Download presentation
Presentation is loading. Please wait.

1
Adapted from the Presentation of Medical School - Duluth
The Complement System Adapted from the Presentation of Jean F. Regal, Ph.D. Medical School - Duluth Like the clotting system, the complement system sits around waiting for something to happen and then it jumps into action. Circulating proteins with membrane bound regulators.

2
Learning Objectives Explain the importance of the complement system in host defense and inflammation and the clinical consequences of complement deficiencies. Describe the biochemistry of activation of the three different pathways including the initiators, sequence of reactions, important enzymes, and fragments. List the proteins which control the complement system and where they act. Describe the biological responses mediated by the different complement receptors. Describe the biological effects of complement activation.

3
Complement: Location of Complement Proteins
Complement is not a single protein but a complex of proteins that are found constitutively in the plasma. Complement proteins are present in secretions, such as bronchial fluids, where they protect portals of entry. Complement proteins are present in interstitial fluids where they protect against agents that penetrate the protective barriers (skin, mucosal membranes, etc.).
.")
4
Production of Complement Proteins
The molecular weights of complement proteins range widely from kDa. Complement proteins are synthesized Primarily by liver hepatocytes and by tissue macrophages, Secondarily by epithelial cells, fibroblasts and monocytes. Concentration ranges in plasma: 1 or 2 ug/ml – Mannose-Binding Lectin and Factor D 300 ug/ml – C4 1200 ug/ml – C3 Albumin concentration is ~40 mg/ml with total serum protein being ~60 mg/ml

5
Roles of Complement Complement proteins are activated on demand.
Complement proteins are activated in a cascade. In these ways, complement proteins are similar to clotting proteins. Complement proteins are non-specific proteins that play roles both in the innate immune system and in the adaptive immune system. Destroy bacteria Destroy fungi Destroy viruses

6
Importance of Complement
The complement system is so important to our defense against microorganisms that there are several pathways by which the complement system can be activated. Classical pathway Alternative pathway Mannose-binding lectin pathway (aka, lectin pathway)
")
7
Nomenclature of Complement Proteins
Complement proteins in the common portions of the Classical Pathway Denoted with the letter “C” followed by a number and are named C1 through C9. Proteins in the Mannose-Binding Lectin Pathway are Mannan-binding lectin (MBL) MBL-associated serine protease-1 (MASP-1) MBL-associated serine protease-2 (MASP-2) Proteins in the Alternative Pathway that lead to the common portions of the classical complement pathway Denoted as factors (Factor B and Factor D).
 MBL-associated serine protease-1 (MASP-1) MBL-associated serine protease-2 (MASP-2) Proteins in the Alternative Pathway that lead to the common portions of the classical complement pathway. Denoted as factors (Factor B and Factor D).")
8
Function of the Complement System
The complement system acts as an auxiliary system in immunity, both on its own and in conjunction with humoral immunity. In its role in innate immunity, it is a primitive surveillance and defense system for microbes, independent of T cells and antibodies. In its role in adaptive immunity, it is a major effector system for humoral immunity. Lowest organisms have some aspects of the complement system. Primitive vertebrates like the lamprey and hagfish. Invertebrates such as the horseshoe crab and insects have alternative pathway.

9
Specific Functions of the Complement System
Chemotactic Agent Activator of Inflammation Complement also augments stimulation of B cells through complement receptor 2 (CR2/CD21) to increase the humoral immune response.
 to increase the humoral immune response.")
10
Biochemistry of the Complement System
Activation of the complement system The classical pathway The mannose-binding lectin pathway The alternative pathway Control of complement activation Activation/Inactivation of C4b and C3b Complement receptors

11
Activation of the Classical Pathway

12
Activators Lectin Pathway Classical Pathway Alternative Pathway MBL
MASP-1, MASP-2 C1q C3 + H2O Factor B Factor D C1r2 C1s2 C4 C2 C3 C3 convertase (C4b2a) C3b (Opsonin) C3a C5a C5 convertase (C4b2a3b) C5b C6 C7 C8 C9 Membrane Attack Complex C5 Terminal lytic Pathway Antigen Antibody Complexes (IgG/IgM) Polysaccharides on Microbes; Also IgA Foreign Surfaces (LPS); Spontaneous (Nucleophiles) Activators (Anaphylatoxins)
 C3b (Opsonin) C3a. C5a. C5 convertase (C4b2a3b) C5b C6 C7 C8 C9. Membrane Attack Complex. C5. Terminal lytic Pathway. Antigen Antibody. Complexes (IgG/IgM) Polysaccharides on. Microbes; Also IgA. Foreign Surfaces (LPS); Spontaneous (Nucleophiles) Activators. (Anaphylatoxins)")
13
Complement Sensors Lectin Pathway Classical Pathway
Alternative Pathway MBL MASP-1, MASP-2 C1q C3 + H2O Factor B Factor D C1r2 C1s2 C4 C2 C3 C3 convertase (C4b2a) C3b (Opsonin) C3a C5a C5 convertase (C4b2a3b) C5b C6 C7 C8 C9 Membrane Attack Complex C5 Terminal lytic Pathway Antigen Antibody Complexes (IgG/IgM) Polysaccharides on Microbes; Also IgA Foreign surfaces (LPS); Spontaneous (Nucleophiles) Activators Complement Sensors (Anaphylatoxins)
 C3b (Opsonin) C3a. C5a. C5 convertase (C4b2a3b) C5b C6 C7 C8 C9. Membrane Attack Complex. C5. Terminal lytic Pathway. Antigen Antibody. Complexes (IgG/IgM) Polysaccharides on. Microbes; Also IgA. Foreign surfaces (LPS); Spontaneous (Nucleophiles) Activators. Complement. Sensors. (Anaphylatoxins)")
14
2 IgG/1 IgM C1q C1q C1r C1r C1s C1s C4 C4b
Activation of C1 C1 is present in plasma as an inactive C1qr2s2 complex Binding of two arms of the complex to immunoglobulin (2 IgG or 1 pentameric IgM) causes conformational change in C1q. This initiates a cascade of events. C1q conformational change C1r conformational change C1r conformational change C1r active enzyme C1r active enzyme C1s enzymatic cleavage C1s enzymatic cleavage C1s active enzyme C1s active enzyme C4 cleavage This result of this cascade is often referred to as the C1 esterase cleavage of C4. Cleavage of C4 is controlled by the C1 inhibitor (C1INH) The absence or mutation of C1 inhibitor leads to hereditary angioedema (swelling of the face and respiratory airways, as well as abdominal cramps). 2 IgG/1 IgM C1q C1q C1r C1r C1s C1s C4 C4b Circulating IgM is not in the right conformation for C1q binding, but antigen bound IgM is. A single molecule of IgM on a foreign RBC can activate the classical pathway, whereas some 1000 molecules of IgG on a foreign RBC are required to make sure that 2 IgG molecules are close enough to each other to initiate C1q binding. (within nm of each other). Italics = conformational change Color = enzyme activity
 causes conformational change in C1q. This initiates a cascade of events. C1q conformational change C1r conformational change. C1r conformational change C1r active enzyme. C1r active enzyme C1s enzymatic cleavage. C1s enzymatic cleavage C1s active enzyme. C1s active enzyme C4 cleavage. This result of this cascade is often referred to as the C1 esterase cleavage of C4. Cleavage of C4 is controlled by the C1 inhibitor (C1INH) The absence or mutation of C1 inhibitor leads to hereditary angioedema (swelling of the face and respiratory airways, as well as abdominal cramps). 2 IgG/1 IgM C1q C1q C1r C1r C1s C1s C4 C4b Circulating IgM is not in the right conformation for C1q binding, but antigen bound IgM is. A single molecule of IgM on a foreign RBC can activate the classical pathway, whereas some 1000 molecules of IgG on a foreign RBC are required to make sure that 2 IgG molecules are close enough to each other to initiate C1q binding. (within nm of each other). Italics = conformational change. Color = enzyme activity.")
15
Activation of C1 C1 esterase

