Download presentation
Presentation is loading. Please wait.

1
How to Manage High Risk Myeloma Dr Matthew Jenner Consultant Haematologist Southampton General Hospital UK Myeloma Forum Autumn Day 12 November 2014

2
Introduction

3
Why define high risk myeloma? 3 Patient expectations o Outcomes vary widely between different patients o Myeloma very heterogenous disease Aim for a risk stratified approach – one size may not fit all o Maximise treatment for those that need it o Minimise treatment and toxicities for those who may not o Acute leukaemia and lymphoma models Better define high risk disease o Subgroup analysis may lead to identification of common clinical and biological features leading to more individualised treatments

4
Variables that impact prognosis in any malignancy including myeloma Patient factors o Age o Performance status (activity levels) o Co-morbidities o Medication o Kidney function Tumour stage o in myeloma, markers of disease bulk o ISS based on albumin and beta 2 microglobulin Tumour biology o Isotype o Extramedullary myeloma and plasma cell leukaemia o Genetic lesions detected by cytogenetics, gene expression or mutation analysis o Response to treatment
 o Co-morbidities o Medication o Kidney function Tumour stage o in myeloma, markers of disease bulk o ISS based on albumin and beta 2 microglobulin Tumour biology o Isotype o Extramedullary myeloma and plasma cell leukaemia o Genetic lesions detected by cytogenetics, gene expression or mutation analysis o Response to treatment")
5
High risk myeloma Defining high risk myeloma Individual drug therapies Autologous transplantation Clinical trials and future strategies

6
Smouldering myeloma

7
Classifiers of high risk status 7 Degree of bone marrow infiltration o IMWG criteria Imaging o PET-CT o Whole body CT o Whole body DW MRI Immunophenotyping o Aberrant vs normal plasma cells ?Cytogenetics

8
Smouldering myeloma Role of high risk cytogenetics 8 Data for cytogenetics in symptomatic myeloma is clear cut Adverse IgH translocations and copy number abnormalities well recognised o t(4;14), t(14;16), t(14;20), del1p, del17p, gain 1q Same abnormalities found in MGUS and smouldering myeloma Case series of stable MGUS and SMM with apparent high risk abnormalities IgH translocations initiating events Copy number abnormalities ?progression events
, t(14;16), t(14;20), del1p, del17p, gain 1q Same abnormalities found in MGUS and smouldering myeloma Case series of stable MGUS and SMM with apparent high risk abnormalities IgH translocations initiating events Copy number abnormalities progression events")
9
MGUS and smouldering myeloma cytogenetics: Wessex myeloma database IgH translocations 9 Different patterns of progression from MGUS and SMM to myeloma t(14;20) stable disease MGUS o t(4;14) 1/5 progressed and t(14;16) 2/6 progressed at median f/u of 17-120 months from diagnosis of MGUS SMM o t(4;14) 12/19 progressed and t(14;16) 2//4 progressed at median f/u of 33 to 78months from diagnosis of SMM o Evolving and non-evolving pattern of progression MGUSSMMMM t(4;14)6/193 (3%)19/148 (13%)198/1830 (11%) t(14;16)6/193 (3%)4/148 (3%)55/1830 (3%) t(14;20)9/192 (5%)1/149 (<1%)27/1830 (1.5%) FM Ross, L Chiecchio et al, Haematologica 2010
 stable disease MGUS o t(4;14) 1/5 progressed and t(14;16) 2/6 progressed at median f/u of months from diagnosis of MGUS SMM o t(4;14) 12/19 progressed and t(14;16) 2//4 progressed at median f/u of 33 to 78months from diagnosis of SMM o Evolving and non-evolving pattern of progression MGUSSMMMM t(4;14)6/193 (3%)19/148 (13%)198/1830 (11%) t(14;16)6/193 (3%)4/148 (3%)55/1830 (3%) t(14;20)9/192 (5%)1/149 (<1%)27/1830 (1.5%) FM Ross, L Chiecchio et al, Haematologica 2010")
10
Smouldering myeloma 10 No evidence to recommend treatment based on HR cytogenetics alone Use standard CRAB criteria for commencing treatment +/- novel imaging Close monitoring including imaging Rationale: o Potential role for homeostasis between sub clones Need for further studies to evaluate in face of new agents o Require OS as well as PFS data

