Download presentation
Presentation is loading. Please wait.

1
MRCP: technique and interpretation “10 rules in MRCP”
Lieven Van Hoe MD PhD OLV Hospital Group Aalst - Belgium

2
Procedure Axial and coronal double echo HASTE (5mm) NON-FATSAT
 NON-FATSAT")
3
10% of your patients has focal liver lesions Double echo HASTE: lesion characterizarion
cyst ++ / +++ as bright as CSF hemangioma + / ++ not as bright as CSF solid ± / + ± isointense

4
solid 60 msec 360 msec hemangioma

5
Axial and coronal double echo HASTE (5mm)
Thin-section MRCP Scout for breath-hold single-slice MRCP

6
Single-slice MRCP Procedure - RARE sequence
slice thickness 3 cm, TE 1100 3 sec / image breath hold = overview images

7
Axial non-FATSAT turboFLASH T1
Procedure Axial non-FATSAT turboFLASH T1 = magic tool for detection of pancreatic cancer and focal liver lesions Liver white Pancreas white Tumor dark

8
Multiphase contrast-enhanced VIBE
Procedure Multiphase contrast-enhanced VIBE Problem-solving tool Pancreatic lesions Only if required T P

9
Never use MRCP without cross-sectional imaging
Rule N° 1 Never use MRCP without cross-sectional imaging

10
Man, 43-year, elevated liver enzymes, previously papillotomy for biliary stone disease. Stone?
Figure 8: susceptbility artifact: aerobilia. Single-slice MRCP image obtained in a patient who underwent ERCP and papillotomy (a) shows heterogenous low signal intensity in lumen of dilated CBD (arrows): aerobilia? Stones? Axial T2-weighted image (b) shows an air-fluid level in the lumen of the CBD (arrow), which is diagnostic of aerobilia. Careful inspection of all axial images did not reveal stones in the dependent portion of the CBD lumen. Also note presence of naso(biliairy) ? tube (arowhead in b.). In patients with more extensive aerobilia and less fluid in the CBD, it may be impossible to exclude the presence of CBD stones, even with careful inspection of axial images.
 shows heterogenous low signal intensity in lumen of dilated CBD (arrows): aerobilia Stones Axial T2-weighted image (b) shows an air-fluid level in the lumen of the CBD (arrow), which is diagnostic of aerobilia. Careful inspection of all axial images did not reveal stones in the dependent portion of the CBD lumen. Also note presence of naso(biliairy) tube (arowhead in b.). In patients with more extensive aerobilia and less fluid in the CBD, it may be impossible to exclude the presence of CBD stones, even with careful inspection of axial images.")
11
Always correlate with axial T2-weighted images !!
Aerobilia Always correlate with axial T2-weighted images !! Air-fluid level Extensive air may make MRCP nondiagnostic

12
Liver function abnormalities
Figure 20. Limitations of ductal imaging: the invisible pancreatic carcinoma. Patient with biochemical signs of biliary obstruction. Single-slice MRCP (a) reveals biliary dilatation without visible lithiasis. The pancreatic duct appears normal. T1-weighted image (b) surprisingly reveals a hypointense mass in the pancreatic tail (arrow). On T2-weighted images (c), this mass was nearly isointense to normal pancreatic parenchyma. Final diagnosis was pancreatic adenocarcinoma. The diagnosis would have been missed completely if cross-sectional T1-weighted images were not obtained.
 reveals biliary dilatation without visible lithiasis. The pancreatic duct appears normal. T1-weighted image (b) surprisingly reveals a hypointense mass in the pancreatic tail (arrow). On T2-weighted images (c), this mass was nearly isointense to normal pancreatic parenchyma. Final diagnosis was pancreatic adenocarcinoma. The diagnosis would have been missed completely if cross-sectional T1-weighted images were not obtained.")
13
Missed pancreatic carcinoma
Never perform MRCP without cross-sectional imaging never, never, never TFLASH: 700 msec/slice – HASTE: 400 msec / slice