16
Activation of C4 C1 esterase cleaves C4. C4a can act a chemoattractant
C4b has a thioester region which forms covalent bonds with molecules on the target surface. C4b can act as an opsonin and interacts with complement receptors (CR1).
.")
17
Activation of C2 C2 interacts with C4b and is cleaved by C1s, forming a C4b2a complex on the surface. C4b2a is the classical pathway’s C3 convertase. Thus, C4b2a is an enzyme that cleaves C3 to C3a and C3b. Note: There is some disagreement among scientists about the nomenclature for the cleavage products for C2. For example, some scientists identify the C3 convertase as the C4b2b complex. Generally, it is the larger fragment that has enzymatic activity. In the case of C2 cleavage products, C2a is the smallest and contributes to the enzymatic activity of the C4b2a complex.

18
C3 activation C4b2a cleaves C3, activating a labile thioester bond on C3b. This thioester can bind COVALENTLY to free hydroxyl or amino groups, resulting in C3b covalently binding to target surfaces. C3b bound to a surface acts as an opsonin. Key points for the classical pathway Activation occurs in conjunction with specific antibody C3b and C4b covalently bind to target via thioester bonds Because there is a series of enzymatic cleavage events, there is tremendous amplification of the signal as the signal progresses down the series.

19
Review of Activation of the Classical Pathway
The sequence of complement protein activation in the classical pathway is 1>4>2>3>5>6>7>8>9 Note that 4b gets “before (b 4)” its expected place. The classical pathway is triggered by antigen binding to (crosslinking) two IgG molecules or two subunit parts of one IgM molecule. The cascade of proteolytic steps in the classical pathway are performed by serine esterases. C4b and C3b bind covalently to surfaces via thioester bonds.
 its expected place. The classical pathway is triggered by antigen binding to (crosslinking) two IgG molecules or two subunit parts of one IgM molecule. The cascade of proteolytic steps in the classical pathway are performed by serine esterases. C4b and C3b bind covalently to surfaces via thioester bonds.")
20
Sequential Enzymatic Cleavage Events in Complement Activation

21
Enzymatic Cleavage Events Lectin Pathway Classical Pathway
Alternative Pathway MBL MASP-1, MASP-2 C1q C3 + H2O Factor B Factor D C1r2 C1s2 C4 C2 C3 C3 convertase (C4b2a) C3b (Opsonin) C3a C5a C5 convertase (C4b2a3b) C5b C6 C7 C8 C9 Membrane Attack Complex C5 Terminal lytic Pathway Antigen Antibody Complexes (IgG/IgM) Polysaccharides on Microbes; Also IgA Foreign surfaces (LPS); Spontaneous (Nucleophiles) Activators Complement Sensors Enzymatic Cleavage Events (Anaphylatoxins)
 C3b (Opsonin) C3a. C5a. C5 convertase (C4b2a3b) C5b C6 C7 C8 C9. Membrane Attack Complex. C5. Terminal lytic Pathway. Antigen Antibody. Complexes (IgG/IgM) Polysaccharides on. Microbes; Also IgA. Foreign surfaces (LPS); Spontaneous (Nucleophiles) Activators. Complement. Sensors. Enzymatic. Cleavage. Events. (Anaphylatoxins)")
22
Activation through C5 Involves proteolytic cleavage steps, liberating smaller fragments from C2 through C5. The smaller fragments are soluble and can have biologic effects. The larger fragments remain bound in a complex required for the next activation step. By convention, Smaller fragments are denoted by the letter ‘a’ (e.g., C3a, C5a) Larger fragments by ‘b’ (e.g., C3b, C5b) Notable exception is C2 (C2a is the larger, active fragment). Complexes with enzymatic activity are often denoted by a line over the top of the numbers or letters, as in (C4b2a)
 Larger fragments by ‘b’ (e.g., C3b, C5b) Notable exception is C2 (C2a is the larger, active fragment). Complexes with enzymatic activity are often denoted by a line over the top of the numbers or letters, as in. (C4b2a)")
23
Activation of the Mannose-Binding Pathway

