Download presentation
Presentation is loading. Please wait.

1
Basics of hemostasis Christiane Thienelt, MD Assistant Professor of Medicine Hematology/Oncology DVAMC/UC Denver 2014

2
Objectives 1. Overview of coagulation 2. Basic coagulation tests
3. Bleeding disorders

3
What is Hemostasis? Hemostasis=injury to blood vessel triggers a series of reactions Formation of fibrin-platelets plugs Bleeding stops 1. vascular phase 2. platelet phase (primary hemostasis) 3. coagulation phase (secondary hemostasis) 4. Regulation of extension of clot by coagulation factor inhibitors and by Fibrinolysis 5. remodeling and repair after arrest of bleeding
 3. coagulation phase (secondary hemostasis) 4. Regulation of extension of clot by coagulation factor inhibitors and by Fibrinolysis. 5. remodeling and repair after arrest of bleeding.")
4
Hemostasis Stabilization by fibrin formation Extension of clot
(clotting cascade)=secondary hemostasis Extension of clot limited by: Natural anticoagulants Platelet plug forms =primary hemostasis Fibrinolysis
=secondary hemostasis. Extension of clot. limited by: Natural anticoagulants. Platelet plug forms. =primary hemostasis. Fibrinolysis.")
5
What is Thrombosis? Uncontrolled pathological clotting
Propagation of a clot to occlude normal blood flow Ironically, the generation of a NORMAL hemostatic plug and the formation of an ABNORMAL thrombus are basically the same mechanisms!

6
Importance of Coagulation in Medicine
Good hemostasis=Good Surgery Clot Busting ( Thrombolysis)= Cardiovascular Medicine, life-threatening PE ( pulmonary embolism)
= Cardiovascular Medicine, life-threatening PE ( pulmonary embolism)")
7
Components of hemostasis
1. Endothelium-vessel wall 2. Platelets 3. Coagulation factors

8
Vessel Wall Normal Endothelium: -inhibits coagulation
-prevents platelet aggregation -promotes clot breakdown -provides barrier to reactive elements in the vessel wall

9
Prevent blood from leaking out holes
Vessel Wall Prevent blood from leaking out holes in blood vessels

10
Vascular phase-Vessel Wall injury
Injury of blood vessel leads to VASOCONSTRICTION diverting blood flow Collagen, Tissue factor and von Willebrand factor (vWF) are exposed Platelet adhere, aggregate and activate blood coagulation
 are exposed. Platelet adhere, aggregate and activate blood coagulation.")
11
Platelet Phase: Physiology
Megakaryocyte in bone marrow: precursor for platelets derived from hematopoietic stem cells Up to 2000 platelets Bud off, circulate 7-10 days Spleen: 1/3 of platelets TPO: thrombopoietin main growth and maturation factor for megakaryocytes

12
Platelet adhesion: Blood Flow
Normal Endothelium: -inhibits coagulation -prevents platelet aggregation -promotes clot breakdown -provides barrier to reactive elements in the vessel wall platelets are moving through the blood vessel at the outer edge of the laminar blood flow Flow highest in the center, slowest in the periphery -denuded endothelium (injury)leads to pseudopods to increase area of surface contact From: Mechanisms in Hematology
leads to pseudopods to increase area of surface contact. From: Mechanisms in Hematology.")
13
Formation of a Platelet Plug
There are 4 events in the formation of a platelet plug: Platelet adhesion Platelet activation Platelet aggregation Fibrin formation and support of local coagulation

14
Smooth discoid shape of resting platelets
Spiny spheric shape of activated platelets

15
vWF=von Willebrand Factor is von Willebrand disease
Lack /dysfunction of vWF=von Willebrand Factor is von Willebrand disease Glycoproteins on platelet surface are receptors for adhesive proteins present in the vessel wall and in plasma. Numbering is based on separation pattern on gel electrophoresis Platelet adhesion receptors and their ligands include: list Single ligand may bind to different receptors and initiate several functional responses Binding of vWF to GPIb by way of cytoplasmic signal activates GP IIb/IIIa promoting binding of fibrinogen and vWF From: Mechanisms in Hematology

16
Platelet Adhesion: Main mechanisms
=Platelets adhere to the injured surface and build a temporary clot (primary hemostasis) Exposed platelets change shape (pseudopods) Temporary bond between GPIb and vWF Stimulated platelets expose membrane glycoproteins IIb and IIIa IIb and IIIa bind fibrinogen and vWF more platelets are recruited and aggregated -temporary bond depends on high shear stress and is the main interaction that slows platelets down. -high shear stress is present in areas of endothelial injury
 Exposed platelets change shape (pseudopods) Temporary bond between GPIb and vWF. Stimulated platelets expose membrane glycoproteins IIb and IIIa. IIb and IIIa bind fibrinogen and vWF. more platelets are recruited and aggregated. -temporary bond depends on high shear stress and is the main interaction that slows platelets down. -high shear stress is present in areas of endothelial injury.")
17
Platelet Adhesion Binding of GPIIbIIIa to
1. subendothelial vWF secures stable platelet adhesion to the vessel wall while its 2. binding to fibrinogen facilitates platelet Aggregation

18
Platelet Aggregation Aggregation:
Platelets are laced together through fibrinogen bridges Locally thrombin converts the fibrinogen to fibrin stabilizing the platelet plug

19
Platelet Activation Ligand-Receptor interactions
Leads to intracellular signalling Exposure of GpIIb/IIIa Release of dense and alpha granules