14
Use dynamic (repetitive) MRCP
Rule N° 2 Use dynamic (repetitive) MRCP
 MRCP.")
15
Figure 3. Use of single-slice MRCP to assess the contractile function of the sphincter of Oddi. Single-slice MRCP image (a) and enlarged view of the sphincter area (b) display common bie duct and pancreatic duct. A small hypointense nodular structure is seen distally in the CBD (arrow in b). A second MRCP image obtained a few seconds later is shown in c. This image and the magnified view (d) reveal fluid within the sphincteric portion of the CBD (arrows). The hypointense nodular ‘lesion’ in the distal CBD has disappeared. Image c is obtained during sphincter relaxation, while a is obtained during sphincter contraction. The nodular ‘lesion’ in a is caused by forceful sphincter contraction (pseudocalculus sign, see also figure 26). By comparing images a and c, it can be concluded that the sphincter exhibits contractile activity and that no lithiasis is present. May 13, 2003 10hr:12min:15sec May 13, 2003 10hr:12min:23sec

16
Temporal variability in shape of the sphincter of Oddi It works !
Only possible with breath-hold single-slice MRCP

17
Use the correct slice thickness Not 10 cm !
Rule N° 3 Use the correct slice thickness Not 10 cm !

18
10cm 5cm 2cm 3cm Figure 4. Single-slice MRCP: effect of slice thickness Four single-slice MRCP images obtained with identical slice position and slice orientation but with different slice thickness are compared. Slice thickness: a: 2cm, b: 3cm; c: 5 cm; d: 10 cm. The CBD is best seen in b. Images c. and d. suffer from lower contrast and more superimposition artifact.

19
Be aware of biliary flow phenomena on axial images
Rule N° 5 Be aware of biliary flow phenomena on axial images

20
Flow void in common bile duct
axial T2 Flow void in common bile duct Compare with single-slice MRCP Believe single-slice MRCP if results are different

21
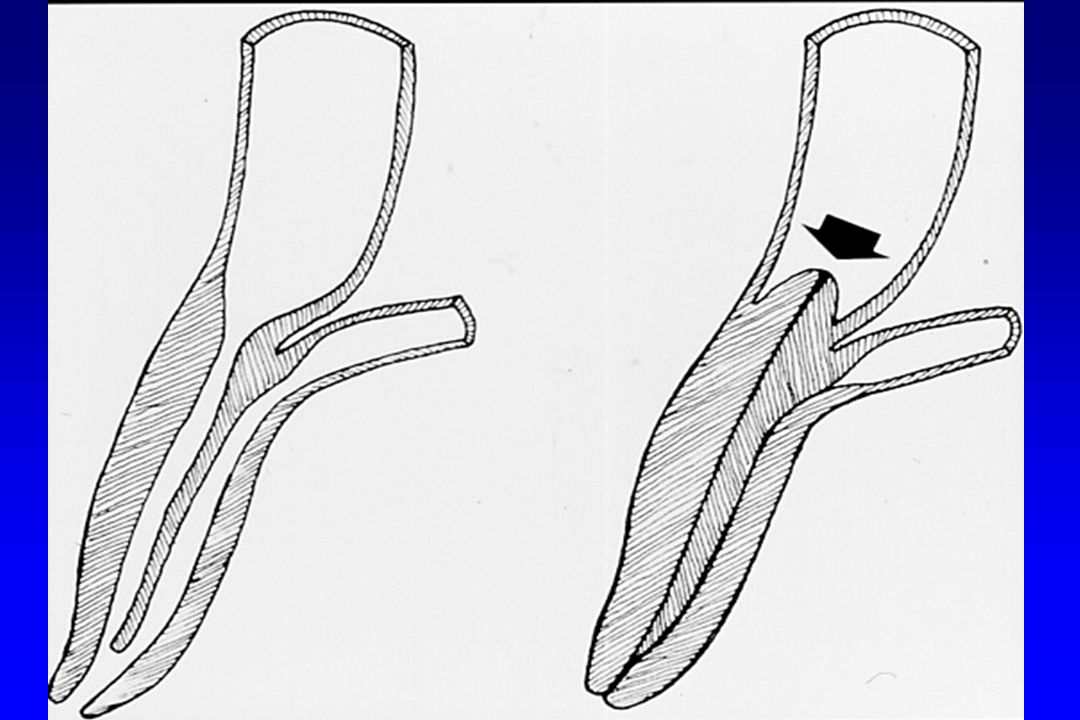
Be aware of the pseudo-calculus sign
Rule N° 6 Be aware of the pseudo-calculus sign