24
MBL Pathway Activation of the MBL Pathway is primarily mediated by a protein constituent in the plasma called mannan-binding lectin (also called the mannose-binding lectin or MBL). Activation of the MBL Pathway does not require specific antibody for activation. Activation of the MBL Pathway occurs by a C1-independent mechanism. Activation of the MBL pathway occurs when MBL binds to specific sugar residues like N-acetyl glucosamine or mannose that are present in the cell wall polysaccharides of microorganisms such as Salmonella, Listeria, Neisseria, Candida, etc. MBL, which resembles C1q, interacts with MASP-1 and MASP-2 by a mechanism similar to C1q interaction with C1r and C1s, resulting in the formation of the classical pathway C3 convertase (C4b2a). Lectin is something that recognizes specific sequences of sugar residues. Mannose type receptor on phagocytes recognizes N acetyl glucosamine, mannose, glucose, fucose. Pathogen associated molecular patterns (on pathogen) interact with pattern recognition receptors.
. Activation of the MBL Pathway does not require specific antibody for activation. Activation of the MBL Pathway occurs by a C1-independent mechanism. Activation of the MBL pathway occurs when MBL binds to specific sugar residues like N-acetyl glucosamine or mannose that are present in the cell wall polysaccharides of microorganisms such as Salmonella, Listeria, Neisseria, Candida, etc. MBL, which resembles C1q, interacts with MASP-1 and MASP-2 by a mechanism similar to C1q interaction with C1r and C1s, resulting in the formation of the classical pathway C3 convertase (C4b2a). Lectin is something that recognizes specific sequences of sugar residues. Mannose type receptor on phagocytes recognizes N acetyl glucosamine, mannose, glucose, fucose. Pathogen associated molecular patterns (on pathogen) interact with pattern recognition receptors.")
25
Activators Lectin Pathway Classical Pathway Alternative Pathway MBL
MASP-1, MASP-2 C1q C3 + H2O Factor B Factor D C1r2 C1s2 C4 C2 C3 C3 convertase (C4b2a) C3b (Opsonin) C3a C5a C5 convertase (C4b2a3b) C5b C6 C7 C8 C9 Membrane Attack Complex C5 Terminal lytic Pathway Antigen Antibody Complexes (IgG/IgM) Polysaccharides on Microbes; Also IgA Foreign Surfaces (LPS); Spontaneous (Nucleophiles) Activators (Anaphylatoxins)
 C3b (Opsonin) C3a. C5a. C5 convertase (C4b2a3b) C5b C6 C7 C8 C9. Membrane Attack Complex. C5. Terminal lytic Pathway. Antigen Antibody. Complexes (IgG/IgM) Polysaccharides on. Microbes; Also IgA. Foreign Surfaces (LPS); Spontaneous (Nucleophiles) Activators. (Anaphylatoxins)")
26
Complement Sensors Lectin Pathway Classical Pathway
Alternative Pathway MBL MASP-1, MASP-2 C1q C3 + H2O Factor B Factor D C1r2 C1s2 C4 C2 C3 C3 convertase (C4b2a) C3b (Opsonin) C3a C5a C5 convertase (C4b2a3b) C5b C6 C7 C8 C9 Membrane Attack Complex C5 Terminal lytic Pathway Antigen Antibody Complexes (IgG/IgM) Polysaccharides on Microbes; Also IgA Foreign surfaces (LPS); Spontaneous (Nucleophiles) Activators Complement Sensors (Anaphylatoxins)
 C3b (Opsonin) C3a. C5a. C5 convertase (C4b2a3b) C5b C6 C7 C8 C9. Membrane Attack Complex. C5. Terminal lytic Pathway. Antigen Antibody. Complexes (IgG/IgM) Polysaccharides on. Microbes; Also IgA. Foreign surfaces (LPS); Spontaneous (Nucleophiles) Activators. Complement. Sensors. (Anaphylatoxins)")
27
Activation of the Alternative Pathway