11
Case 1

12
60 year old female 12 1996 o Right breast carcinoma treated with WLE and RT 2005 o DCIS left breast with bilateral mastectomies and Arimidex o No evidence of relapse on follow-up May 2013 o Generalised bone pain, weight loss o IgG kappa paraprotein 15g/L o Free KLC 551 mg/L o BMA: 15% PC o FISH: t(14;16), del17p, del1p, gain 1q o ISS 2 o SS: lytic lesions skull, humeri, collapse L2 and T12 July 2013 o Local RT L2 8Gy single fraction o Myeloma XI: CTD
, del17p, del1p, gain 1q o ISS 2 o SS: lytic lesions skull, humeri, collapse L2 and T12 July 2013 o Local RT L2 8Gy single fraction o Myeloma XI: CTD")
13
Case 1 13 CTD x6 achieving VGPR: o paraprotein 0.7 g/L o FKLC 140 mg/L BM: MRD positive 0.1% abnormal PC HDM(200) ASCT 9/12/13 D100 11/3/14 o Paraprotein 1.6 g/L o FKLC 127 mg/L o BM: no excess PC o MRD pos 0.1% abnormal PC April 2014 Randomised to lenalidomide and vorinostat maintenance June 2014 progressive flank pain: o Renal tract USS neg o July 2014 PET-CT
 ASCT 9/12/13 D100 11/3/14 o Paraprotein 1.6 g/L o FKLC 127 mg/L o BM: no excess PC o MRD pos 0.1% abnormal PC April 2014 Randomised to lenalidomide and vorinostat maintenance June 2014 progressive flank pain: o Renal tract USS neg o July 2014 PET-CT")
14
Case 1 PET-CT

15
Case 1 July 2014 15 PET-CT o Widespread FDG avid lesions multiple vertebrae, sternum, ribs, pelvis o Left paravertebral mass MRI o T7 to T11/12 soft tissue mass with early cord compromise Bone marrow approx 10% PC Paraprotein 3.5 g/L Free kappa light chains 77 mg/L Treatment: o RT to paraspinal mass o VRD-PACE o VRD o VRD-PACE Awaiting follow-up imaging

16
Case 1 Observations 16 Cytogenetically defined high risk myeloma (HRMM) Role of individual drugs cannot be ascertained from single case Achieved VGPR. MRD positive. Commenced maintenance at approx 4 months post ASCT Extramedullary relapse Questions: o How important is depth of response in cytogenetically defined HRMM? o Does high dose mephalan improve outcome or promote progression? o What is the role of consolidation and maintenance and when should it start? o Does recovery period post ASCT enable myeloma plasma cell recovery? o What is more important dose intensity or dose density? o What is the role of imaging?

17
Genomic landscape of high risk myeloma

18
Initiation and progression of myeloma Morgan, Walker & Davies, Nature Reviews Cancer 2012

19
Clonal dynamics in a patient with high-risk MM. The summarized results of 8 different FISH assays are shown to indicate the relative abundance of each clone defined by aCGH at the 5 time points studied. Keats J J et al. Blood 2012;120:1067-1076 ©2012 by American Society of Hematology

