (1987) Paris & Zweig-Frank (2001). Scenario = Mental Health Hospitals Found M=52.2% Age M= 42.8 N= 142 m, 359 w Diagnose system = DSM III Still BPD = 16.5% % suicide = 7.75% Estudios prospectivos (7, 2, 2 y 10 años) Links et al. (1998). Skodol et al. (2005). Grilo et al. (2004). Zanarini, Frankenburg et al. (2005) Scenario = General Health Hospitals Age M= 31 at baseline N= 63 m, 237 w Diagnose = DSM III y DSM IV Still BPD = 33.3% % suicide = 5.85% Improvement associated factors Skills acquisition. Absence of stable couple. Economic independence. Non improvement associated factors. Early sexual abuse and other forms of mistreatment. Substance abuse.
 Stone (1990) Paris et al. (1987) Paris & Zweig-Frank (2001). Scenario = Mental Health Hospitals Found M=52.2% Age M= 42.8 N= 142 m, 359 w Diagnose system = DSM III Still BPD = 16.5% % suicide = 7.75% Estudios prospectivos (7, 2, 2 y 10 años) Links et al. (1998). Skodol et al. (2005). Grilo et al. (2004). Zanarini, Frankenburg et al. (2005) Scenario = General Health Hospitals Age M= 31 at baseline N= 63 m, 237 w Diagnose = DSM III y DSM IV Still BPD = 33.3% % suicide = 5.85% Improvement associated factors Skills acquisition. Absence of stable couple. Economic independence. Non improvement associated factors. Early sexual abuse and other forms of mistreatment. Substance abuse..")
3
BEHAVIORAL THERAPIES FOR BPD Dialectical behavior Therapy (DBT) (P-B). Reductions on self-harm behavior, medical emergencies frequencies, anger and impulsivity; improovements on social adjustment and treatment adherence (Lieb, & Stoffers, 2012; Linehan et. al. 1999; Lieb, Zanarini, Schahl, Linehan & Bohus, 2004; Turner, 2000; Verheul et. al. 2003). Acceptance and Commitment Therapy (ACT) (B). Reductions on self-harm behavior, emotion dysregulation, experiential avoidance, BPD symptoms severity, anxiety and depression (Gratz & Gunderson, 2006; Morton, Snowdon, Gopold & Guymer, 2012). DBT + ACT (B). Better outcomes than ACT or DBT alone (Shearin & Linehan, 1994). Functional Analytic Psychotherapy (FAP) (P-B). Improvement on identity stability and interpersonal dimensions (Callaghan, Summers & Weidman, 2003; Koerner, Kohlenberg & Parker, 1996; Kohlenberg & Tsai, 1991; Kohlenberg & Tsai, 2000). Improvement of ACT impacts (Kohlenberg & Callaghan, 2010; Luciano, 1999) and DBT (Busch, Manos, Rusch, Bowe & Kanter, 2010).
. Acceptance and Commitment Therapy (ACT) (B). Reductions on self-harm behavior, emotion dysregulation, experiential avoidance, BPD symptoms severity, anxiety and depression (Gratz & Gunderson, 2006; Morton, Snowdon, Gopold & Guymer, 2012). DBT + ACT (B). Better outcomes than ACT or DBT alone (Shearin & Linehan, 1994). Functional Analytic Psychotherapy (FAP) (P-B). Improvement on identity stability and interpersonal dimensions (Callaghan, Summers & Weidman, 2003; Koerner, Kohlenberg & Parker, 1996; Kohlenberg & Tsai, 1991; Kohlenberg & Tsai, 2000). Improvement of ACT impacts (Kohlenberg & Callaghan, 2010; Luciano, 1999) and DBT (Busch, Manos, Rusch, Bowe & Kanter, 2010)..")
4
WISE CHOICES: ACT GROUP TREATMENT FOR BPD (Morton & Shaw, 2012) Group sessions - 1st module. Introduction Avoidance and values Willingness and acceptance Awareness of thoughts Mindfulness of pleasure Awareness of emotions, sensations and urges Responding to emotions, sensations and urges Acting on values Obstaces and choice points 18 sessions (25 patients, 1 therapist, 1 cotherapist, 2 monitors)
.")