28
Alternative Pathway Phylogenetically the oldest of the C3 activating pathways. Does not require specific antibody/antigen binding for activation. Can be triggered by a low level of spontaneous lysis of C3 by water to C3i that functions in a manner similar to C3b. Can be amplified by C3b binding to foreign surface structures (LPS) or by additional cleavage by bacterial proteases. Things deficient in sialic acid are good activators. An ‘activating surface’ is in large part one without adequate regulatory protein function to control alternative pathway activation, or one that is not favorable to control of the alternative pathway by factor H.
 or by additional cleavage by bacterial proteases. Things deficient in sialic acid are good activators. An ‘activating surface’ is in large part one without adequate regulatory protein function to control alternative pathway activation, or one that is not favorable to control of the alternative pathway by factor H.")
29
Some Initiators or Activators of the Alternative Pathway of Complement Activation
Many Gram negative and Gram positive bacteria LPS from Gram negative bacteria Teichoic acid from Gram positive cell walls Fungal and yeast cell walls (zymosan) Some viruses and virus infected cells Some tumor cells Some parasites Human IgA, IgG and IgE in complexes Anionic polymers (dextran sulfate) Pure carbohydrates (agarose, inulin) Targets bearing surface clusters of both charge and neutral sugar. Alternative pathway is always autoactivating and an activating surface lacks the regulators to keep it under control.
 Some viruses and virus infected cells. Some tumor cells. Some parasites. Human IgA, IgG and IgE in complexes. Anionic polymers (dextran sulfate) Pure carbohydrates (agarose, inulin) Targets bearing surface clusters of both charge and neutral sugar. Alternative pathway is always autoactivating and an activating surface lacks the regulators to keep it under control.")
30
Activators Lectin Pathway Classical Pathway Alternative Pathway MBL
MASP-1, MASP-2 C1q C3 + H2O Factor B Factor D C1r2 C1s2 C4 C2 C3 C3 convertase (C4b2a) C3b (Opsonin) C3a C5a C5 convertase (C4b2a3b) C5b C6 C7 C8 C9 Membrane Attack Complex C5 Terminal lytic Pathway Antigen Antibody Complexes (IgG/IgM) Polysaccharides on Microbes; Also IgA Foreign Surfaces (LPS); Spontaneous (Nucleophiles) Activators (Anaphylatoxins) A nucleophile is a molecule that can donate electrons. For example, Cl-, hydrogen peroxide, carboxylate anions, amines, nitrates, or NH3 (ammonia)
 C3b (Opsonin) C3a. C5a. C5 convertase (C4b2a3b) C5b C6 C7 C8 C9. Membrane Attack Complex. C5. Terminal lytic Pathway. Antigen Antibody. Complexes (IgG/IgM) Polysaccharides on. Microbes; Also IgA. Foreign Surfaces (LPS); Spontaneous (Nucleophiles) Activators. (Anaphylatoxins) A nucleophile is a molecule that can donate electrons. For example, Cl-, hydrogen peroxide, carboxylate anions, amines, nitrates, or NH3 (ammonia)")
31
Complement Sensors Lectin Pathway Classical Pathway
Alternative Pathway MBL MASP-1, MASP-2 C1q C3 + H2O Factor B Factor D C1r2 C1s2 C4 C2 C3 C3 convertase (C4b2a) C3b (Opsonin) C3a C5a C5 convertase (C4b2a3b) C5b C6 C7 C8 C9 Membrane Attack Complex C5 Terminal lytic Pathway Antigen Antibody Complexes (IgG/IgM) Polysaccharides on Microbes; Also IgA Foreign surfaces (LPS); Spontaneous (Nucleophiles) Activators Complement Sensors (Anaphylatoxins)
 C3b (Opsonin) C3a. C5a. C5 convertase (C4b2a3b) C5b C6 C7 C8 C9. Membrane Attack Complex. C5. Terminal lytic Pathway. Antigen Antibody. Complexes (IgG/IgM) Polysaccharides on. Microbes; Also IgA. Foreign surfaces (LPS); Spontaneous (Nucleophiles) Activators. Complement. Sensors. (Anaphylatoxins)")
32
Formation of the Alternative Pathway C3 Convertase (C3bBb)
C3 tickover - spontaneous conformational change of a few C3 molecules, leading to water hydrolyzing the thiolester bond of C3 to form C3 H20 or C3i. C3i is then deposited in a random and non-specific manner on the surfaces of host cells and pathogenic organisms alike. On the normal host cell, bound C3i can inactivated by binding to Factor I and Factor H. On the pathogenic organism, bound C3i can be further activated by binding to Factor B to form C3iB which is then cleaved by Factor D to form C3iBb (C3 convertase). Properdin acts to stabilize the alternative pathway C3 convertase (C3bBb) Surfaces rich in carbohydrate and deficient in sialic acid tend to be the best activators.
. Properdin acts to stabilize the alternative pathway C3 convertase (C3bBb) Surfaces rich in carbohydrate and deficient in sialic acid tend to be the best activators.")
33
Activation and Inactivation of C3b
C3 = Complement C3 FB = Factor B FD = Factor D FI = Factor I (in conjuction with Factor H, inactivates soluble C3b and C4b when deposited on the surface of a normal cell) FH = Factor H (cofactor of Factor I in mediating cleavage of C3b to its inactive form C3bi aka C3i C3 tickover is about 1% of the total C3 per hour. C3bBb is stabilized by properdin Stablized by properdin Target Cell Membrane Normal Cell Membrane
 FH = Factor H (cofactor of Factor I in mediating. cleavage of C3b to its inactive form C3bi. aka C3i. C3 tickover is about 1% of the total C3 per hour. C3bBb is stabilized by properdin. Stablized by. properdin. Target Cell Membrane. Normal Cell Membrane.")
34
Amplification of C3 Cleavage by Membrane-Bound C3bBb
Amplification – 1 C1 molecule 6 C4b2a 1200 C3b Properdin stabilizes C3bBb

35
Activation of C5 and the Terminal Complement Pathway
C5 is cleaved by either the Classical Pathway C5 convertase (C4b2aC3b) or by the Alternative Pathway C5 convertase (C3bBbC3b) into 2 fragments: C5a and C5b. Cleavage of C5 is the last enzymatic step C5b binds to a target and then interacts with C6, C7, C8 and C9 to form the Membrane Attack Complex in the lipid membrane. The Membrane Attack Complex is a transmembrane channel that allows passage of ions, compromises of the semi-permeable membrane, and causes lysis of the cell.
 or by the Alternative Pathway C5 convertase (C3bBbC3b) into 2 fragments: C5a and C5b. Cleavage of C5 is the last enzymatic step. C5b binds to a target and then interacts with C6, C7, C8 and C9 to form the Membrane Attack Complex in the lipid membrane. The Membrane Attack Complex is a transmembrane channel that allows passage of ions, compromises of the semi-permeable membrane, and causes lysis of the cell.")
36
Activation of C5 C5 is cleaved into 2 fragments (C5a and C5b) by either The Alternative Pathway C5 convertase (C3bBbC3b) or The Classical Pathway C5 convertase (C4b2aC3b). Cleavage of C5 is the last enzymatic step.
. Cleavage of C5 is the last enzymatic step.")
37
Non-Cleavage Events Involved in MAC Assembly Lectin Pathway
Classical Pathway Alternative Pathway MBL MASP-1, MASP-2 C1q C3 + H2O Factor B Factor D C1r2 C1s2 C4 C2 C3 C3 convertase (C4b2a) C3b (Opsonin) C3a C5a C5 convertase (C4b2a3b) C5b C6 C7 C8 C9 Membrane Attack Complex C5 Terminal lytic Pathway Antigen Antibody Complexes (IgG/IgM) Polysaccharides on Microbes; Also IgA Foreign surfaces (LPS); Spontaneous (Nucleophiles) Activators Complement Sensors (Anaphylatoxins) Non-Cleavage Events Involved in MAC Assembly
 C3b (Opsonin) C3a. C5a. C5 convertase (C4b2a3b) C5b C6 C7 C8 C9. Membrane Attack Complex. C5. Terminal lytic Pathway. Antigen Antibody. Complexes (IgG/IgM) Polysaccharides on. Microbes; Also IgA. Foreign surfaces (LPS); Spontaneous (Nucleophiles) Activators. Complement. Sensors. (Anaphylatoxins) Non-Cleavage. Events Involved in. MAC Assembly.")
38
Non-Cleavage Events in Assembly of the Membrane Attack Complex
C5b then interacts with C6, C7, and C8. Lysis can occur in the absence of binding of C9 but it is slower.

