Download presentation
Presentation is loading. Please wait.

1
Susanna Cooper, MPH MOAPC Coordinator, City of Quincy

2
Background on the Quincy MOAPC Cluster Participating communities Quincy Braintree Weymouth Stoughton Randolph Communities were selected based on past history of collaboration with Impact Quincy, need, and capacity to implement programs

3
MassCALL2 2008-2013: City of Quincy awarded MassCALL2 to address rising rates of fatal and non-fatal opioid overdose Impact Quincy (IQ) subcontracts Local strategies included OD prevention education to high risk individuals Establishing a Quincy Learn to Cope chapter Quincyoverosehelp.org Train the trainer overdose signs and first aid, to be presented to service providers, health officials, law enforcement, etc. in Quincy, Braintree, and Weymouth

4
MassCALL2 Frustration with limitations of grant and inability to outreach to neighboring communities doing similar work Appealed to DPH Pre-existing relationship with stakeholders in Braintree and Weymouth DPH realized that with the same amount of money, you can take a regional approach and make a bigger impact Greater return on investment

5
MassCALL2 Final Strategies & Collaborations Between 2008 and 2013 IQ: Instituted semi-annual Drug Take Back Day in collaboration with Quincy, Braintree, Milton, and Weymouth Established Braintree Drug Task Force Now called the Mayor’s Partnership on Substance Abuse Worked with DA to install MedReturn kiosks in 24 Norfolk County communities Organized an overdose vigil, collaborating with Braintree, Weymouth, and Randolph

6
Preparing for the MOAPC RFR Quincy, Braintree, Randolph, and Weymouth identify opioid abuse and overdose as major public health issues in their communities Representatives come together in July of 2012 stating their commitment to prevention work regardless of funding status Crucial for sustainability With knowledge that a new RFR would be released in early 2013, the plan was to apply as a cluster of municipalities First meeting included representatives from municipalities (mayors, health dept), law enforcement, and pharmacists Hired Interaction Institute for Social Change (IISC) to facilitate
, law enforcement, and pharmacists Hired Interaction Institute for Social Change (IISC) to facilitate")
7
Formation of the “Design Team” The meeting in July was too ‘touchy feely’ for some, and caused frustration among ‘action oriented’ individuals Reassess purpose and best practice Design Team was formed as a smaller group who would meet often, get input from stakeholders, and use input to inform a strategic plan moving forward Design Team would eventually become the MOAPC Cluster Stoughton inquired about partnering, and was selected based on data and high capacity to implement prevention strategies

8
January 2013: DPH Releases the MOAPC RFR When the RFR was released, our Design Team was already far ahead of the curve Coordinator worked to tailor IISC facilitation based on group needs

9
Prior to the release, we had coordinated an assessment Each community spent 3-4 months collecting data and conducting key informant interviews Assessment process helped me to “assess capacity” across all 5 communities IISC facilitators helped us to develop timelines and action steps, and kept meetings tightly facilitated

10
Regional Opioid Conference IQ sponsored a conference in collaboration with our selected MOAPC communities Issues with autonomy and ability to make decisions as a newly formed Design Team Conference was being funded with MassCALL2 dollars; this was not made clear MOAPC communities wanted to use this conference as an opportunity to do capacity building and more data collection; feared this was getting overlooked as we finalized the agenda Highlighted successes and past collaboration, but there was confusion as to who could design the agenda, present, and make decisions Conference was extremely successful, but the experience led to awareness that we NEEDED a decision making process for our group