20
3 different types of granules
2020 3 different types of granules -lysosomes (for intracellular protein degradation) -dense granules (delta) -alpha granules Electrone Dense granules contain non-protein platelet AGONISTS: calcium, serotonin and non-metabolic pool of ADP and ATP. There are 3-8 dense granules per platelet. Calcium content makes them appear dense under e-microsope. Release of contents promote platelet activation Alpha granules are the predominant granules, about 50 per platelet. Broad variety of proteins: 1. adhesive proteins (vWF, fibrinogen, fibronectin, GPIIb/IIIa) 2. procoagulant factors (factors 5, 11, 13) 3. anticoagulant factors (Prot S) 4. anti-lytic factors (PAI-1) 5. anti-heparin s (PF4) 6. growth-promoting factors (PDGFR, TGF-beta) Platelet AGONISTS Calcium Serotonin ADP/ATP Thromboxane A2 vWF, fibrinogen, clotting factors Anticoagulants (protein S) Anti-heparins ( PF4)
 -dense granules (delta) -alpha granules. Electrone Dense granules contain non-protein platelet AGONISTS: calcium, serotonin and non-metabolic pool of ADP and ATP. There are 3-8 dense granules per platelet. Calcium content makes them appear dense under e-microsope. Release of contents promote platelet activation. Alpha granules are the predominant granules, about 50 per platelet. Broad variety of proteins: 1. adhesive proteins (vWF, fibrinogen, fibronectin, GPIIb/IIIa) 2. procoagulant factors (factors 5, 11, 13) 3. anticoagulant factors (Prot S) 4. anti-lytic factors (PAI-1) 5. anti-heparin s (PF4) 6. growth-promoting factors (PDGFR, TGF-beta) Platelet AGONISTS. Calcium. Serotonin. ADP/ATP. Thromboxane A2. vWF, fibrinogen, clotting factors. Anticoagulants (protein S) Anti-heparins ( PF4)")
21
2121 Platelet Activation New platelets stick to activated platelets and are themselves activated through release of compounds that further amplify platelet activation These include (a) Products of oxidation of arachidonic acid by the cyclooxygenase pathway that includes thromboxane A2 (this pathway is blocked by aspirin=Cox 1 inhibitor)*** (b) ADP released from dense granules
 Products of oxidation of arachidonic acid by the cyclooxygenase pathway that includes thromboxane A2 (this pathway is blocked by aspirin=Cox 1 inhibitor)*** (b) ADP released from dense granules.")
22
Resultant intracellular signaling events lead to platelet activation
Binding of GPIIbIIIa to subendothelial vWF secures stable platelet adhesion to the vessel wall while its binding to fibrinogen facilitates platelet aggregation -Resultant intracellular signaling events lead to platelet activation -Binding of GPIIbIIIa to subendothelial vWF secures stable platelet adhesion to the vessel wall while its binding to fibrinogen facilitates platelet aggregation From: Mechanisms in Hematology 22

23
Summary of Platelet Plug Formation
2323 Summary of Platelet Plug Formation Adhesion Platelets adhere to damaged vessel wall directly via collagen or indirectly via von Willebrand factor Activation Excitatory agonists (collagen, thromboxane A2, etc) cause a conformational change in platelet to expose Glycoprotein IIbIIIa binding sites for fibrinogen Aggregation Platelets are laced together through fibrinogen bridges Fibrin formation Locally thrombin converts the fibrinogen to fibrin stabilizing the platelet plug
 cause a conformational change in platelet to expose Glycoprotein IIbIIIa binding sites for fibrinogen. Aggregation. Platelets are laced together through fibrinogen bridges. Fibrin formation. Locally thrombin converts the fibrinogen to fibrin stabilizing the platelet plug.")
24
Platelet Plug- primary hemostasis Prevention of Bleeding:
Scaffold for secondary hemostasis Prevention of Bleeding: Basis for second part of coagulation scaffolding Platelet plug forms 24

25
Coagulation phase: Clotting factors
Through two different pathways, the clotting cascade is activated and fibrinogen is converted into fibrin Secondary hemostasis

26
Clotting factors fill in gaps (clotting cascade makes fibrin,
Coagulation Phase Prevention of Bleeding: Clotting factors fill in gaps (clotting cascade makes fibrin, the “glue” of a clot)
")
27
Clotting factors Usually referred to by number (except prothrombin and fibrinogen) Numbers written as Roman numerals 13 known procoagulants

28
Coagulation Cascade Series of enzymatic reactions
Activated when collagen, tissue factor or negatively charged surfaces are exposed Key reaction: production of thrombin Thrombin converts fibrinogen to fibrin

29
THE CLOTTING MECHANISM
INTRINSIC EXTRINSIC Collagen Tissue Thromboplastin XII XI VII IX Hemophilia B Hemophilia A VIII X COMMON PATHWAY V FIBRINOGEN (I) PROTHROMBIN THROMBIN (II) (IIa) FIBRIN
 PROTHROMBIN THROMBIN. (II) (IIa) FIBRIN.")
30
Common Pathway Xa with V, Calcium and phospholipid convert prothrombin (II) to thrombin (IIa) “Prothrombinase complex” occurs on platelet surface Thrombin has many substrates both procoagulant ( positive feedback loop) and anticoagulant ( negative feedback)
 and anticoagulant ( negative feedback)")
31
THE CLOTTING MECHANISM
INTRINSIC EXTRINSIC Collagen Tissue Thromboplastin= Tissue Factor (TF) XII XI VII IX VIII X V FIBRINOGEN (I) PROTHROMBIN THROMBIN (II) (IIa) FIBRIN (clot)
 XII. XI. VII. IX. VIII. X. V. FIBRINOGEN. (I) PROTHROMBIN THROMBIN. (II) (IIa) FIBRIN (clot)")
32
Extrinsic Pathway Precipitating event is exposure of tissue factor to blood Tissue factor is a membrane protein which acts as cofactor for VIIa Phospholipid, tissue factor and VIIa cleaves X Xa