39
Punches Hole in Bacterial or Viral Membrane
Lectin Pathway Classical Pathway Alternative Pathway MBL MASP-1, MASP-2 C1q C3 + H2O Factor B Factor D C1r2 C1s2 C4 C2 C3 C3 convertase (C4b2a) C3b (Opsonin) C3a C5a C5 convertase (C4b2a3b) C5b C6 C7 C8 C9 Membrane Attack Complex C5 Terminal lytic Pathway Antigen Antibody Complexes (IgG/IgM) Polysaccharides on Microbes; Also IgA Foreign surfaces (LPS); Spontaneous (Nucleophiles) Activators Complement Sensors (Anaphylatoxins) Punches Hole in Bacterial or Viral Membrane
 C3b (Opsonin) C3a. C5a. C5 convertase (C4b2a3b) C5b C6 C7 C8 C9. Membrane Attack Complex. C5. Terminal lytic Pathway. Antigen Antibody. Complexes (IgG/IgM) Polysaccharides on. Microbes; Also IgA. Foreign surfaces (LPS); Spontaneous (Nucleophiles) Activators. Complement. Sensors. (Anaphylatoxins) Punches Hole in Bacterial. or Viral Membrane.")
40
Assembly of C9 Channel If C9 molecules are bound to the C5bC6C7C8 complex, they form the Membrane Attack Complex that can punch a hole in the lipid membrane. Since the Membrane Attack Complex is a transmembrane channel that allows passage of ions, it will compromise the semi-permeability of the membrane and result in lysis of the cell.

41
Notes on C9 Assembly If the interaction with C5b through C9 occurs in proximity to a membrane, then the MAC assembly occurs in that membrane and lysis is the end result. Alternatively, C5b-9 can bind to S protein in the fluid phase. In this case, lysis does not occur.

42
Summary of Pathways of Activation
Three Primary Pathways of Activation with different start signals Classical – antigen antibody Mannose binding lectin - mannose Alternative – LPS, carbohydrates, etc Proteolytic cleavages of complement components operate through C5 Non-proteolytic events for assembly of C6789 membrane attack complex

43
Summary of Names You Need to Know
Classical Pathway: C1q, C1r, C1s, C4, C2 Mannose Binding lectin pathway: MBL (mannose binding lectin) MASP-1 (MBL-associated serine protease) MASP-2 Alternative Pathway: Factor B Factor D Properdin Common to all pathways: C3 Terminal Lytic pathway: C5, C6, C7, C8, C9
 MASP-1 (MBL-associated serine protease) MASP-2. Alternative Pathway: Factor B. Factor D. Properdin. Common to all pathways: C3. Terminal Lytic pathway: C5, C6, C7, C8, C9.")
44
Control What stops the activation? Or Why don’t we lyse all of our own cells?

45
Things That Limit Complement Activation
Short half life of the enzymes formed Properties of non-activator surfaces Inhibitors Fluid phase inhibitors So active fragments don’t go too far Membrane bound inhibitors On our own membranes So C3b and C4b don’t attach or don’t lead to lysis of our own cells

46
Activation and Inactivation of C3b
C3 = Complement C3 FB = Factor B FD = Factor D FI = Factor I ( inconjuction with Factor H, inactivates soluble C3b and C4b when deposited on the surface of a normal cell) FH = Factor H (cofactor of Factor I in mediating cleavage of C3b to its inactive form C3bi aka C3i C3 tickover is about 1% of the total C3 per hour. C3bBb is stabilized by properdin Stablized by properdin Target Cell Membrane Normal Cell Membrane
 FH = Factor H (cofactor of Factor I in mediating. cleavage of C3b to its inactive form C3bi. aka C3i. C3 tickover is about 1% of the total C3 per hour. C3bBb is stabilized by properdin. Stablized by. properdin. Target Cell Membrane. Normal Cell Membrane.")
49
What If You Lack Control?
Deficiencies of complement control proteins can lead to uncontrolled activation of the complement system Consequences of activation – lysis, etc Consumption (exhaustion) of the complement components leading to the consequences of secondary complement deficiency (immune-complex disease and infections)
 of the complement components leading to the consequences of secondary complement deficiency (immune-complex disease and infections)")
50
C1 Inhibitor Deficiency
Roles of the C1 inhibitor Inhibits C1 esterase Also inhibits kallikrein, plasmin, Factor XIa and Factor XIIa Deficiency in C1 inhibitor leads to recurrent episodes of localized edema in skin, GI tract, or larynx Results in HAE (hereditary angioedema) Prevalence: 2-10 per 100,000 First case of homozygous C1 inhibitor deficiency reported in 2006 (JACI 118:1330, 2006) Homozygous patients had undetectable C1q, reduced C1s, circulating active C1r, and a C1Inh mostly in its cleaved inactive form. The most common HAE treatment is attenuated androgens, which increase the C1INH gene transcription levels. C1INH is a serpin plasma serine protease inhibitor. Also inhibits MASP
 Prevalence: 2-10 per 100,000. First case of homozygous C1 inhibitor deficiency reported in 2006 (JACI 118:1330, 2006) Homozygous patients had undetectable C1q, reduced C1s, circulating active C1r, and a C1Inh mostly in its cleaved inactive form. The most common HAE treatment is attenuated androgens, which increase the C1INH gene transcription levels. C1INH is a serpin plasma serine protease inhibitor. Also inhibits MASP.")
51
Hereditary angioedema
Figure 3-6. Hereditary angioneurotic edema (HAE). A and B, Angioedema of the hands. C, Five-year-old girl with a moderate attack of angioedema. D, Small bowel barium radiograph during an acute episode of pain in the proband. Two segments of jejunum have mural edema: "thumbprinting" (thick arrows) and spiculation (thin arrows). This condition is one of several that are caused by deficiencies and dysfunction on complement regulator proteins. HAE is an autosomal dominant condition caused by a deficiency or nonfunction of C1 esterase inhibitor []. Patients with this abnormality have recurrent episodes of swelling of the soft tissues, primarily of the face, extremities, larynx, and intestinal mucosa. Symptoms usually begin in adolescence, and attacks are commonly triggered by emotional stress and trauma (see panels A-D). Without the C1 esterase inhibitor, there is continued activation of the classic complement pathway and dysregulation of the activity of clotting, kinin, and fibrinolysis pathways. The causative factor leading to the angioedema may be C3a, C4a, and C5a; the anaphylotoxins; or C2 kinin from kinin activity. C4 levels are decreased in patients with HAE. Aminocaproic acid is used in the treatment of patients with acute attacks and for prevention before a medical procedure such as surgery. For long-term therapy, androgens such as danazol have been shown to stimulate C1 esterase inhibitor production. (Panels A and B from Arreaza et al. [], with permission; panel C from Weinstock et al. [], with permission; panel D from Nielsen et al. []; with permission.)
. A and B, Angioedema of the hands. C, Five-year-old girl with a moderate attack of angioedema. D, Small bowel barium radiograph during an acute episode of pain in the proband. Two segments of jejunum have mural edema: thumbprinting (thick arrows) and spiculation (thin arrows). This condition is one of several that are caused by deficiencies and dysfunction on complement regulator proteins. HAE is an autosomal dominant condition caused by a deficiency or nonfunction of C1 esterase inhibitor []. Patients with this abnormality have recurrent episodes of swelling of the soft tissues, primarily of the face, extremities, larynx, and intestinal mucosa. Symptoms usually begin in adolescence, and attacks are commonly triggered by emotional stress and trauma (see panels A-D). Without the C1 esterase inhibitor, there is continued activation of the classic complement pathway and dysregulation of the activity of clotting, kinin, and fibrinolysis pathways. The causative factor leading to the angioedema may be C3a, C4a, and C5a; the anaphylotoxins; or C2 kinin from kinin activity. C4 levels are decreased in patients with HAE. Aminocaproic acid is used in the treatment of patients with acute attacks and for prevention before a medical procedure such as surgery. For long-term therapy, androgens such as danazol have been shown to stimulate C1 esterase inhibitor production. (Panels A and B from Arreaza et al. [], with permission; panel C from Weinstock et al. [], with permission; panel D from Nielsen et al. []; with permission.)")
52
Deficiency in Decay Accelerating Factor (CD55) & CD59
DAF deficiency causes increased susceptibility of erythrocytes to membrane attack complex-mediated lysis See as complement-mediated intravascular hemolysis in paroxysmal nocturnal hemoglobinuria (PNH) DAF deficiency is due to a defect in a post-translational modification of the peptide anchors that bind the proteins to the cell membrane Recent studies suggest that DAF deficiency can be treated with an antibody to C5 reduces hemolysis
 DAF deficiency is due to a defect in a post-translational modification of the peptide anchors that bind the proteins to the cell membrane. Recent studies suggest that DAF deficiency can be treated with an antibody to C5 reduces hemolysis.")
53
What If You Lack a Complement Protein?