11
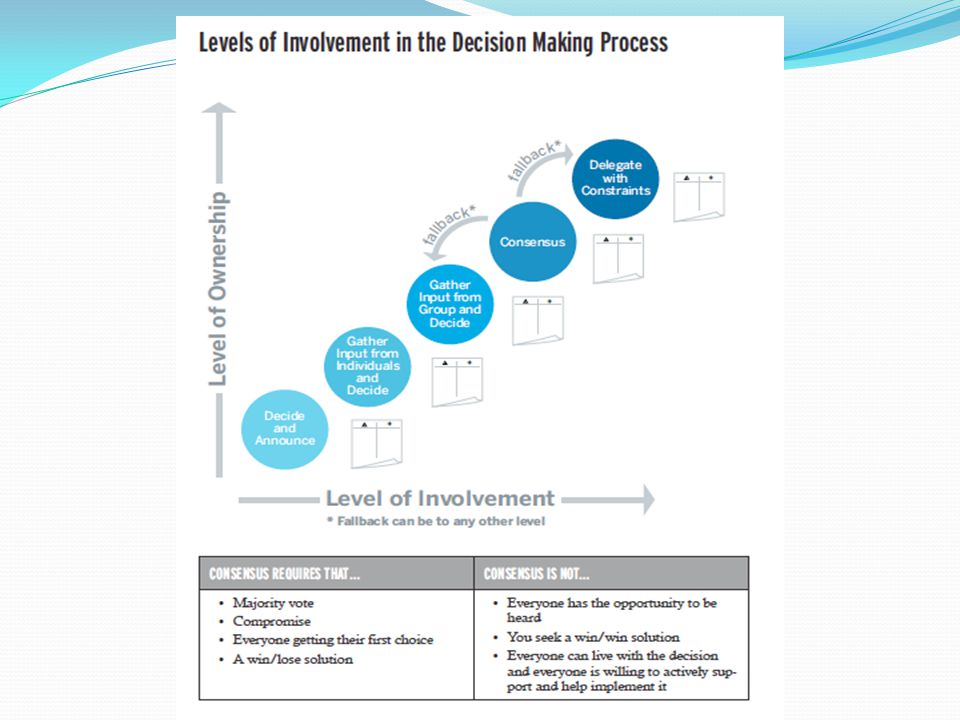
Decision Making Imperative to have a well thought out decision making process After the experience with the conference, cluster members were concerned that they were giving “token input” Often people think they are at the “consensus table”, when really they’re at the “input table”

13
Evaluating Realistic Scenarios As you begin your work, you may begin to see barriers that hinder your ability to make a final decision School board does not approve a project Mayor/Town Manager does not give you full support Budgetary constraints ?? Example: In our cluster, there was concern that even though the group was deemed a “decision making body”, the Program Director would not approve of the final decision

14
Cluster’s Proposed Solutions Agree to keep in constant contact with Program Director (PD) A month prior to any due date, submit what we need to PD so that we have a two week window to make changes Plan for PD to be at this table for high stakes decisions or for decisions he is most invested in Know what the constraints are beforehand Figure out how to leverage PD’s wisdom and knowledge
 A month prior to any due date, submit what we need to PD so that we have a two week window to make changes Plan for PD to be at this table for high stakes decisions or for decisions he is most invested in Know what the constraints are beforehand Figure out how to leverage PD’s wisdom and knowledge")
15
Consensus a definition The leader has no more authority in the decision than anyone else. We are equal in power at this table. Once group agrees to go forward with something, everyone supports the decision and is willing to help implement that agreement. Consensus may not be reached in the allotted meeting time, so we must have a fallback plan “if by the end of this hour if we cannot reach consensus, the decision will be made in this way” Option: Delegate to an appointed person or subcommittee

16
How our cluster makes decisions… We will make decisions by consensus Fallback: if we cannot reach consensus in time allotted, we will accept a majority vote (4 out of 5 communities) Each community has one voice regardless of how many reps. are at the table TA Provider does note vote

17
For high stakes decisions: We will make provisional consensus agreements if someone is absent OR if Alejandro needs to be involved Alejandro is a separate voice representing Bay State (grant holder) and not part of the Quincy voice High stakes decisions are: Intervening variables Strategies What we’re prioritizing out of the data + methods we are using Pilot strategies
 and not part of the Quincy voice High stakes decisions are: Intervening variables Strategies What we’re prioritizing out of the data + methods we are using Pilot strategies")
18
Real Examples of Consensual Decisions Intervening variables, strategies, and logic model Core measure questions for youth health surveys Looking for consistency in questions asked across our region Allotting additional funds for data analysis Allotting additional funds to support specific cluster communities (projects that would benefit MOAPC) In all of these scenarios, we have used our decision making method to reach consensus
 In all of these scenarios, we have used our decision making method to reach consensus")
19
Where We Are Today Strategic plan was approved by DPH in Spring of 2014 Selected strategies: Provide overdose prevention education to substance using inmates at Norfolk County House of Corrections Educate around Good Samaritan Law and the importance of calling 9-11 for active users and peers Develop a social marketing campaign to middle school parents Implement Scope of Pain training for regional prescribers Development of educational materials for parents

20
Challenges Strategic Prevention Framework (SPF) Not everyone likes to “move slow to move fast” Sometimes “process” is a difficult sell Every community has different capacity and different ability 2 communities are funded by DFC, 2 communities are unfunded Development of culturally appropriate strategies and materials
 Not everyone likes to move slow to move fast Sometimes process is a difficult sell Every community has different capacity and different ability 2 communities are funded by DFC, 2 communities are unfunded Development of culturally appropriate strategies and materials")
21
Contact: Susanna Cooper (617) 471-8400 x 191 scooper@baystatecs.org
 x 191")
Similar presentations







 7/3/20151.>")











