Download presentation
Presentation is loading. Please wait.

1
Immunopathology Path 6266 May 18, 2010 Judy Aronson, M.D. Jaronson@utmb.edu

2
Outline How does the immune response damage tissues? –Hypersensitivity mechanisms –Examples of immunopathologic disease –Autoimmune diseases How does autoimmunity occur? –Mechanisms of peripheral tolerance –Lessons from an experimental model of autoimmune diabetes

3
The double edged sword of immune responses “Immunitas”: Freedom from disease Protective responses against infectious agents “Pathos”: Suffering/ disease Host tissue damage by immune response

4
Hypersensitivity reactions Mechanisms of immune-mediated injury Classified into 4 types (I-IV) Imperfect correlation between hypersensitivity reaction and disease syndrome –In some diseases, all 4 types may contribute –Humoral and cell-mediated mechanisms may co- exist
 Imperfect correlation between hypersensitivity reaction and disease syndrome –In some diseases, all 4 types may contribute –Humoral and cell-mediated mechanisms may co- exist")
5
Categories of diseases with immunopathologic components Infectious Allergic Transplant rejection Graft vs. host disease Autoimmune

6
Hypersensitivity Reactions Type I: anaphylactic –allergy, asthma Type II: antibody-mediated –transfusion reaction Type III: immune complex-mediated –post-strep glomerulonephritis Type IV: cell-mediated, delayed type –tuberculosis

7
Type I hypersensitivity Immunoglobulin E (IgE) –made by plasma cells, specific for allergen Mast cells, basophils –Have receptors for Fc portion of IgE molecule –When antigen binds IgE variable regions, degranulation of cells occurs –Histamine and other vasoactive substances are released Severe reactions can be life-threatening!
 –made by plasma cells, specific for allergen Mast cells, basophils –Have receptors for Fc portion of IgE molecule –When antigen binds IgE variable regions, degranulation of cells occurs –Histamine and other vasoactive substances are released Severe reactions can be life-threatening!")
9
Type I hypersensitivity

10
Mast cell mediators Primary mediators –Histamine: vasodilation and increased permeability, bronchoconstriction, mucus secretion –Tryptase: generate kinins, activate complement –Eosinophil chemotactic factor –Neutrophil chemotactic factor Secondary mediators –Lipid mediators (result from PLA2 activation) PAF LTC4, LTD4: vaso- dilation, bronchospasm LTB4: chemotactic factor PGD2: increased mucus, bronchospasm –Cytokines: TNF, IL-1, IL- 4, IL-5, IL-6)
 PAF LTC4, LTD4: vaso- dilation, bronchospasm LTB4: chemotactic factor PGD2: increased mucus, bronchospasm –Cytokines: TNF, IL-1, IL- 4, IL-5, IL-6)")
11
Clinical diseases Systemic anaphylaxis –Urticaria (hives), bronchoconstriction, laryngeal edema, hypersecretion of mucus, vomiting, abdominal cramps –Life threatening Localized reactions—eg urticaria, hay fever Asthma
, bronchoconstriction, laryngeal edema, hypersecretion of mucus, vomiting, abdominal cramps –Life threatening Localized reactions—eg urticaria, hay fever Asthma")
12
Urticaria (hives)
")
13
Asthma

14
Type II hypersensitivity Involves IgG or IgM antibodies that react with fixed antigen on cells or tissue components Mechanisms of damage: –cell lysis (complement, MAC) –inflammation (complement activation) –block normal cell function –stimulate excessive cell function
 –inflammation (complement activation) –block normal cell function –stimulate excessive cell function")
15
Complement A system of about 20 serum proteins Activation is by a proteolytic cascade mechanism –Classical pathway: initiated by Ag-Ab complexes –Alternative pathway: initiated by microbial surface Important products are formed at activating cell surface (opsonins, MAC) and in aqueous environment (anaphylatoxins)
 and in aqueous environment (anaphylatoxins)")
16
Overview of complement activation pathways From: Robbins

17
Complement: Effector functions Formation of membrane attack complex, lysis of target cell Generation of C3a and C5a “anaphylatoxins” –Chemotactic factors for phagocytes, esp. pmn –Leukocyte activation –Mast cell degranulation –Bronchoconstriction Opsonization—coating surface of target cell with C fragments (esp. C3), promoting phagocytosis
, promoting phagocytosis.")
18
Downloaded from: Robbins & Cotran Pathologic Basis of Disease (on 2 January 2007 07:24 PM) © 2005 Elsevier Activation and effector functions of complement
 © 2005 Elsevier Activation and effector functions of complement")
19
The Lytic Pathway of Complement From: Roitt