22
Pseudocalculus sign 30 sec later

24
Small stones not surrounded by fluid are invisible
Rule N° 7 Small stones not surrounded by fluid are invisible

25
Not included in slice Does the patient has stones in distal CBD ??
Normal size

26
May be difficult diagnosis ! Repetitive imaging useful
Impacted stone Ermens Andre PG Figure 35. False negative prospective MRCP diagnosis of CBD lithiasis. Patient referred to rule out biliary lithiasis. Single-slice MRCP image (a) was interpreted as normal. Because of persistent symptoms, ERCP was performed. ERCP image (b) shows several small stones in the distal portion of the CBD (arrows). Retrospectively, these can also be suspected at MRCP: magnified view of a. shows nodular structure in distal CBD, surrounded by only a small amount of fluid and thus barely visible (c, arrow) (s, sphincter segment). Axial T2-weighted image (d) confirms presence of a very small stone in the dependent portion of the CBD. May be difficult diagnosis ! No surrounding fluid Repetitive imaging useful
 was interpreted as normal. Because of persistent symptoms, ERCP was performed. ERCP image (b) shows several small stones in the distal portion of the CBD (arrows). Retrospectively, these can also be suspected at MRCP: magnified view of a. shows nodular structure in distal CBD, surrounded by only a small amount of fluid and thus barely visible (c, arrow) (s, sphincter segment). Axial T2-weighted image (d) confirms presence of a very small stone in the dependent portion of the CBD. May be difficult diagnosis ! No surrounding fluid. Repetitive imaging useful.")
28
Anticipate differences between MRCP and ERCP images
Rule N° 8 Anticipate differences between MRCP and ERCP images