33
Intrinsic System Independent of VII
Contact activation of XII activates XI =contact to negatively charged surfaces (kaolin, celite, silica) XIa activates IX IXa with VIII can activate X In vivo there is likely not a strict separation of these two pathways 33
 XIa activates IX. IXa with VIII can activate X. In vivo there is likely not a strict separation of these two pathways. 33.")
34
THE CLOTTING MECHANISM
INTRINSIC EXTRINSIC Collagen Tissue Thromboplastin XII XI VII IX VIII X V FIBRINOGEN (I) PROTHROMBIN THROMBIN (II) (IIa) FIBRIN (=clot)
 PROTHROMBIN THROMBIN. (II) (IIa) FIBRIN (=clot)")
35
Formation of a Fibrin Clot-last step
Thrombin binds to fibrinogen and liberates fibrinopeptides A and B Fibrin monomers form polymers by overlapping and interact laterally to form fibrin strands and sheets Factor XIII cross links fibrin for a stable clot 35

36
Role of Vitamin K Factors II, VII, IX and X
undergo vitamin K dependent gamma carboxylation Reaction occurs in the liver The anticoagulants protein C and S also are carboxylated 36

37
Thrombin Fibrinogen Fibrin 37

38
Prothrombin Xa Va Thrombin Fibrinogen Fibrin 38

39
Extrinsic Pathway TF Prothrombin VIIa Xa Va Thrombin Fibrinogen Fibrin
39

40
Intrinsic pathway XIIa Extrinsic Pathway XIa TF Prothrombin IXa VIIa
VIIIa Xa Va Thrombin Fibrinogen Fibrin 40

41
Intrinsic pathway XIIa Extrinsic Pathway XIa TF Prothrombin IXa VIIa
VIIIa Xa Va Soft clot Thrombin Fibrinogen Fibrin XIIIa Hard clot Fibrin 41

42
Intrinsic pathway XIIa Extrinsic Pathway XIa TF Prothrombin IXa VIIa
VIII VIIIa Xa Va V + + Soft clot Thrombin Fibrinogen Fibrin XIIIa Hard clot + Fibrin 42

43
Control of Coagulation
Normal balance towards anticoagulation Fibrinolysis=clot breakdown Antithrombin III=natural anticoagulant Proteins C and S=natural anticoagulants 43

44
Natural Anticoagulants: AT III, protein C, S
TFPI TF+ VIIa IX+VIII X+V II Fibrinolysis CLOT Degradation of Factors V, VIII Protein C and Protein S Thrombin together with Thrombomodulin activates Protein C and Protein C with cofactor protein S leads to degradation of Factors V and VIII Antithrombin Forms complex with thrombin and other serine proteases Inhibits activated blood clotting factors, especially Factors II and X Heparin potentiates the anticoagulant effect Antithrombin Heparin Thrombin

45
Natural Anti-Coagulants
Spreading clot beyond where it is needed- limited by “anti-clotting” factors Natural anti-clotting factors (Protein C, Protein S, Antithrombin)
")
46
Extra clot and old clot “cleaned-up” by factors that “chew up” clot
Fibrinolysis Extra clot and old clot “cleaned-up” by factors that “chew up” clot Clot breakdown system (fibrinolysis)
")
47
Fibrinolysis Plasmin Fibrin Fibrin Split Products (FSP) 47
 47")
48
Fibrinolytic phase Lysis (=breakdown) of clot allows repair of vessel wall/tissue injury and normalizes flow through vessel Fibrin is degraded by plasmin Plasmin originated from plasminogen Plasminogen is activated by tissue plasminogen activator (TPA) Fibrinolysis is inhibited by plasminogen activator inhibitors and alpha2-antiplasmin
 Fibrinolysis is inhibited by plasminogen activator inhibitors and alpha2-antiplasmin.")
49
Fibrinolysis Plasminogen tPA Plasmin Fibrin
INHIBITORS of PLASMINOGEN Plasminogen activator inhibitor (PAI-1) inhibits Plasminogen Alpha 2 antiplasmin tPA Plasmin Fibrin Fibrin Split Products (FSP) D-Dimer 49
 inhibits Plasminogen. Alpha 2 antiplasmin. tPA. Plasmin. Fibrin. Fibrin Split Products (FSP) D-Dimer. 49.")
50
Commonly Used Pharmacologic Agents in Bleeding
Hemostatic tranexamic acid (Cyklokapron): 5% mouthwash for prolonged bleeding in dentistry, antifibrinolytic aminocaproic acid (Amikar): inhibits plasmin, antifibrinolytic, oral rinse, iv or tablets Aprotonin(Trasylol), antifibrinolytic, withdrawn from Market Activated factor VII, recombinant, bypasses intrinsic system
: 5% mouthwash for prolonged bleeding in dentistry, antifibrinolytic. aminocaproic acid (Amikar): inhibits plasmin, antifibrinolytic, oral rinse, iv or tablets. Aprotonin(Trasylol), antifibrinolytic, withdrawn from Market. Activated factor VII, recombinant, bypasses intrinsic system.")
51
Summary Hemostasis Depends on -vessel wall integrity
-adequate platelet number -adequate Platelet function -adequate factor levels -adequate fibrinolysis