5
WISE CHOICES: ACT GROUP TREATMENT FOR BPD (Morton & Shaw, 2012) Group sessions – 2nd module. Values in interpersonal relationships Listening mindfully Practising courage to share ourselves Brainstorming alternative perspectives Assertively making requests In the other person’s shoes Giving and receiving positives Negotiation 18 sessions (25 patients, 1 therapist, 1 cotherapist, 2 monitors)
.")
6
WISE CHOICES: ACT GROUP TREATMENT FOR BPD (Morton & Shaw, 2012) “ENHANGEMENT” Individual sessions 1st session: Assesment. Functional analysis: Identifiation of experiential avoidance patterns. Sessions 2-9: Wise Choices enhangement. Review of group week group session. Free use of ACT strategies to solve motivation problems. Assistance in use of current week skills to main problems. Use of FEAR-DARE acronyms Assigning weekly homework. Use of SMART acronym. 16 sessions (4 therapists)
.")
7
WISE CHOICES: ACT GROUP TREATMENT FOR BPD (Morton & Shaw, 2012) “ENHANGEMENT” Individual sessions 10th session: Assesment. Functional analysis: Identifiation of CRBs. Sessions 11-18: Wise Choices FAP enhangement. Review of group week group session. Free use of ACT strategies to solve motivation problems. Assistance in use of current week skills to main problems. Use of FEAR-DARE acronyms. Use of 5 rules to work on CRBs and draw parallels to Os. Assigning weekly homework. Use of SMART acronym. 16 sessions (4 therapists)
.")
8
PILOT STUDY JUSTIFICATION Contribute to psychological well being of BPD diagnosed patients: Diminishing entry to emergencies services, symptoms of emotion dysregulation, impulsivity, suicidal risk, fear of emotions and experiential avoidance; Improving quality of life and interpersonal adjustment. Need to start a research line based about the development and effectiveness of low cost interventions for BPD (Lieb et al., 2004; Marquis & Wilber, 2008). INPRF BPD had one year at pilot study start, TFP (1 year / 2 sessions per week) and DBTinformed where TAU (9 months / 1 group and individual session per week).
. INPRF BPD had one year at pilot study start, TFP (1 year / 2 sessions per week) and DBTinformed where TAU (9 months / 1 group and individual session per week)..")
9
HYPOTHESIS ACT+ will show better lobal outcomes tan TAU on Reduction on BPD symptoms severity – Borderline Evaluation of Severity Over Time Scale (Pfohl et. al. 2009; Reyes & García, 2014). Reduction on Suicide Risk – Plutchik Suicide Risk Scale (Plutchik & Van Pragg, 1989). Reduction on Impulsivity – Plutchik Impulsivity Scale (Plutchik & Van Pragg, 1989; Páez et al. 1996). Reduction on Emotion Dysregulation – Difficulties in Emotion Regulation Scale (Gratz & Roemer, 2004; Marín Tejeda et al. 2012). Reduction on Experiential Avoidance – Acceptance and Action Questionnaire-II (Ciarrochi & Bilich, 2006; Patrón 2010). Reduction on Fear of Emotions – Affective Control Scale (Williams, Chambless & Ahrens, 1997; Ramírez, Ascencio, Reyes & Vargas, 2014). Improvement of Quality of Life – WHO Quality of Life Scale (World Health Organization, 1993). *Results not shown in this presentation
. Reduction on Suicide Risk – Plutchik Suicide Risk Scale (Plutchik & Van Pragg, 1989). Reduction on Impulsivity – Plutchik Impulsivity Scale (Plutchik & Van Pragg, 1989; Páez et al. 1996). Reduction on Emotion Dysregulation – Difficulties in Emotion Regulation Scale (Gratz & Roemer, 2004; Marín Tejeda et al. 2012). Reduction on Experiential Avoidance – Acceptance and Action Questionnaire-II (Ciarrochi & Bilich, 2006; Patrón 2010). Reduction on Fear of Emotions – Affective Control Scale (Williams, Chambless & Ahrens, 1997; Ramírez, Ascencio, Reyes & Vargas, 2014). Improvement of Quality of Life – WHO Quality of Life Scale (World Health Organization, 1993). *Results not shown in this presentation.")