20
HRMM: Thalidomide

21
MRC Myeloma IX - Trial Design Intensive Clodronate CVAD Zoledronic acid CVAD Clodronate C-TD Zoledronic acid C-TD MEL-200 ASCT –Thal+Thal Non-intensive Clodronate MP Zoledronic acid MP Clodronate C-TDa Zoledronic acid C-TDa Max Response –Thal+Thal Primary endpoints: PFS, OS, ORR Secondary endpoints: Time to first SRE, SRE incidence, Safety, and QoL Zoledronic acid (4 mg IV q 3-4 wk); Clodronate (1,600 mg/d PO) ISRCTN68454111 N = 1,960 RANDOMISATION Treatment continued until disease progression 21
; Clodronate (1,600 mg/d PO) ISRCTN N = 1,960 RANDOMISATION Treatment continued until disease progression 21")
22
12243648 60 0 Favourable iFISH Adverse iFISH 012 24364860 OS (months) 0 20 40 60 80 100 Patients (%) 88 93 81 77 53 44 32 16 10 5 CTDa MP 72 88 93 OS (months) 0 20 40 60 80 100 Patients (%) 60 55 43 44 23 17 8888 3636 CTDa MP 60 55 CTDa MP P <.001 Myeloma IX: Landmark analysis in patients with favourable and adverse iFISH In patients with favourable FISH there was a strong OS advantage for CTDa compared to MP. This effect was not seen in patients with adverse cytogenetics: t(4;14), t(14:16), +1q, del(17p) CTDa MP P =.41 AB GJ Morgan, FE Davies et al, Blood 2011
, t(14:16), +1q, del(17p) CTDa MP P =.41 AB GJ Morgan, FE Davies et al, Blood")
23
Survival according to thalidomide maintenance therapy regimen (ITT population): (A) PFS; and (B) OS; (C) OS in patients with favorable iFISH profiles; (D) OS in patients with adverse iFISH profiles. Morgan G J et al. Clin Cancer Res 2013;19:6030-6038 ©2013 by American Association for Cancer Research

24
HRMM: bortezomib

25
Diagram of patient disposition and patient flow through protocol. Harousseau J et al. JCO 2010;28:4621-4629 ©2010 by American Society of Clinical Oncology IFM 2005-01 Bortezomib-Dex vs. Vincristine- Adriamicin-Dex (VAD) Newly diagnosed myeloma suitable for intensive chemotherapy and ASCT A: VADB: Vel Dex
 Newly diagnosed myeloma suitable for intensive chemotherapy and ASCT A: VADB: Vel Dex.")
26
IFM 2005-01: (A) Event-free survival (EFS) and (B) overall survival (OS) in patients with t(4;14) treated with bortezomib-dexamethasone (Vel/Dex) induction (n = 106) or vincristine, doxorubicin, and dexamethasone (VAD) induction (n = 98; EFS and OS in years; P <.001 for EFS and OS Avet-Loiseau H et al. JCO 2010;28:4630-4634 ©2010 by American Society of Clinical Oncology

27
CONSORT diagram of 827 adult patients with multiple myeloma (MM) in the Dutch-Belgian Hemato-Oncology Group 65/German Multicenter Myeloma Group HD4 (HOVON-65/GMMG-HD4) Sonneveld P et al. JCO 2012;30:2946-2955 ©2012 by American Society of Clinical Oncology A: VAD- thalidomide B: PAD- bortezomib