52
Objectives 1. Overview of coagulation 2. Basic coagulation tests
3. Bleeding disorders

53
Basic coagulation tests
1. Platelet count 2. Bleeding Time/Platelet function testing 3. Prothrombin time (PT)/INR 4. aPTT (activated partial Thromboplastin time) 5. Thrombin Time (TT) 6. Factor assay 7. D-Dimer
/INR. 4. aPTT (activated partial Thromboplastin time) 5. Thrombin Time (TT) 6. Factor assay. 7. D-Dimer.")
55
SEVERITY OF THROMBOCYTOPENIA
Normal >150,000/mm3 Mild ,000/mm3 Moderate ,000/mm3 Severe ,000/mm3 Very Severe <5,000/mm3

56
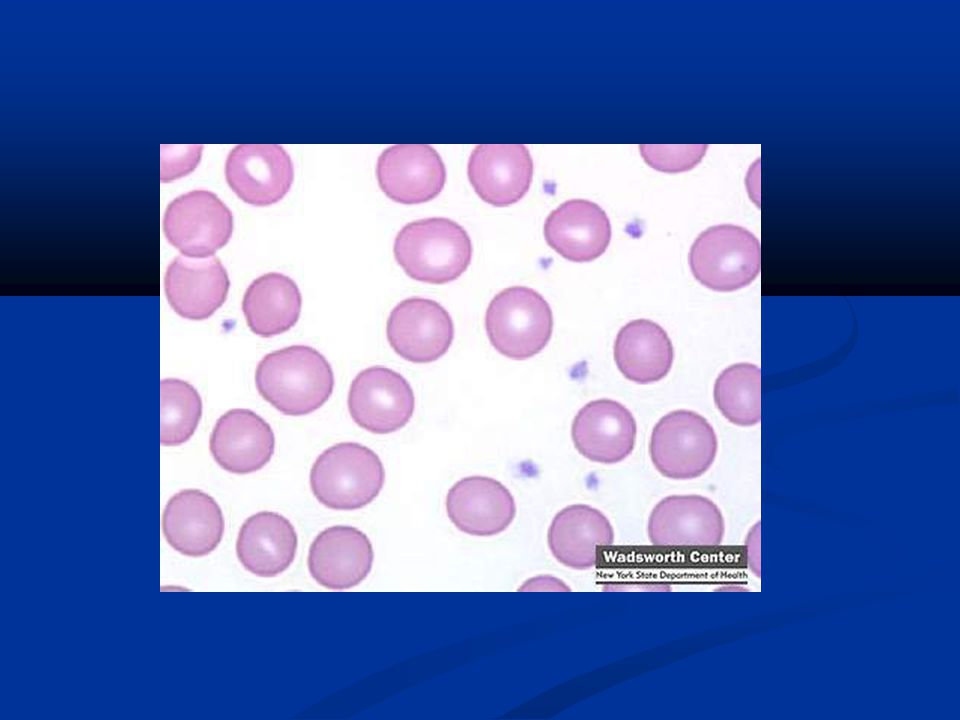
Thrombocytopenia (=low platelet count)
Normal platelet count between 150, ,000/ul Platelets 20–50,000: may see spontaneous hemorrhage and increased risk of hemorrhage with trauma or surgery So safe platelet count for surgery is generally 50,000 or higher Platelets <10,000-20,000: can see life- threatening spontaneous hemorrhage

57
Maslak, P. ASH Image Bank 2008;2008:8-00089
5757 Figure 1. This picture demonstrates petechiae in dependent areas of a thrombocytopenic patient with AML Maslak, P. ASH Image Bank 2008;2008: Copyright ©2008 American Society of Hematology. Copyright restrictions may apply.

58
Basic coagulation tests
1. Platelet count 2. Bleeding Time/Platelet function testing 3. Prothrombin time (PT)/INR 4. aPTT (activated partial Thromboplastin time) 5. Thrombin Time (TT) 6. Factor assay 7. D-Dimer
/INR. 4. aPTT (activated partial Thromboplastin time) 5. Thrombin Time (TT) 6. Factor assay. 7. D-Dimer.")
59
Bleeding Time/Platelet function analyzer
Bleeding time measures platelet function, vessel wall and skin integrity A template device makes a cut on the forearm and time to clot (2-9 minutes) is measured Platelet function analyzer (PFA) can determine an in vitro bleeding time with agonists
 is measured. Platelet function analyzer (PFA) can determine an in vitro bleeding time with agonists.")
60
Bleeding time Old test to screen for vW Disease
or other platelet function disorder Operator dependent, not reproducible Elevated in patients with uremia and liver disease-little prognostic value Also prolonged in patients taking ASA or NSAIDS Does not correlate with bleeding complications Not helpful-please do not order!