20
Biological Effects of C5a From: Roitt

21
Opsonization and phagocytosis From: Roitt

22
Type II Hypersensitivity

23
ABO antigens and transfusion

24
Type III hypersensitivity Caused by immune complexes (antigen- antibody) that are soluble and formed in antigen excess Circulating immune complexes deposited according to size, charge, local hemodynamics, etc. (e.g. glomeruli of kidney, joints, skin, small vessels) Complement is activated, inflammation ensues
 Complement is activated, inflammation ensues.")
25
Type III (Immune complex) Hypersensitivity
 Hypersensitivity")
26
Normal glomerulus

28
Immune complex glomerulonephritis

29
HBV: Immune complex GN

31
Question to consider, buzz group In a patient with ongoing or active type III hypersensitivity reaction, would you expect the following components in the systemic circulation to be increased, decreased, or unchanged, compared to baseline for the patient? –C3 –C4 –Total complement (CH50)
.")
32
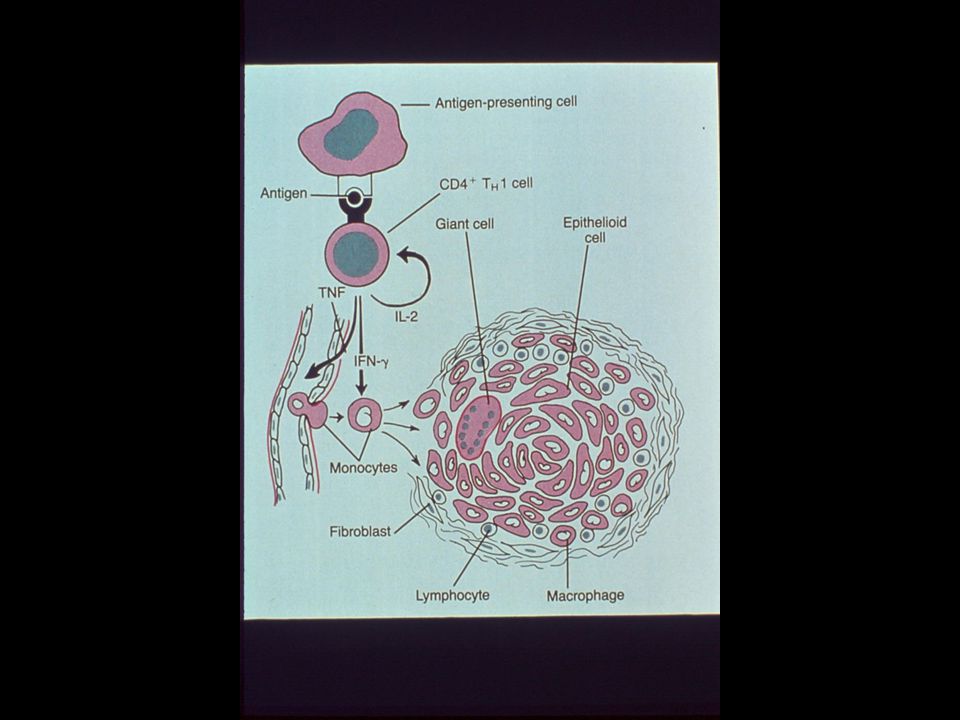
Type IV hypersensitivity T lymphocytes and macrophages are effector cells (cell-mediated immune reactions) Macrophages activated by T cell cytokines (interferon gamma) make granulomas TB is classic example of delayed type hypersensitivity (DTH)
 Macrophages activated by T cell cytokines (interferon gamma) make granulomas TB is classic example of delayed type hypersensitivity (DTH)")
33
T cells have multiple effector functions

40
Non-cytopathic virus interactions with host Zinkernagel, 1997

41
Effects of antiviral T cells Virus featureProtectionImmunopathology Cytopathic+++Not noticeable Noncytopathic With limited spread Widespread or involving essential organs Putative (unknown) non- cytopathic
 non- cytopathic")
42
Effects of antiviral T cells (from Zinkernagel, 1997) Virus featureProtectionImmunopathology Cytopathic+++Not noticeable Noncytopathic With limited spread +++/- Widespread or involving essential organs ++++ Putative (unknown) non- cytopathic Not noticeable +++
 Virus featureProtectionImmunopathology Cytopathic+++Not noticeable Noncytopathic With limited spread +++/- Widespread or involving essential organs ++++ Putative (unknown) non- cytopathic Not noticeable +++")
43
Autoimmunity Occurs when hypersensitivity mechanisms are directed against “self” antigens Breakdown of “tolerance”

44
Requirements for categorization as autoimmune disorder The presence of an autoimmune reaction Clinical or experimental evidence that such a reaction is of primary pathogenetic significance, not secondary to tissue damage from another cause The absence of another well-defined cause of the disease