29
MRCP: - imaging in the physiologic state
MRCP: - imaging in the physiologic state (no ductal distention) - limitations in spatial resolution Low-grade stenoses can be missed The length of stenoses can be overestimated (physiologic collapse) Small polypoid ductal lesions can be missed
 - limitations in spatial resolution. Low-grade stenoses can be missed. The length of stenoses can be overestimated (physiologic collapse) Small polypoid ductal lesions can be missed.")
30
MRCP – ERCP The same things look different !! (distention)
")
31
Aberrant right posterior duct
Figure 12. Imaging in the physiologic state: the invisible stenosis Patient who underwent cholecystectomy. Single-slice MRCP image (a) shows aberrant right posterior duct draining into the common hepatic duct in close proximity to the cystic duct (arrow). Corresponding ERCP image (b) confirms the presence of an aberrant right posterior hepatic duct. Moreover, it shows a short stenosis of this duct (arrowheads), probably related to trauma dusing cholecystectomy. Note that this stenosis is not well seen in a. Reprinted with permission from reference 1 (fig 27)
 shows aberrant right posterior duct draining into the common hepatic duct in close proximity to the cystic duct (arrow). Corresponding ERCP image (b) confirms the presence of an aberrant right posterior hepatic duct. Moreover, it shows a short stenosis of this duct (arrowheads), probably related to trauma dusing cholecystectomy. Note that this stenosis is not well seen in a. Reprinted with permission from reference 1 (fig 27)")
32
Figure 14. Spatial resolution
Patient with CBD lithiasis. Single-slice MRCP (a) reveals CBD lithiasis (arrow). The portion of the pancreatic duct included in the slice appears normal. ERCP image (b) shows small eccentric lacunar image in pancreatic duct (small mucus plug ?) (arrow), which is invisible at MRCP. This may be related to a combination of more limited spatial resolution and lack of ductal distention.
 reveals CBD lithiasis (arrow). The portion of the pancreatic duct included in the slice appears normal. ERCP image (b) shows small eccentric lacunar image in pancreatic duct (small mucus plug ) (arrow), which is invisible at MRCP. This may be related to a combination of more limited spatial resolution and lack of ductal distention.")
33
Rule N° 9 For lesion characterization, use all information available (T1, T2, MRCP, multiphase contrast-enhanced images)
")
34
Cirrhosis. Incidental finding.
Figure 34. Peribiliary varices mimicking polypoid bile duct mass. Single-slice MRCP image (a) reveals severe narrowing of the proximal extrahepatic duct (arrowheads), possibly representing an impacted stone or a polypoid tumor. Axial contrast-enhanced T1-weighted images (b,c) show the absence of a normal portal vein with formation of multiple collaterals (cavernous transformation) (arrows in b.) and extrahepatic venous collaterals (arrowheads in b.). The focal narrowing of the bile duct is explained by the presence of large peribiliary venous collaterals (arrowheads in c.).
 reveals severe narrowing of the proximal extrahepatic duct (arrowheads), possibly representing an impacted stone or a polypoid tumor. Axial contrast-enhanced T1-weighted images (b,c) show the absence of a normal portal vein with formation of multiple collaterals (cavernous transformation) (arrows in b.) and extrahepatic venous collaterals (arrowheads in b.). The focal narrowing of the bile duct is explained by the presence of large peribiliary venous collaterals (arrowheads in c.).")
35
The double duct sign can be caused by chronic pancreatitis with pseudomass. Refer to axial T1- and T2-weighted images for differentiation with carcinoma. Figure 21. Limitations of ductal imaging: double duct sign in chronic pancreatitis. Patient with biochemical signs of biliary obstruction. Single-slice MRCP image (a) showing narrowing of the distal CBD and pancreatic duct (double duct sign), suggesting pancreatic cancer. However, T1-weighted image (b) shows that the pancreatic head has a preserved high signal intensity (arrows), which almost exludes pancreatic cancer as a possibility. Axial T2-weighted image (c ) reveals small air- and fluid-filled pseudocyst adjacent to the pancreatic tail (arrow). Also note thickening of adjacent gastric wall (arrowheads). Both findings suggests presence of a small pancreatogastric fistula. T2-weighted images obtained at lower levels revealed a tortuous course of the pancreatic duct, without marked dilatation, which, again, makes pancreatic carcinoma unlikely. Final diagnosis was chronic pancreatitis with pseudocyst. An almost complete regression of the abnormalities was observed at a control MRI exam two months later.
 showing narrowing of the distal CBD and pancreatic duct (double duct sign), suggesting pancreatic cancer. However, T1-weighted image (b) shows that the pancreatic head has a preserved high signal intensity (arrows), which almost exludes pancreatic cancer as a possibility. Axial T2-weighted image (c ) reveals small air- and fluid-filled pseudocyst adjacent to the pancreatic tail (arrow). Also note thickening of adjacent gastric wall (arrowheads). Both findings suggests presence of a small pancreatogastric fistula. T2-weighted images obtained at lower levels revealed a tortuous course of the pancreatic duct, without marked dilatation, which, again, makes pancreatic carcinoma unlikely. Final diagnosis was chronic pancreatitis with pseudocyst. An almost complete regression of the abnormalities was observed at a control MRI exam two months later.")
36
Be aware of susceptibility artifact
Rule N° 10 Be aware of susceptibility artifact

37
Figure 9. Susceptibility artifact: metallic clips
Figure 9. Susceptibility artifact: metallic clips. Pseudostenosis due to signal loss caused by a surgical clip used in cholecystectomy. (a) Multisection MRCP image shows false stenosis of the CHD (arrow). The appearance of the stenosis resembles that of a bile duct tumor. No dilatation of the upstream biliary tree is seen. (b) Drip-infusion cholangiogram reveals three surgical clips (arrowheads) near the normal CHD. Reprinted with permission from: Watanabe et al. Diagnostic Pitfalls of MR Cholangiopancreatography in the Evaluation of the Biliary Tract and Gallbladder. RadioGraphics : Watanabe et al. RadioGraphics :
 Multisection MRCP image shows false stenosis of the CHD (arrow). The appearance of the stenosis resembles that of a bile duct tumor. No dilatation of the upstream biliary tree is seen. (b) Drip-infusion cholangiogram reveals three surgical clips (arrowheads) near the normal CHD. Reprinted with permission from: Watanabe et al. Diagnostic Pitfalls of MR Cholangiopancreatography in the Evaluation of the Biliary Tract and Gallbladder. RadioGraphics : Watanabe et al. RadioGraphics :")
38
Susceptibility artifact air metal
Figure 9. Susceptibility artifact: metallic clips. Pseudostenosis due to signal loss caused by a surgical clip used in cholecystectomy. (a) Multisection MRCP image shows false stenosis of the CHD (arrow). The appearance of the stenosis resembles that of a bile duct tumor. No dilatation of the upstream biliary tree is seen. (b) Drip-infusion cholangiogram reveals three surgical clips (arrowheads) near the normal CHD. Reprinted with permission from: Watanabe et al. Diagnostic Pitfalls of MR Cholangiopancreatography in the Evaluation of the Biliary Tract and Gallbladder. RadioGraphics :
 Multisection MRCP image shows false stenosis of the CHD (arrow). The appearance of the stenosis resembles that of a bile duct tumor. No dilatation of the upstream biliary tree is seen. (b) Drip-infusion cholangiogram reveals three surgical clips (arrowheads) near the normal CHD. Reprinted with permission from: Watanabe et al. Diagnostic Pitfalls of MR Cholangiopancreatography in the Evaluation of the Biliary Tract and Gallbladder. RadioGraphics :")
39
Thank you !!