61
Platelet function screen
Replaces the bleeding time as a test of platelet function PFA-100; ordered as “platelet function screen” Blue top tube Measures the time it takes for blood to block membrane coated with platelet agonists ( either collagen/epinephrine or collagen/ADP)
")
62
Basic coagulation tests
1. Platelet count 2. Bleeding Time/Platelet function testing 3. Prothrombin time (PT)/INR 4. aPTT (activated partial Thromboplastin time) 5. Thrombin Time (TT) 6. Factor assay 7. D-Dimer
/INR. 4. aPTT (activated partial Thromboplastin time) 5. Thrombin Time (TT) 6. Factor assay. 7. D-Dimer.")
63
Prothrombin time (PT) Measures extrinsic pathway
Useful for measurement of VII, X, V and II and fibrinogen Calcium and thromboplastin (extract of tissue) added to citrated plasma and time to clotting is measured in seconds PT is sensitive to decreased levels of Vitamin K- dependent factors (exception factor IX), useful for monitoring oral anticoagulants (WARAFRIN) Test results expressed in seconds
 added to citrated plasma and time to clotting is measured in seconds. PT is sensitive to decreased levels of Vitamin K- dependent factors (exception factor IX), useful for monitoring oral anticoagulants (WARAFRIN) Test results expressed in seconds.")
64
THE CLOTTING MECHANISM
INTRINSIC EXTRINSIC Collagen Tissue Thromboplastin XII Measured by PT XI VII IX VIII X V FIBRINOGEN (I) PROTHROMBIN THROMBIN (II) (III) FIBRIN
 PROTHROMBIN THROMBIN. (II) (III) FIBRIN.")
65
INR For monitoring oral anticoagulants (warfarin, coumadin) expressed as INR (International Normalized Ratio) Devised to correct for variations in instrumentations and reagents ( tissue thromboplastin) Normal INR is 1.0 Therapeutic anticoagulation is 2-3 ( for A fib, DVT, PE), occasionally ( for artificial valves)
 Normal INR is 1.0. Therapeutic anticoagulation is 2-3 ( for A fib, DVT, PE), occasionally ( for artificial valves)")
66
INR equation [Patient PT/Mean Normal PT]ISI=INR
ISI=international sensitivity index INR=international normalized ratio
![INR equation [Patient PT/Mean Normal PT]ISI=INR](http://slideplayer.com/slide/3382721/17/images/66/INR+equation+%5BPatient+PT%2FMean+Normal+PT%5DISI%3DINR.jpg "ISI=international sensitivity index. INR=international normalized ratio.")
67
Basic coagulation tests
1. Platelet count 2. Bleeding Time/Platelet function testing 3. Prothrombin time (PT)/INR 4. aPTT (activated partial Thromboplastin time) 5. Thrombin Time (TT) 6. Factor assay 7. D-Dimer
/INR. 4. aPTT (activated partial Thromboplastin time) 5. Thrombin Time (TT) 6. Factor assay. 7. D-Dimer.")
68
THE CLOTTING MECHANISM
INTRINSIC EXTRINSIC Collagen Tissue Thromboplastin XII XI VII Measured by PTT IX VIII X V FIBRINOGEN (I) PROTHROMBIN THROMBIN (II) (III) FIBRIN
 PROTHROMBIN THROMBIN. (II) (III) FIBRIN.")
69
Activated Partial thromboplastin time (aPTT)
Measures the intrinsic pathway Surface activating agent and phospholipid is added to citrated plasma Activated plasma is then recalcified and time to clotting measured in seconds

70
aPTT Measures the activity of the entire clotting pathway except Factor VII ( because Factor VII is extrinsic pathway) Useful to detect Factor VIII, IX, XI, XII deficiencies Sensitive to inhibition by heparin and fibrin split products

71
Basic coagulation tests
1. Platelet count 2. Bleeding Time/Platelet function testing 3. Prothrombin time (PT)/INR 4. aPTT (activated partial Thromboplastin time) 5. Thrombin Time (TT) 6. Factor assay 7. D-Dimer 8. Bleeding Time/Platelet function testing
/INR. 4. aPTT (activated partial Thromboplastin time) 5. Thrombin Time (TT) 6. Factor assay. 7. D-Dimer. 8. Bleeding Time/Platelet function testing.")
72
Thrombin Time Excess thrombin is added to plasma
Measure the rate of conversion of fibrinogen to fibrin upon the addition of thrombin to plasma Prolonged in the presence of heparin, low or abnormal fibrinogen and fibrinogen/fibrin degradation products

73
THE CLOTTING MECHANISM
INTRINSIC EXTRINSIC Collagen Tissue Thromboplastin XII XI VII IX VIII X COMMON PATHWAY V FIBRINOGEN (I) PROTHROMBIN THROMBIN (II) (III) FIBRIN
 PROTHROMBIN THROMBIN. (II) (III) FIBRIN.")
74
Basic coagulation tests
1. Platelet count 2. Bleeding Time/Platelet function testing 3. Prothrombin time (PT)/INR 4. aPTT (activated partial Thromboplastin time) 5. Thrombin Time (TT) 6. Factor assay 7. D-Dimer
/INR. 4. aPTT (activated partial Thromboplastin time) 5. Thrombin Time (TT) 6. Factor assay. 7. D-Dimer.")
75
Factor assay Each of the factors is individually assayed using modifications of the PT or PTT test Pooled normal plasma is defined as 100% activity Factor levels vary tremendously from person to person ( normal is % activity)
")
76
Basic coagulation tests
1. Platelet count 2. Bleeding Time/Platelet function testing 3. Prothrombin time (PT)/INR 4. aPTT (activated partial Thromboplastin time) 5. Thrombin Time (TT) 6. Factor assay 7. D-Dimer
/INR. 4. aPTT (activated partial Thromboplastin time) 5. Thrombin Time (TT) 6. Factor assay. 7. D-Dimer.")
77
Intrinsic pathway XIIa Extrinsic Pathway XIa TF Prothrombin IXa VIIa
VIII VIIIa Xa Va V + + Soft clot Thrombin Fibrinogen Fibrin XIIIa Hard clot + Fibrin 77