28
Phase III Trial of PAD and bortezomib maintenance vs. VAD and thalidomide in Myeloma: Survival Survival OutcomeHR95% CIP Value PFS Overall From last HDM 0.79 0.82 0.66-0.95 0.66-1.02.01.08 OS 0.730.56-0.96.02 Sonneveld P, et al. ASH 2010. Abstract 40. 0 25 50 75 100 Cumulative % Progression Free 012243648 VAD PAD 373 371 n 243 215 F VAD PAD Mos HR: 0.79 (95% CI: 0.66-0.95; P =.01) HOVON
 HOVON.")
29
Kaplan-Meier survival curves of progression-free survival (PFS) and overall survival (OS) according to treatment arm within subgroups according to del(17p). Sonneveld P et al. JCO 2012;30:2946-2955 ©2012 by American Society of Clinical Oncology Arm A VAD/thal Arm B PAD/bort Bortezomib appears to overcome adverse effect of del(17p) Perhaps related to adverse impact of thalidomide on del(17p) myeloma?
 Perhaps related to adverse impact of thalidomide on del(17p) myeloma .")
30
(A)Kaplan-Meier distribution curve (intent-to-treat analysis) for the key efficacy end point of progression-free survival. (B)Forest plot of hazard ratios for progression-free survival, for the individual studies and the integrated analysis Sonneveld P et al. JCO 2013;31:3279-3287 ©2013 by American Society of Clinical Oncology Bortezomib-Based Versus Nonbortezomib-Based Induction Treatment Before Autologous Stem-Cell Transplantation in Patients With Previously Untreated Multiple Myeloma: A Meta-Analysis of Phase III Randomized, Controlled Trials
Forest plot of hazard ratios for progression-free survival, for the individual studies and the integrated analysis Sonneveld P et al. JCO 2013;31: ©2013 by American Society of Clinical Oncology Bortezomib-Based Versus Nonbortezomib-Based Induction Treatment Before Autologous Stem-Cell Transplantation in Patients With Previously Untreated Multiple Myeloma: A Meta-Analysis of Phase III Randomized, Controlled Trials.")
31
HRMM: Total therapy

32
Total Therapy 3 Developed at MIRT, Arkansas Multidrug sequential treatment (V-DT-PACE) Intensive chemotherapy Tandem autologous transplantation Consolidation Maintenance High risk myeloma defined by gene expression profiling TT2 no bortezomib TT3 with bortezomib 32
 Intensive chemotherapy Tandem autologous transplantation Consolidation Maintenance High risk myeloma defined by gene expression profiling TT2 no bortezomib TT3 with bortezomib 32")
33
TP53 deletion is not an adverse feature in multiple myeloma treated with total therapy 3 British Journal of Haematology Volume 147, Issue 3, pages 347-351, 21 AUG 2009 DOI: 10.1111/j.1365-2141.2009.07864.x http://onlinelibrary.wiley.com/doi/10.1111/j.1365-2141.2009.07864.x/full#f1 Volume 147, Issue 3, http://onlinelibrary.wiley.com/doi/10.1111/j.1365-2141.2009.07864.x/full#f1 OSEFS GEP low risk GEP high risk

34
Identification of novel agents that improve the survival of patients with high-risk MM. xy plot of percent OS for the 2 arms of randomized controlled clinical trials for patients with different genetic lesions. Bergsagel P L et al. Blood 2013;121:884-892 ©2013 by American Society of Hematology

35
HRMM: Novel agent combinations

36
VRD consolidation Nooka et al Leukaemia 2014 36 High-risk myeloma defined by o the presence of deletion of p53 (locus 17p13) o deletion of 1p o (t(4;14) or t(14;16) by fluorescence in situ hybridization or by metaphase cytogenetics o presentation as PCL (20% circulating plasma cells in peripheral blood) 45 patients Induction not specified, majority VTD or VRD ASCT Maintenance therapy o lenalidomide (10 mg/day orally) on days 1–21 of a 28-day cycle o bortezomib (1.3 mg/m 2 per week subcutaneously/intravenously) o low-dose dexamethasone (40 mg per week orally) o for up to 3 years, followed by single-agent lenalidomide maintenance thereafter
 o deletion of 1p o (t(4;14) or t(14;16) by fluorescence in situ hybridization or by metaphase cytogenetics o presentation as PCL (20% circulating plasma cells in peripheral blood) 45 patients Induction not specified, majority VTD or VRD ASCT Maintenance therapy o lenalidomide (10 mg/day orally) on days 1–21 of a 28-day cycle o bortezomib (1.3 mg/m 2 per week subcutaneously/intravenously) o low-dose dexamethasone (40 mg per week orally) o for up to 3 years, followed by single-agent lenalidomide maintenance thereafter")
37
RVD consolidation 37 Overall median PFS 32/12, 3 year OS 93%