54
Review: What does complement do?
Lyses cells (MAC) Inflammatory mediators (C3a, C5a) Opsonization Solubilization and clearance of immune complexes Augmentation of humoral immunity
 Inflammatory mediators (C3a, C5a) Opsonization. Solubilization and clearance of immune complexes. Augmentation of humoral immunity.")
55
Review: What does complement do?
Lyses cells (MAC) Inflammatory mediators (C3a, C5a) Opsonization Solubilization and clearance of immune complexes Augmentation of humoral immunity
 Inflammatory mediators (C3a, C5a) Opsonization. Solubilization and clearance of immune complexes. Augmentation of humoral immunity.")
56
Anaphylatoxins C3a C3a receptor Response
C3a and C5a can mimic the symptoms of inflammation and anaphylaxis Chemotaxis, smooth muscle contraction, increased vascular permeability, degranulation of mast cells, etc. Distinct receptors on many cell types

57
Anaphylatoxin Receptors
CD88

58
Review: What does complement do?
Lyses cells (MAC) Inflammatory mediators (C3a, C5a) Opsonization Solubilization and clearance of immune complexes Augmentation of humoral immunity
 Inflammatory mediators (C3a, C5a) Opsonization. Solubilization and clearance of immune complexes. Augmentation of humoral immunity.")
59
Things C4b and C3b can do Complement Activation C4b and/or C3b
on surfaces Participate in continued pathway activation leading to MAC Degraded to fragments Interact with CR2 and CR3 Interact with CR1 Lysis Opsonization Clearance of IC Augmentation of humoral immunity Opsonization Clearance of IC

60
CR1 (CD35) Major ligands C3b, C4b
Monocytes, macrophages, PMN, Eosinophil, RBC, B and T cells Transport of immune complexes by RBC Promotes immune adherence (binding of opsonized microbes to primate RBCs) Promotes phagocytosis in cooperation with Fc receptors Blocks formation of C3 convertase
 Promotes phagocytosis in cooperation with Fc receptors. Blocks formation of C3 convertase.")
61
Complement Receptors

62
Review: What does complement do?
Lyses cells (MAC) Inflammatory mediators (C3a, C5a) Opsonization Solubilization and clearance of immune complexes Augmentation of humoral immunity
 Inflammatory mediators (C3a, C5a) Opsonization. Solubilization and clearance of immune complexes. Augmentation of humoral immunity.")
63
C3 fragment interaction with Complement Receptors
Bacteria or IC Clearance of Immune Complex Augments humoral immunity