78
D-Dimer Fibrin monomer bind to form thrombus
Factor XIII binds their D-domains together Fibrinolysis: Degradation fragment is called D- Dimer D-Dimer is a fibrin split product

79
D-Dimer Elevated D-Dimer levels indicate that
1) Thrombin has acted on fibrinogen to form a fibrin monomer which bonded to another monomer aided by Factor XIII 2) clot was lysed by plasmin (=fibrinolysis)
 Thrombin has acted on fibrinogen to form a fibrin monomer which bonded to another monomer aided by Factor XIII. 2) clot was lysed by plasmin (=fibrinolysis)")
80
Objectives 1. Overview of coagulation 2. Basic coagulation tests
3. Bleeding disorders

81
Evaluation of Bleeding
Patients may consider an appropriate amount of bruising or bleeding to be excessive Therefore, a detailed history is essential in the workup

82
Approach to the bleeding patient- History is the most important tool
1. Have you ever had a nosebleed? How frequent did these occur? Did it require a trip to the hospital? 2. Have you ever had dental work? Did it require stitching or packing due to the bleeding? Did it bleed the next day? 3. What surgeries have you undergone? Did any of them require transfusions? Did your surgeon comment on excessive bleeding? 4. What is the biggest bruise you ever had? How did it happen? 5. How long are your menstrual periods? Have you ever been so anemic you needed to be on iron replacement? Did you have excessive bleeding after childbirth or require a transfusion then? 6. Have you ever had bleeding when you urinated, from your stomach or from your gastrointestinal tract? 7. Do you bleed when you brush your teeth? From Hemostasis and Thrombosis; 1999Landes Bioscience

83
Approach to the bleeding patient
1. History/Severity of symptoms: Major vs. Minor bleeding, menorrhagia, bruising, nosebleeds (Acquired vs. inherited) 2. Prior stressors (contact sports, trauma, broken bones, surgeries, pregnancies) 3. Family History (extended, especially males) 4. Drugs (Rx plus OTC) 5. Previous coagulation parameters available? (PT, PTT, platelet count) 6. Concurrent illnesses
 2. Prior stressors (contact sports, trauma, broken bones, surgeries, pregnancies) 3. Family History (extended, especially males) 4. Drugs (Rx plus OTC) 5. Previous coagulation parameters available (PT, PTT, platelet count) 6. Concurrent illnesses.")
84
Case A 40 y/o woman presents to your office for dental evaluation. She will need extraction of several teeth. Years ago, she had wisdom teeth extraction performed and tells you that she started to bleed about 4 hrs after extraction and needed plasma transfusion to stop the bleeding. She is very apprehensive about any further extractions. You order the following labs: CBC shows normal platelets count at 267. PT is normal at 12.3 sec, PTT is normal at 28 sec. INR is 1.0. Platelet function testing is normal. She also tells you that she bled each time after her deliveries ( she has 4 children) where she lost enough blood to receive blood transfusions each time. She bled after her gallbladder surgery and her tonsillectomy. You tell her: A) based on her history, she must have a bleeding disorder B) you don’t think, she has a bleeding disorder because all of her testing has been normal C) you think, she must have had an incompetent surgeon/dentist before and YOU will be more careful D) you think, she needs more testing
 where she lost enough blood to receive blood transfusions each time. She bled after her gallbladder surgery and her tonsillectomy. You tell her: A) based on her history, she must have a bleeding disorder. B) you don’t think, she has a bleeding disorder because all of her testing has been normal. C) you think, she must have had an incompetent surgeon/dentist before and YOU will be more careful. D) you think, she needs more testing.")
85
Bleeding disorders Inherited bleeding disorders
Von Willebrands disease Hemophilia A and B Other factor deficiencies Acquired bleeding disorders Thrombocytopenia Liver disease Vitamin K deficiency/warfarin overdose DIC Renal disease/uremia Drug induced (ASA)
")
86
Bleeding disorders 1. Vessel defects 2. Platelet disorders
3. Coagulation abnormalities 4. Other

87
Vessel defects 1. Vitamin C deficiency 2. Bacterial/viral infections
3. Rheumatologic disorders (vasculitis)
")
88
Vessel wall integrity Peri-follicular hemorrhage Scorbutic gingivitis

89
Bleeding disorders 1. Vessel defects 2. Platelet disorders
3. Coagulation abnormalities 4. Other

90
Platelet disorders Thrombocytopenia ( decreased numbers of platelets)
Platelet function defects ( abnormal platelet function)
")
91
Thrombocytopenia (=low platelet count)
Normal platelet count between 150, ,000/ul Platelets 20–50,000: may see spontaneous hemorrhage and increased risk of hemorrhage with trauma or surgery So safe platelet count for surgery is generally 50,000 or higher Platelets <10,000-20,000: can see life-threatening spontaneous hemorrhage

92
Causes of Thrombocytopenia
Caused by either of these mechanisms: Decreased production of platelets Increased destruction of platelets Distribution/Dilution disorders (Increased sequestration of platelets due to splenomegaly)
")
93
Do not blanch with pressure Not palpable
Petechiae Do not blanch with pressure Not palpable