38
ASCT and maintenance

39
39

42
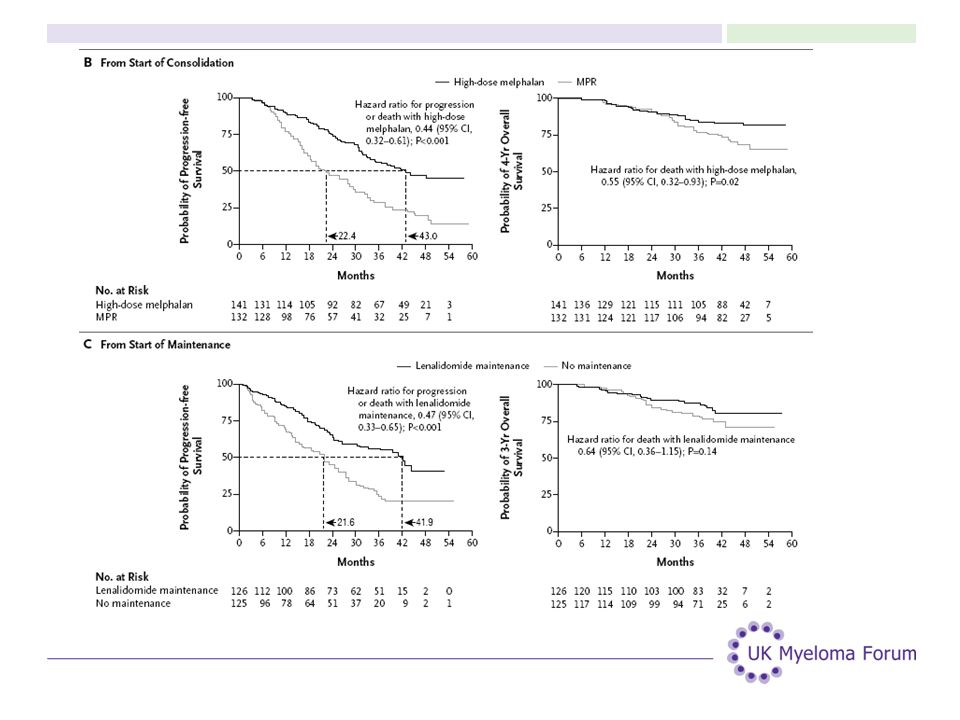
PFS Mel 200 x2 vs. MPR Len maint vs. not

43
Therapy of high risk myeloma Potential conclusions 43 Thalidomide minimal benefit during induction Thalidomide adverse as maintenance Bortezomib partially overcomes adverse risk associated with t(4;14) myeloma Bortezomib may overcome adverse risk associated with del17p myeloma Impact on GEP defined high risk myeloma unclear Tandem autologous transplant superior to MPR consolidation in high risk myeloma Lenalidomide maintenance unclear in high risk myeloma All needs formal randomised evaluation
 myeloma Bortezomib may overcome adverse risk associated with del17p myeloma Impact on GEP defined high risk myeloma unclear Tandem autologous transplant superior to MPR consolidation in high risk myeloma Lenalidomide maintenance unclear in high risk myeloma All needs formal randomised evaluation")
44
MUK9 Optimum study

45
Introduction: High risk myeloma accounts for 20-30% of presenting cases This subset of patients do not benefit from current treatment approaches There is a need for this population to develop both Good diagnostic tools to identify these patients New treatment strategies The high risk trial is a specific trial geared towards fit newly diagnosed high risk patients Registration phase: identify high risk patients Treatment phase: investigate 2 new treatment approaches Evaluate alongside anticipated best treatment including maintenance