10
STUDY PARTICIPANTS SOCIODEMOGRAPHIC CHARACTERISTISCS

11
STUDY PARTICIPANTS COMORBIDITIES

12
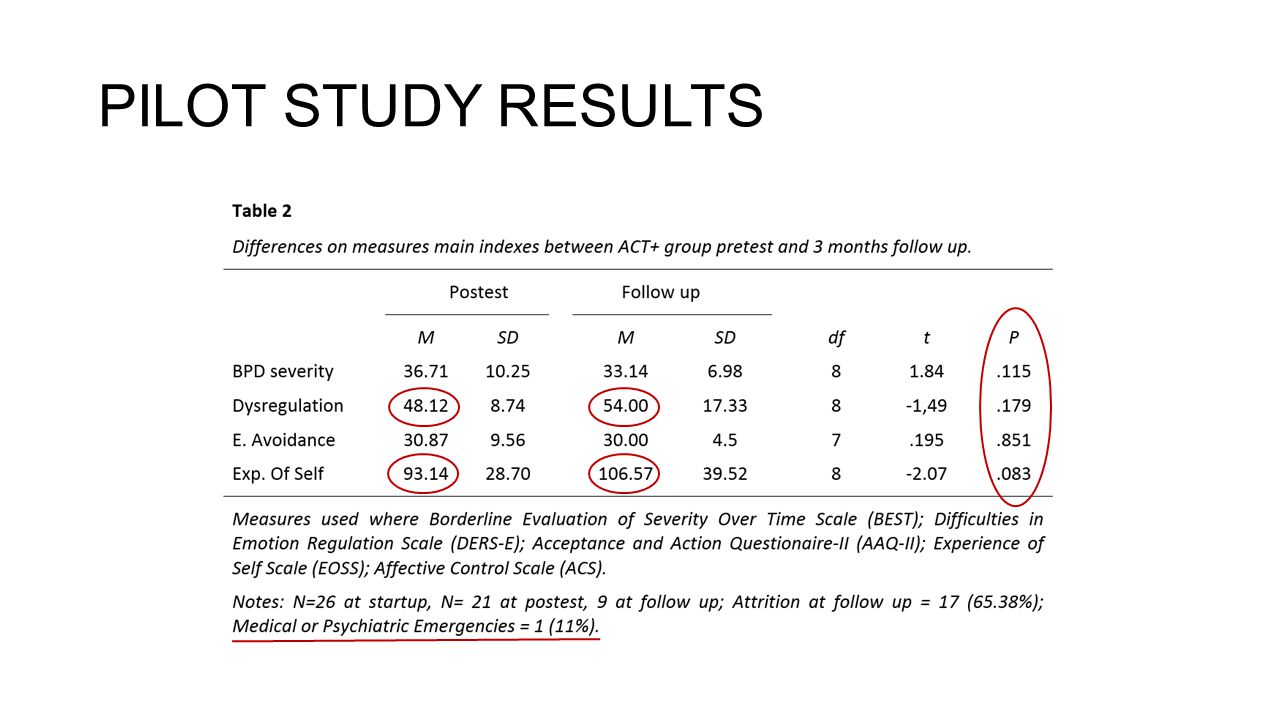
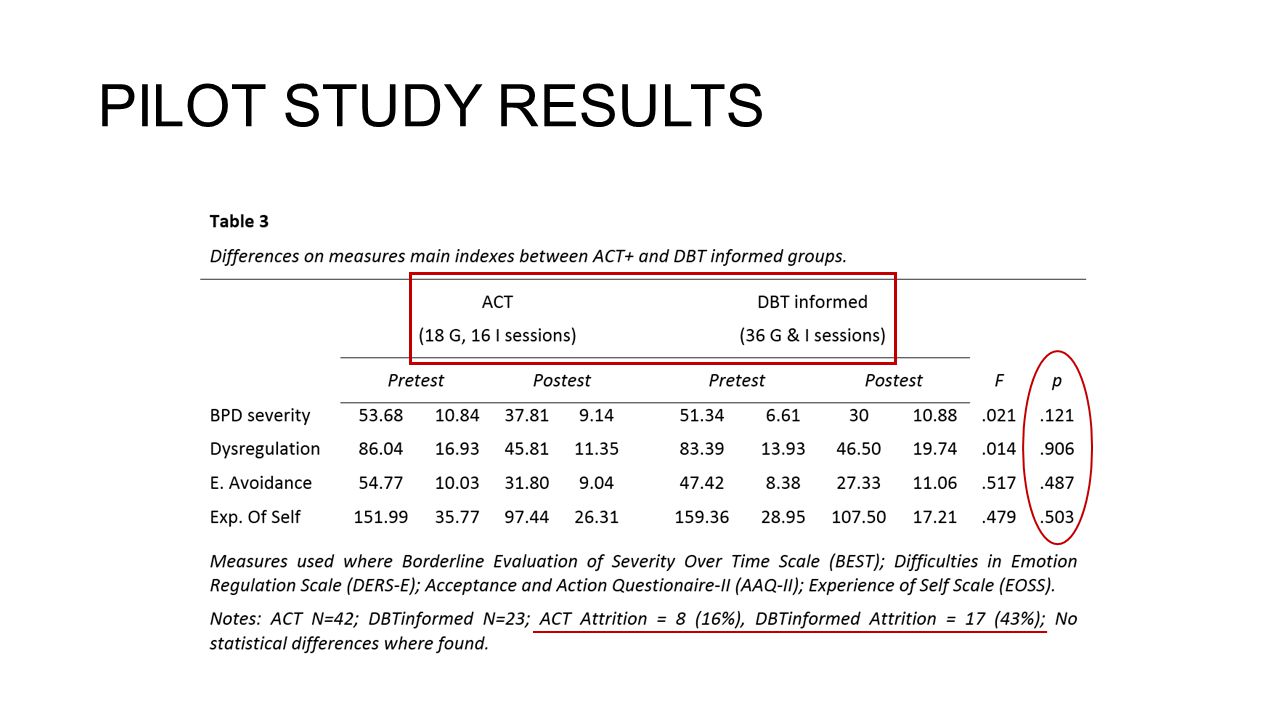
PILOT STUDY RESULTS

16
DISCUSSION AND CONCLUSION HIPOTHESIS TESTING AND IMPACT ACT+ showed to be and effective brief intervention as needed by the INPRF-BPD clinic. ACT+ enhanged could achieve better outcomes, specially on interpersonal satisfaction and social adjustment domains. Include DBT crisis survival and emotion regulation skills on the fist module. Use of Matrix model to integrate ACT and FAP elements. Drawing paralels between CRBs and Os since treatment start including group sessions. Formal FAP on second module individual sessions. ACT+ is the new TAU of the INPRF-BPD clinic. SOLUTIONS TO STUDY LIMITATIONS Need of a wider N Compare groups by age and diagnosis. Need of a RCT to prove effectiveness compared to time equivalent treatments. Asses treatment integrity of all treatments. Refinement of selection criteria. Need of mediational analysis. Asses relation between hypothesized mediational variables and treatment outcomes.