94
Impaired/Decreased Platelet production
Bone marrow failure -nutritional deficiencies ( Vitamin B12, Folate) -ETOH -malignancies ( leukemia, lymphoma, metastatic disease to bone marrow, myelodysplastic syndrome) -Drug-induced (chemotherapy , antibiotics, thiazide diuretics etc) -Radiation ( marrow in Radiation field) -Viral infections (HIV, Hep C) -congenital
 -ETOH. -malignancies ( leukemia, lymphoma, metastatic disease to bone marrow, myelodysplastic syndrome) -Drug-induced (chemotherapy , antibiotics, thiazide diuretics etc) -Radiation ( marrow in Radiation field) -Viral infections (HIV, Hep C) -congenital.")
95
Disorders causing Increased Destruction of Platelets
Thrombocytopenia occurs when platelets are rapidly destroyed and bone marrow cannot compensate Most common cause is immune thrombocytopenia where platelets are coated with anti-platelet antibodies leading to premature removal of platelets by the spleen Disorders: Immune thrombocytopenia (ITP) – common cause (outpatient) DIC – rare cause (usually inpatient setting) Sepsis – rare cause (inpatient) Thrombotic thrombocytopenic purpura (TTP) – rare cause, inpatients
 – common cause (outpatient) DIC – rare cause (usually inpatient setting) Sepsis – rare cause (inpatient) Thrombotic thrombocytopenic purpura (TTP) – rare cause, inpatients.")
96
Thrombocytopenia ITP ( immune thrombocytopenic purpura)
Autoimmune disorder caused by antibodies that lead to destruction of platelets

97
Disorders of dilution/distribution
Active bleeding or clotting (consumption) Massive transfusion (dilution) Hypersplenism ( sequestration of platelets in enlarged spleen) -normally 30% of platelets stored in spleen -with increase in size, more platelets get sequestered in spleen -most often seen in Liver disease ( Liver cirrhsois)->portal hypertension->splenomegaly
 Massive transfusion (dilution) Hypersplenism ( sequestration of platelets in enlarged spleen) -normally 30% of platelets stored in spleen. -with increase in size, more platelets get sequestered in spleen. -most often seen in Liver disease ( Liver cirrhsois)->portal hypertension->splenomegaly.")
98
Abnormal platelet function (platelet number normal)
1. Drug induced ( aspirin, NSAIDs, Plavix) -stop aspirin 5-7 days before elective surgery 2. uremia 3. congenital platelet function defects (Glanzman thrombasthenia, Bernard-Soulier syndrome-missing platelet receptor proteins)
 -stop aspirin 5-7 days before elective surgery. 2. uremia. 3. congenital platelet function defects. (Glanzman thrombasthenia, Bernard-Soulier syndrome-missing platelet receptor proteins)")
99
Bleeding disorders 1. Vessel defects 2. Platelet disorders
3. Coagulation abnormalities 4. Other

100
Hemophilia X-linked deficiency of Factor VIII (hemophilia A) or Factor IX (hemophilia B) Males primarily affected Carrier females can be symptomatic Elevated PTT is only abnormal screening test 100

101
Hemophilia A and B Hemophilia A – Factor VIII deficiency 1:5000 male births Hemophilia B – Factor IX deficiency 1:50,000 male births Many new mutations; negative family history does not rule out hemophilia 101

102
Diagnosis of Hemophilia
Screen males with unexplained hematomas, bruises and post surgical or traumatic bleeding PTT ranges from high normal to very prolonged Assay Factor activity to distinguish Hemophilia A and B-important for treatment 102

103
Hemophilia-Clinical manifestations
Clinical manifestations (hemophilia A & B indistinguishable) Hemarthrosis (most common) Fixed joints Soft tissue hematomas (e.g., muscle) Muscle atrophy Shortened tendons Other sites of bleeding Urinary tract CNS, neck (may be life-threatening) Prolonged bleeding after surgery or dental extractions 103
 Hemarthrosis (most common) Fixed joints. Soft tissue hematomas (e.g., muscle) Muscle atrophy. Shortened tendons. Other sites of bleeding. Urinary tract. CNS, neck (may be life-threatening) Prolonged bleeding after surgery or dental extractions")
104
Ecchymoses (typical of coagulation factor disorders)
")
105
105

106
106

107
107

108
Coagulation Factor Testing
Pooled normal plasma is defined as 100% activity Normals are ~50-150% activity Severe hemophilia - <1% - spontaneous bleeds Moderate 2-5%-bleed with minor trauma Mild hemophilia 5-10% - bleed with severe trauma, surgery and dental procedures Factor Level does not change significantly throughout life! 108

109
Factor XI Deficiency PTT prolonged Post-operative bleeding
Variable bleeding history Autosomal recessive Variable incidence in populations 109

110
Hemophilia Hemophilia A Hemophilia B Factor XI deficiency
Affected Coagulation factor F VIII F IX F XI Inheritance X linked recessive Autosomal recessive Incidence 1/5,000 males 1/50,000 males Ashkenazi Jews (5% of population

111
Treatment of hemophilia A: Factor VIII concentrates
Preferred agent: recombinant goal range : 30-40% factor level hemorrhagic joints 100% factor level in patients undergoing major surgery or CNS trauma infuse as fast as possible 1 unit of factor VIII raises plasma level by 2% (Desired Factor VIII concentration x weight in kg 2

112
Bleeding disorders 1. Vessel defects 2. Platelet disorders
3. Coagulation abnormalities 4. Other

113
Von Willebrand Disease
Most common congenital bleeding disorder Autosomal dominant Abnormality in platelet/endothelial interaction Clinical problems: Mucosal bleeding Nose bleeds GI bleeds Menorrhagia Bleeding after surgery if no correction

114
Von Willebrand Disease: Pathophysiology
Von Willebrand’s protein is extremely large protein in a series of forms with 2 functions 1ST FUNCTION: Adheres platelets to exposed collagen at the site of a wound or vessel disruption 2nd FUNCTION: Carry Factor VIII Without this protein, Factor VIII has a VERY short half- life