40
The double duct sign can be caused by chronic pancreatitis with pseudomass. Refer to axial T1- and T2-weighted images for differentiation with carcinoma. Figure 21. Limitations of ductal imaging: double duct sign in chronic pancreatitis. Patient with biochemical signs of biliary obstruction. Single-slice MRCP image (a) showing narrowing of the distal CBD and pancreatic duct (double duct sign), suggesting pancreatic cancer. However, T1-weighted image (b) shows that the pancreatic head has a preserved high signal intensity (arrows), which almost exludes pancreatic cancer as a possibility. Axial T2-weighted image (c ) reveals small air- and fluid-filled pseudocyst adjacent to the pancreatic tail (arrow). Also note thickening of adjacent gastric wall (arrowheads). Both findings suggests presence of a small pancreatogastric fistula. T2-weighted images obtained at lower levels revealed a tortuous course of the pancreatic duct, without marked dilatation, which, again, makes pancreatic carcinoma unlikely. Final diagnosis was chronic pancreatitis with pseudocyst. An almost complete regression of the abnormalities was observed at a control MRI exam two months later.
 showing narrowing of the distal CBD and pancreatic duct (double duct sign), suggesting pancreatic cancer. However, T1-weighted image (b) shows that the pancreatic head has a preserved high signal intensity (arrows), which almost exludes pancreatic cancer as a possibility. Axial T2-weighted image (c ) reveals small air- and fluid-filled pseudocyst adjacent to the pancreatic tail (arrow). Also note thickening of adjacent gastric wall (arrowheads). Both findings suggests presence of a small pancreatogastric fistula. T2-weighted images obtained at lower levels revealed a tortuous course of the pancreatic duct, without marked dilatation, which, again, makes pancreatic carcinoma unlikely. Final diagnosis was chronic pancreatitis with pseudocyst. An almost complete regression of the abnormalities was observed at a control MRI exam two months later.")
41
Be careful with MIP images
Rule N° 4 Be careful with MIP images

42
The patient recently underwent laparoscopic gallbladder surgery and now suffers from jaundice. Injury to CBD? Figure 1. Limitations of MIP images. Patient with jaundice after gallblader surgery. MIP image obtained after postprocessing of a series of thin slices (a) compared to single-slice MRCP with slice thickness 3cm (b). Both images show intrahepatic biliary dilatation. The single-slice MRCP image clearly reveals occlusion of the common hepatic duct (arrow). This diagnosis is missed on the MIP image because an intrahepatic bile duct superimposes on the CHD (arrow).
 compared to single-slice MRCP with slice thickness 3cm (b). Both images show intrahepatic biliary dilatation. The single-slice MRCP image clearly reveals occlusion of the common hepatic duct (arrow). This diagnosis is missed on the MIP image because an intrahepatic bile duct superimposes on the CHD (arrow).")
43
Projects 3D reality on 2D image Pathology may be masked
MIP Projects 3D reality on 2D image Pathology may be masked

Similar presentations


, body (20%), tail (10%) Median age 72 years (65-84 y/o) Most tumors are diagnosed.>")












: Principal.>")



: Principal Modality (2): Faculty.>")
 Faculty of allied medical sciences.>")