45
Autoimmune diseases Systemic –SLE (lupus): anti-nuclear antibodies (ANA) are characteristic joints, skin, kidneys, blood, heart, and brain can be involved (type III hypersensitivity) –Rheumatoid arthritis Organ-specific –Graves disease (thyroid) –Multiple sclerosis (brain)
: anti-nuclear antibodies (ANA) are characteristic joints, skin, kidneys, blood, heart, and brain can be involved (type III hypersensitivity) –Rheumatoid arthritis Organ-specific –Graves disease (thyroid) –Multiple sclerosis (brain)")
46
Central and peripheral tolerance

47
Downloaded from: StudentConsult (on 10 May 2008 09:33 PM) © 2005 Elsevier
 © 2005 Elsevier")
48
Downloaded from: StudentConsult (on 10 May 2008 09:33 PM) © 2005 Elsevier
 © 2005 Elsevier")
49
2 1 Experimental evidence for failure of “homeostatic mechanisms” in autoimmunity: –1: Failure of AICD –2: Inappropriate co- stimulatory mol. expression

50
Transgenic mouse model of IDDM No spontaneous diabetes mellitus Exocrine pancreas Islets Transgene is LCMV antigen under the control of rat insulin promoter (RIP-LCMV) Expression of transgene in cells Von Herrath 2002
 Expression of transgene in cells Von Herrath 2002")
51
RIP-LCMV transgenic mouse Adoptive transfer of LCMV-reactive CTL “insulitis” No -cell destruction No IDDM Transgenic mouse model of IDDM

52
Trigger: Infect with LCMV Increased glucose Decreased insulin Beta cell destruction Insulin dependent diabetes mellitus RIP-LCMV transgenic mouse Variable lag time Transgenic mouse model of IDDM

53
Lessons from LCMV-RIP model of IDDM Peripheral tolerance can be broken. This requires: –Activation of APC’s and production of co- stimulatory signals for T cell activation and amplification –Interaction between PBL and islet cells –Upregulation of MHC-II and macrophage activation by viral infection

54
What are the mechanisms of cell destruction in this model? CTL, perforin-dependent lysis initiates insulitis, but cannot by itself cause IDDM Autoreactive CTL cannot lyse -cells without upregulation of MHC-I expression Interferon- (and other inflammatory cytokines) increase MHC-I Beta cell destruction and IDDM required additional direct effect of interferon- from infiltrating CD4 and CD8 cells
 increase MHC-I Beta cell destruction and IDDM required additional direct effect of interferon- from infiltrating CD4 and CD8 cells.")
55
LCMV infects islets and leads to antigen-presenting cell activation (MHC-II expression) before arrival of T lymphocytes –Expansion of infiltrating CD4 and CD8 T cells –Continued T cell attack against cells even after virus is cleared Lessons possibly generalizable to humans? –An “inflammatory environment” facilitates propagation of autoreactive T cells –“Hit and run” model for human autoimmune diseases— disease may be triggered by infection, but continues after agent is cleared Why does LCMV infection cause IDDM in this model, while adoptive transfer of LCMV-reactive T cells does not?

56
Downloaded from: StudentConsult (on 10 May 2008 09:33 PM) © 2005 Elsevier
 © 2005 Elsevier")
57
T regs “Natural” and “induced” populations Inhibit sustained T cell responses and prevent immunopathology (but do not inhibit initial T cell activation) Lack characteristics of Th1 or Th2 cells Selectively express Foxp3, (forkhead/winged helix family transcription factors) CD25 is an activation marker (IL-2R ); operationally, a marker for T reg –Transfer of CD25 depleted T cells from normal mice into syngeneic nude mice>autoimmune diseases
 Lack characteristics of Th1 or Th2 cells Selectively express Foxp3, (forkhead/winged helix family transcription factors) CD25 is an activation marker (IL-2R ); operationally, a marker for T reg –Transfer of CD25 depleted T cells from normal mice into syngeneic nude mice>autoimmune diseases")
58
Some mechanisms of autoimmune disease 1.Failure of activation-induced cell death –Fas or FasL null mice 2.Breakdown of T cell anergy –Increased co-stimulatory molecules in RA synovium, MS, experimental IDDM 3.Molecular mimicry –Streptococcal M protein and cardiac proteins: acute rheumatic fever 4.Polyclonal lymphocyte activation –Superantigen activation of autoreactive T cells 5.Release of sequestered antigens –Post-traumatic uveitis or orchitis 6.Decreased Treg activity

59
Summary Four general mechanisms have been described by which the immune response can damage host cells and tissues –(type I-IV hypersensitivity reactions) Hypersensitivity mechanisms are important in the pathogenesis of allergic, autoimmune, and some infectious diseases The pathogenesis of autoimmune diseases involves failure of peripheral tolerance Inflammation and inflammatory cytokines play important roles in propagating autoimmune reactions
 Hypersensitivity mechanisms are important in the pathogenesis of allergic, autoimmune, and some infectious diseases The pathogenesis of autoimmune diseases involves failure of peripheral tolerance Inflammation and inflammatory cytokines play important roles in propagating autoimmune reactions")
Similar presentations