115
Von Willebrand Disease: Diagnosis (Initial)
Tests for von Willebrand’s Disease: Factor VIII level normal or decreased (measures 2nd function of vW protein) von Willebrand’s antigen (measures amount of vW protein) < 0.30 IU/dL von Willebrand’s activity, aka ristocetin cofactor activity (measures function of patient’s vW protein using donor platelets) < 0.30 IU/dL Blood Type (Type 0) has lower baseline levels)
 von Willebrand’s antigen (measures amount of vW protein) < 0.30 IU/dL. von Willebrand’s activity, aka ristocetin cofactor activity (measures function of patient’s vW protein using donor platelets) < 0.30 IU/dL. Blood Type (Type 0) has lower baseline levels)")
116
Von Willebrand Disease Types
Type 1: Partial quantitative vWF deficiency. (70-80% cases) Type 2: Qualitative defects – abnormal function of vW protein(15-30% cases) Type 3: Almost complete absence vWF (Rare)
 Type 2: Qualitative defects – abnormal function of vW protein(15-30% cases) Type 3: Almost complete absence vWF (Rare)")
117
Von Willebrand Disease Treatment - DDAVP
Need to avoid aspirin, NSAID’s, other platelet inhibiting drugs Long term prophylaxis rarely required DDAVP (arginine vasopressin) enhances already synthesized vWF release from endothelial stores so effective in type 1 but not type 2 or type 3 disease Once stores depleted, will need time to make more vW factor DDAVP is available as nasal spray (Stimate) or intravenous form Trial in a non-bleeding state is warranted before elective procedure to verify pt will respond with increased levels
 enhances already synthesized vWF release from endothelial stores so effective in type 1 but not type 2 or type 3 disease. Once stores depleted, will need time to make more. vW factor. DDAVP is available as nasal spray (Stimate) or intravenous form. Trial in a non-bleeding state is warranted before elective procedure to verify pt will respond with increased levels.")
118
Von Willebrand Disease Treatment – vWF Replacement Therapy
“Intermediate purity” factor VIII (also rich in vWF) concentrates are most commonly used Mainly used in type 2 and 3 disease Indications in type 1 disease: More severe disease, especially when severe bleeding involved When other measures have failed Post op setting when prolonged treatment maybe needed, because DDAVP will not work repeteadly
 concentrates are most commonly used. Mainly used in type 2 and 3 disease. Indications in type 1 disease: More severe disease, especially when severe bleeding involved. When other measures have failed. Post op setting when prolonged treatment maybe needed, because DDAVP will not work repeteadly.")
119
Case 1 A 23 y/o woman is sent to you for wisdom teeth extraction. On pre-screening form, patient reports “very heavy menses” that have always been present. She works as a hair stylist and has to take off work for her periods. What should you do next? A) inquire about previous surgeries/extractions, i.e. obtain a bleeding history B) Proceed with extractions and see if she bleeds C) Send for hematology evaluation D)Tell the patient that she has a bleeding disorder and deny her surgery.
 inquire about previous surgeries/extractions, i.e. obtain a bleeding history. B) Proceed with extractions and see if she bleeds. C) Send for hematology evaluation. D)Tell the patient that she has a bleeding disorder and deny her surgery.")
120
Case 2 The same patient tells you that she had a vaginal delivery 2 years ago and bled extensively about 8 days after her delivery. She required a Blood transfusion at that time. No obstetric reason for her bleeding was found. She was supposed to see a hematologist at that time but never followed up. What would be the best way to proceed now? A) Obtain a hematology evaluation now B) Assume, she has hemophilia and give a factor concentrate before the extraction C) Assume, she has von Willebrand disease and give DDAVP D) Assume, she has a platelet disorder and arrange for transfusion of platelets before her extraction.
 Obtain a hematology evaluation now. B) Assume, she has hemophilia and give a factor concentrate before the extraction. C) Assume, she has von Willebrand disease and give DDAVP. D) Assume, she has a platelet disorder and arrange for transfusion of platelets before her extraction.")
121
Case 3 The same patient is seen by hematology and is diagnosed with von Willebrand disease, Type I, the most common type. The hematologist most likely will recommend: A) 1 dose of DDAVP i.v. before extraction B) 1 dose of Humate P (Factor VIII) C) Transfusion of platelets before extraction D) Cryoprecipitate before extraction
 1 dose of DDAVP i.v. before extraction. B) 1 dose of Humate P (Factor VIII) C) Transfusion of platelets before extraction. D) Cryoprecipitate before extraction.")
122
Case 4 In a patient with von Willebrand disease, which types of bleeding would you NOT expect? A) nosebleeds B) excessive menstrual bleeding C) joint bleeds ( hemarthrosis) D) post-procedural bleeding
 excessive menstrual bleeding. C) joint bleeds ( hemarthrosis) D) post-procedural bleeding.")
123
Case 5 The same patient eventually undergoes tooth extraction with appropriate pre-treatment and does well. She asks you whether her now 2 y/o son could have von Willebrand disease as well? A) yes, please explain B) no, please explain
 yes, please explain. B) no, please explain.")
124
Bleeding History Pearls***
Mucocutaneous bleeding: Platelet or von Willebrand factor defect Soft Tissue/Joint/Deep Bleeding: Coagulopathy (Factor deficiency=Hemophilia)
")
125
Questions?

Similar presentations








 Thrombocytes. PLATELETS (PLT) Thrombocytes.>")










