Download presentation
Presentation is loading. Please wait.

1
Timing and indications of surgery in stenotic and regurgitant valvular lesions Dr.Deepak Raju

2
Aortic stenosis Pathophysiology Assessment of severity Natural history Management strategy Role of exercise test,EBCT Recommendations

3
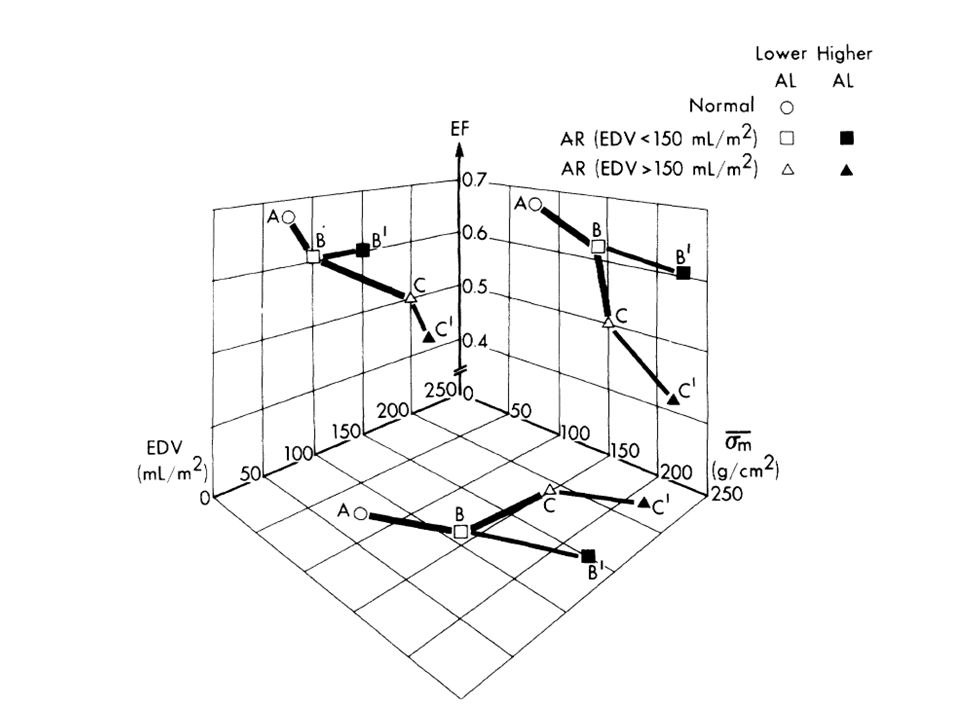
Concept of afterload mismatch Term coined by Ross et al (1976) Increasing aortic pressure increased LV contractility,LV volume and mass kept constant At a particular level contractility started decreasing-mismatch b/w afterload and contractile state
 Increasing aortic pressure increased LV contractility,LV volume and mass kept constant At a particular level contractility started decreasing-mismatch b/w afterload and contractile state")
4
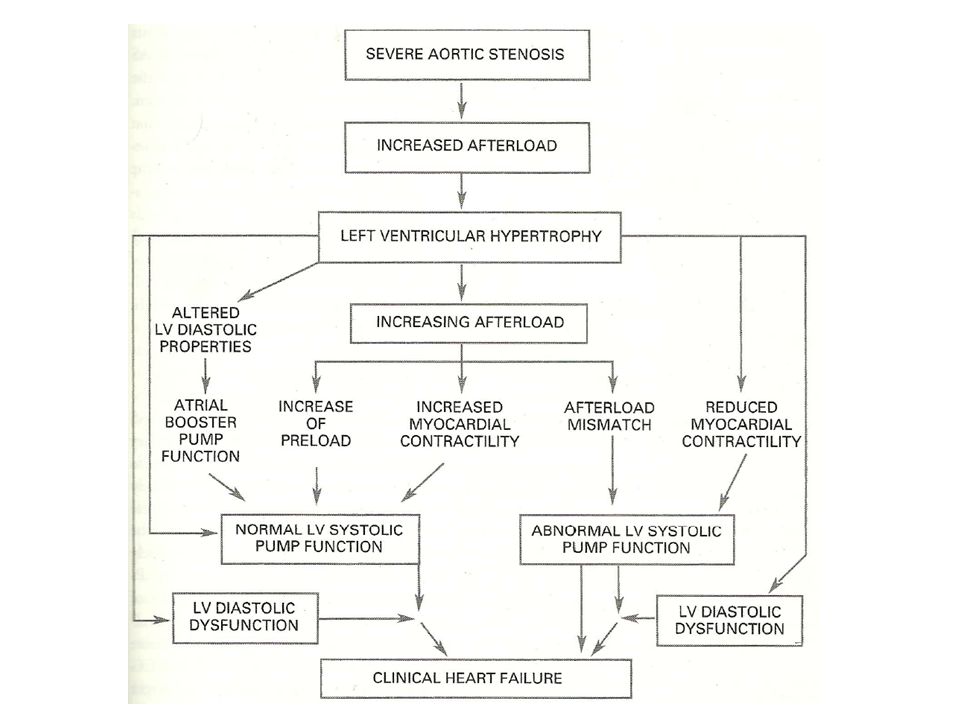
AS-pathophysiology Increasing severity of AS-matched by increasing LV mass and contractility Compensation by hypertrophy fails to sustain afterload Clinical afterload mismatch occurs LV utilizes preload reserve-mechanism by which stroke volume is maintained by increasing preload Preload reserve is not a good compensatory mechanism in AS(LV on steep portion of diastolic pressure volume loop) Systolic pump function fails once preload reserve is no longer adequate Earliest stage of LV dysfunction in severe AS
 Systolic pump function fails once preload reserve is no longer adequate Earliest stage of LV dysfunction in severe AS")
5
LV systolic dysfunction – Afterload mismatch and/or impaired contractility LV diastolic dysfunction – Laplace equation Stress =pressure.radius/2.wall thickness – Increased wall thickness compensates for pressure overload – Impaired relaxation&altered compliance-Diastolic dysfunction – Atrial booster pump maintains LV filling