17
CASE CONCEPTUALIZATION (Reyes, 2014; adapted from Polk, 2014) FIVE SENSES EXPERIENCE MENTAL EXPERIENCE ÁPROACHINGAVOIDANCE PERSPECTIVE ------------------ CHOICE POINT I-CRB1s G-CRB1s O1s I-CRB3s G-CRB3s Problematic rules CRB2s G-CRB2s O2s Values I-T1s G-T1s I-T2s G-T2s T3s I-T Values G-T Values
 FIVE SENSES EXPERIENCE MENTAL EXPERIENCE ÁPROACHINGAVOIDANCE PERSPECTIVE CHOICE POINT I-CRB1s G-CRB1s O1s I-CRB3s G-CRB3s Problematic rules CRB2s G-CRB2s O2s Values I-T1s G-T1s I-T2s G-T2s T3s I-T Values G-T Values")
18
CURRENT RESEARCH Participants: 150 participants with BPD diagnosis confirmed by SCID-II; 50 randomly assigned to each group. Schizofrenia, current psychosis, bipolar disorder, neurological conditions and antisocial personality diagnosed participats will be excluded. Age range: 18 – 45 years. RG101 ACT+FAP+DBT (18 G+I sessions) 02 (6 months) 03 (12 months) RG204 ACT+ (18 G+I sessions) 05 (6 months) 06 (12 months) RG3O7 DBTi (18 G+I sessions) 08 (6 months) 09 (12 months)
 02 (6 months) 03 (12 months) RG204 ACT+ (18 G+I sessions) 05 (6 months) 06 (12 months) RG3O7 DBTi (18 G+I sessions) 08 (6 months) 09 (12 months).")
19
RCT HYPOTHESIS H1: ACT+DBT+FAP will show better outcomes than TAU in Reduction on BPD symptoms severity – Borderline Evaluation of Severity Over Time Scale (Pfohl et. al. 2009; Reyes & García, 2014). Reduction on Suicide Risk – Plutchik Suicide Risk Scale (Plutchik & Van Pragg, 1989). Reduction on Impulsivity – Plutchik Impulsivity Scale (Plutchik & Van Pragg, 1989; Páez et al. 1996). Reduction on Emotion Dysregulation – Difficulties in Emotion Regulation Scale (Gratz & Roemer, 2004; Marín Tejeda et al. 2012). Reduction on Experiential Avoidance – Acceptance and Action Questionnaire-II (Ciarrochi & Bilich, 2006; Patrón 2010). Reduction on Fear of Emotions – Affective Control Scale (Williams, Chambless & Ahrens, 1997; Ramírez, Ascencio, Reyes & Vargas, 2014). Improvement of Quality of Life – WHO Quality of Life Scale (World Health Organization, 1993). H2: Hypothesized change mechanisms will significantly mediate impact of treatments. Psychological Flexibility – Acceptance and Action Questionnaire-II (Ciarrochi & Bilich, 2006; Patrón 2010). Mindfulness – Five facets of mindfulness questionnaire (FFMQ; Baer, Smith, Hopkins, Krietemeyer, & Toney, 2006) Emotion Regulation – Difficulties in Emotion Regulation Scale (Gratz & Roemer, 2004; Marín Tejeda et al. 2012). H3: Significant differences on mediational mechanism contribution to change between treatments will be found.
. Reduction on Suicide Risk – Plutchik Suicide Risk Scale (Plutchik & Van Pragg, 1989). Reduction on Impulsivity – Plutchik Impulsivity Scale (Plutchik & Van Pragg, 1989; Páez et al. 1996). Reduction on Emotion Dysregulation – Difficulties in Emotion Regulation Scale (Gratz & Roemer, 2004; Marín Tejeda et al. 2012). Reduction on Experiential Avoidance – Acceptance and Action Questionnaire-II (Ciarrochi & Bilich, 2006; Patrón 2010). Reduction on Fear of Emotions – Affective Control Scale (Williams, Chambless & Ahrens, 1997; Ramírez, Ascencio, Reyes & Vargas, 2014). Improvement of Quality of Life – WHO Quality of Life Scale (World Health Organization, 1993). H2: Hypothesized change mechanisms will significantly mediate impact of treatments. Psychological Flexibility – Acceptance and Action Questionnaire-II (Ciarrochi & Bilich, 2006; Patrón 2010). Mindfulness – Five facets of mindfulness questionnaire (FFMQ; Baer, Smith, Hopkins, Krietemeyer, & Toney, 2006) Emotion Regulation – Difficulties in Emotion Regulation Scale (Gratz & Roemer, 2004; Marín Tejeda et al. 2012). H3: Significant differences on mediational mechanism contribution to change between treatments will be found..")
Similar presentations








 & Group Therapy Services (GTS)>")