64
Immune Complex Disease
High incidence of Immune Complex disease in individuals who are deficient in C1, C4, C2 or C3 Immune complexes are not solubilized and cleared Complement can also play a significant role in tissue damage in Immune Complex diseases such as SLE (systemic lupus erythematosus) Excess immune complexes cause pathological complement activation inflammation, tissue damage
 Excess immune complexes cause pathological complement activation inflammation, tissue damage.")
65
Immune Complex Solubilization And Transport
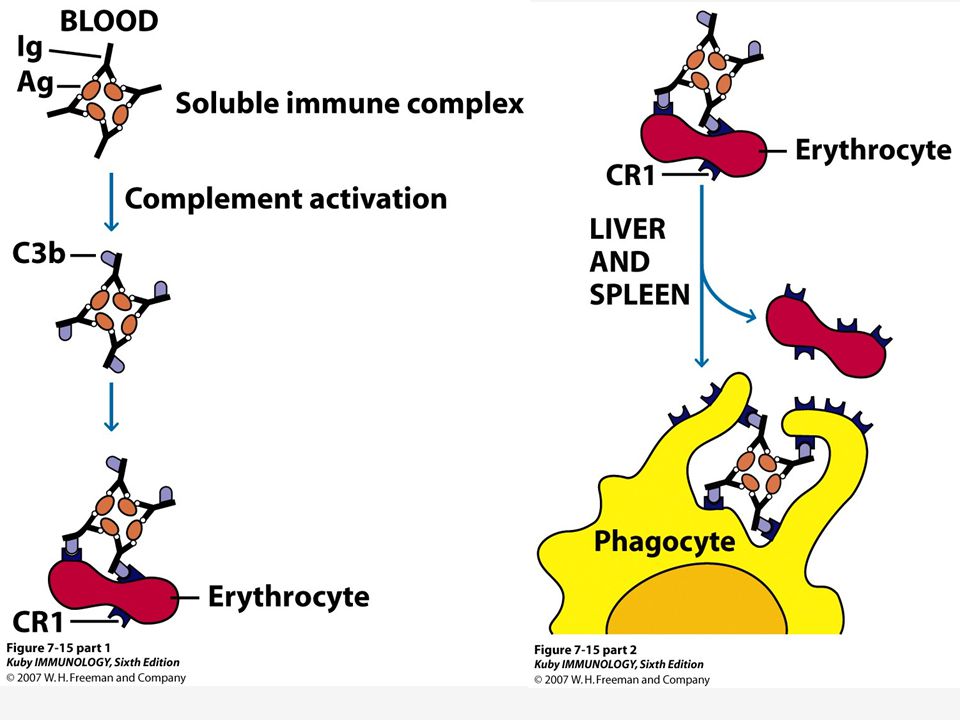
Complement prevents formation of insoluble immune complexes (solubilization). Deposition of insoluble aggregates in the tissues can cause damage and immune complex disease. Binding of C3b to the antigen antibody complex interferes with lattice formation, limits its growth, prevents precipitation of the antigen antibody complexes and keeps them soluble.
. Deposition of insoluble aggregates in the tissues can cause damage and immune complex disease. Binding of C3b to the antigen antibody complex interferes with lattice formation, limits its growth, prevents precipitation of the antigen antibody complexes and keeps them soluble.")
66
Immune complex transport
The complement system is a major mechanism for removal of immune complexes (transport). Immune complexes coated with C3b bind to CR1. More than 85% of the CR1 in the circulation is on the RBC. CR1 receptors on the erythrocyte are responsible for the transport of immune complexes to the reticuloendothelial system for clearance (macrophages in spleen, etc). The immune complex coated with C3b is transferred from the RBC CR1 receptor to the macrophage CR1 receptor. The immune complex is then internalized and degraded.
. Immune complexes coated with C3b bind to CR1. More than 85% of the CR1 in the circulation is on the RBC. CR1 receptors on the erythrocyte are responsible for the transport of immune complexes to the reticuloendothelial system for clearance (macrophages in spleen, etc). The immune complex coated with C3b is transferred from the RBC CR1 receptor to the macrophage CR1 receptor. The immune complex is then internalized and degraded.")
68
Review: What does complement do?
Lyses cells (MAC) Inflammatory mediators (C3a, C5a) Opsonization Solubilization and clearance of immune complexes Augmentation of humoral immunity
 Inflammatory mediators (C3a, C5a) Opsonization. Solubilization and clearance of immune complexes. Augmentation of humoral immunity.")
69
CR2 (CD21) Major ligands C3d, C3dg, iC3b
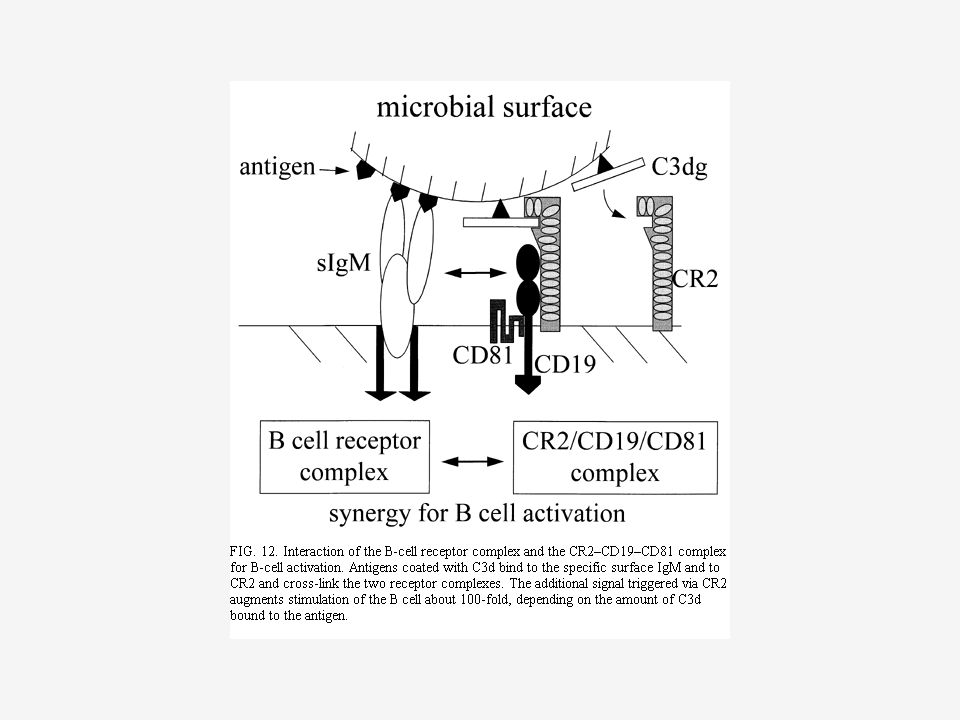
B cells, activated T cells, epithelial cells CR2 forms an additional signal with antibody to augment stimulation of the B cell to increase the humoral immune response (CR2/CD19/CD81). CR2 has high affinity for an envelope protein of Epstein Barr virus, allowing the virus to enter the B cell.
. CR2 has high affinity for an envelope protein of Epstein Barr virus, allowing the virus to enter the B cell.")
71
Complement Deficiencies
Deficiencies of the various complement components often present as infections Pyogenic infections and infections with encapsulated bacteria (classical and alternative) Opsonization and phagocytosis are a primary host defense. Neisseria infections (C3, alternative pathway and terminal lytic pathway) Immune complex or autoimmune disease Classical pathway or C3 deficiencies MBL deficiency results in serious pyogenic infections as well
 Opsonization and phagocytosis are a primary host defense. Neisseria infections (C3, alternative pathway and terminal lytic pathway) Immune complex or autoimmune disease. Classical pathway or C3 deficiencies. MBL deficiency results in serious pyogenic infections as well.")
72
Complement Deficiencies and Associated Diseases
Recurrent infection by pyogenic (pus forming) bacteria such as steptococci and staphylococci. These organisms are gram positive and generally resistant to the lytic effects of the MAC. Nevertheless, the early complement components ordinarily prevent recurrent infection by mediating a localized inflammatory response and opsonizing the bacteria. Wikipedia, 2011 A pyogenic infection is an infection that is characterized by severe local inflammation, usually with pus formation, generally caused by one of the pyogenic bacteria.[1] Some common disease processes caused by pyogenic infections are impetigo, osteomyelitis, septic arthritis, and necrotizing fasciitis.