46
Cytogenetic inter-relationship 1 7 Deletion 1p- (n=71) Deletion 17p (n=74) Adverse translocation (n=144) 6 2 135 60 61 Number gained Frequency 1p- 10% 1q+ 34% 17p 9% Adverse Translocation 21% GEP 20% Overall 25-35% 1 7 Deletion 17p (n=74) Adverse (n=144) 18 65 71 48 180 Gain 1q (n=264) 20 18 14 EMC92 Cytogenetics Myeloma IX data
 Deletion 17p (n=74) Adverse translocation (n=144) Number gained Frequency 1p- 10% 1q+ 34% 17p 9% Adverse Translocation 21% GEP 20% Overall 25-35% 1 7 Deletion 17p (n=74) Adverse (n=144) Gain 1q (n=264) EMC92 Cytogenetics Myeloma IX data")
47
Diagnosing high risk myeloma Our current definition of high risk is based on: - a full blood-count to identify Plasma cell leukaemia - A PCR based expression assay to identify translocations - MLPA to identify copy number changes such as 1q+, 1p- and 17q - Gene expression profile for High risk profile (EMC92 score) Kuiper et al (2009) Kaiser et al (2013)
 Kuiper et al (2009) Kaiser et al (2013)")
48
Daratumumab Daratumumab is monoclonal antibody Targets CD38 and has multiple mechanisms of action against CD38+ MM cells including -ADCC (antibody dependant cytotoxicity) -ADCP (antibody dependant cell phagocytosis) -Apoptosis -Modulating the enzymatic activity of CD38 (Cell adhesion) Demonstrated activity in MM Enhances the potency of other MM drugs such as Lenalidomide offering an interesting alternative to chemotherapy in myeloma.
 -ADCP (antibody dependant cell phagocytosis) -Apoptosis -Modulating the enzymatic activity of CD38 (Cell adhesion) Demonstrated activity in MM Enhances the potency of other MM drugs such as Lenalidomide offering an interesting alternative to chemotherapy in myeloma.")
49
MUK9 Optimum study concepts Arm A: intensive, chemotherapy-rich, DNA damaging. Hit multiple sub-clones Arm B: Alkylator light to minimise secondary genetic events. Multi- agent non-DNA damaging agents Arm C: standard arm

50
Pre-Screening 1200 newly diagnosed myeloma patients 20-30% lost 20-30% High risk 70% Standard risk 15-20% t(11;14) 60 % Hyper diploidy Other High risk trial Other trials
 60 % Hyper diploidy Other High risk trial Other trials")
51
Trial design Registration phase: 1200 newly diagnosed patients 8 week turnaround time Randomise 50 patients per arm Expand by another 35 patients in best arm vs. Control Aim to open early 2015 Newly diagnosed patients CTD CVD CRD VTD Induction X2 cycles Max VDT-PACE X 2 CVRDd CRD Split HDM-V ASCT HDM ASCT Rd Define high risk status VRDdX6 HDM ASCT R To progression Rd HDM-V ASCT VRdX12 VRDdX6 VRdX12

52
Endpoints: Primary phase II: PFS Abilility to turn around risk-defining investigations within 8 weeks Secondary Overall survival Deliverability of treatment Clinical benefit rate Maximum overall response Time to progression Time to maximum response Response at first relapse Safety Toxicity Recruitment rate Exploratory: To evaluate the potential to reduce genome instability by altering treatment strategies avoiding excessive alkylating agent exposure.

53
Follow-on from MUK9 Optimum study Phase 2/3 expansion National Phase 3 study: NCRI portfolio Pick a winner concept Define best arm to evaluate against standard arm Potential to establish a high risk “backbone” on to which newer agents can be added Added benefit of providing baseline risk-based classification that may feed in to other studies

54
Acknowledgements 54 ICR/RMH o Gareth Morgan o Faith Davies o Martin Kaiser o Eileen Boyle Myeloma CTN o Eric Low o Heather MacKinnon o Jennifer Fraser o Gordon Cook o Guy Pratt Leeds CTRU o Sarah Brown o Louise Flanagan Wessex Regional Genetics Lab o Fiona Ross o Laura Chiecchio

Similar presentations


1 CHILDHOOD LEUKAEMIA. TA OGUNLESI (FWACP)2 LEUKAEMIA Heterogenous group of malignant disorders Characterised by uncontrolled clonal.>")


 Idiopathic Associated with other diseases (autoimmune, infectious, non-heme.>")









>")