[citation needed][2] [edit] Pyogenic bacteria A great many species of bacteria may be pyogenic. The most commonly found include:[3] Staphylococcus aureus Staphylococcus epidermidis Streptococcus pyogenes Escherichia coli (Bacillus coli communis) Streptococcus pneumoniae (Fraenkel's pneumococcus) Klebsiella pneumoniae (Friedländer's bacillus) Salmonella typhi (Bacillus typhosus) Pseudomonas aeruginosa Neisseria gonorrhoeae Actinomyces Burkholderia mallei (Glanders bacillus) Mycobacterium tuberculosis (tubercle bacillus) From Wikipedia, the free encyclopedia Jump to: navigation, search SEM micrograph of an encapsulated bacterium (Pneumococcus). Polysaccharide encapsulated bacteria, frequently referred to simply as encapsulated bacteria and less precisely called encapsulated organisms, are a group of bacteria that have an outer covering, a bacterial capsule, made of polysaccharide. Contents [hide] 1 Examples of encapsulated bacteria 2 Role in disease 2.1 Asplenia 2.2 Children 3 See also 4 References [edit] Examples of encapsulated bacteria Haemophilus influenzae type b (Hib)[1] Streptococcus pneumoniae (pneumococcus)[1] Neisseria meningitides (meningococcus)[1] Group B streptococcus (GBS)[1] Klebsiella pneumoniae Salmonella typhi[2]
 bacteria such as steptococci and staphylococci. These organisms are gram positive and generally resistant to the lytic effects of the MAC. Nevertheless, the early complement components ordinarily prevent recurrent infection by mediating a localized inflammatory response and opsonizing the bacteria. Wikipedia, A pyogenic infection is an infection that is characterized by severe local inflammation, usually with pus formation, generally caused by one of the pyogenic bacteria.[1] Some common disease processes caused by pyogenic infections are impetigo, osteomyelitis, septic arthritis, and necrotizing fasciitis.[citation needed][2] [edit] Pyogenic bacteria. A great many species of bacteria may be pyogenic. The most commonly found include:[3] Staphylococcus aureus. Staphylococcus epidermidis. Streptococcus pyogenes. Escherichia coli (Bacillus coli communis) Streptococcus pneumoniae (Fraenkel s pneumococcus) Klebsiella pneumoniae (Friedländer s bacillus) Salmonella typhi (Bacillus typhosus) Pseudomonas aeruginosa. Neisseria gonorrhoeae. Actinomyces. Burkholderia mallei (Glanders bacillus) Mycobacterium tuberculosis (tubercle bacillus) From Wikipedia, the free encyclopedia. Jump to: navigation, search. SEM micrograph of an encapsulated bacterium (Pneumococcus). Polysaccharide encapsulated bacteria, frequently referred to simply as encapsulated bacteria and less precisely called encapsulated organisms, are a group of bacteria that have an outer covering, a bacterial capsule, made of polysaccharide. Contents. [hide] 1 Examples of encapsulated bacteria. 2 Role in disease. 2.1 Asplenia. 2.2 Children. 3 See also. 4 References. [edit] Examples of encapsulated bacteria. Haemophilus influenzae type b (Hib)[1] Streptococcus pneumoniae (pneumococcus)[1] Neisseria meningitides (meningococcus)[1] Group B streptococcus (GBS)[1] Klebsiella pneumoniae. Salmonella typhi[2]")
75
Factor H is One Fluid Phase Inhibitor of C3 Convertase
Factor H is a fluid phase inhibitor of C3 convertase. If it sees C3bBb floating around, it binds and dissociates the Bb, thus inactivating the C3bBb. ‘Decay acceleration of the convertase’

76
Factor H Can Inactivate C3bBb on the Surface of a Normal Cell
If Factor H sees C3bBb on a membrane with sialic acid (like our membranes), it will bind to the sialic acid residue and C3b, displacing Bb from the convertase and inactivating C3bBb. Factor I than can degrade the C3b, with Factor H as a cofactor. An activator surface (such as bacteria) does not have sialic acid and therefore Factor H cannot bind and displace the Bb. In this case, the Factor H does not inhibit the C3 convertase activity.
, it will bind to the sialic acid residue and C3b, displacing Bb from the convertase and inactivating C3bBb. Factor I than can degrade the C3b, with Factor H as a cofactor. An activator surface (such as bacteria) does not have sialic acid and therefore Factor H cannot bind and displace the Bb. In this case, the Factor H does not inhibit the C3 convertase activity.")
Similar presentations








 Activation pathways Effector functions Regulation of complement activation.>")
BB Fall 2007.>")






BB Unit 1 Nature of the Immune System Part 9 Complement.>")




 Harvianto Siman Santosa ( )>")