7
Assessment of severity Jet velocity-reproducible,strongest predictor of clinical outcome Aortic valve area-continuity equation Velocity ratio- – suboptimal image of LVOT – effectively indexed for BSA – Ratio <0.25 indicates severe stenosis

9
Other measures of severity Stroke work loss – Ratio of mean PG to mean LV pressure – >26% predictive of probability of cardiac death or AVR Energy loss index – Calculated from aortic valve area and area of aorta at sinotubular junction – Severe AS <0.55 cm2/m2 Valvulo arterial impedance – Reflects degree of valve obstruction,ventricular response and systemic vascular impedance – survival lower in patients with Zva >4.5 mmHg/ml/m2 (Zeineb et al JACC 2009)
")
13
Natural history Prolonged latent period Rate of progression of stenosis of moderate severity – Jet velocity 0.3 m/s/yr – Gradient 7 mmHg/yr – Area 0.1 cm2/yr

14
Asymptomatic adult-AS

15
Pellikka et al.circulation 2005,622 pts,mean follow up 5.4 yr

16
Other findings(Pellikka et al ) – Patients with jet velocity >4.5 m/s had greater likelihood of develpoing symptoms(relative risk 1.34) – Incidence of sudden cardiac death was 1% /yr
 – Patients with jet velocity >4.5 m/s had greater likelihood of develpoing symptoms(relative risk 1.34) – Incidence of sudden cardiac death was 1% /yr")
17
Asymptomatic patient-AS Patients with asymptomatic severe AS require frequent monitoring for devt.of symptoms In a meta analysis of seven studies the risk of sudden cardiac death was found to be 0.4%/yr(375 pts,mean follow up 2.1 yr)
")
18
Follow up – Clinical frequent monitoring for devt of symptoms every year for mild 6 mth for moderate and severe – TTE Every year for severe AS 1-2 year for moderate AS 3-5 year for mild AS – Patient education regarding devt of symptoms

19
Exercise testing May be considered in asymptomatic patients with unclear symptoms to elicit(IIb) – limited exercise capacity – exercise induced symptoms – Abnormal BP response
 – limited exercise capacity – exercise induced symptoms – Abnormal BP response")
20
Amato et al 2001,Heart 2001 – 66pts,14 mth follow up – Positive stress rest Horizontal or downsloping ST dep>1 mm (men ) &2mm (women)or upsloping ST>3mm in men Angina,near syncope Ventricular arrhythmia SBP fails to rise by 20 mmHg – Grp with Abnormal exercise response 19% symptom free survival at 2 yrs – Normal 85% symptom free survival at 2 yrs – 6% experienced SCD;all had positive stress test
 &2mm (women)or upsloping ST>3mm in men Angina,near syncope Ventricular arrhythmia SBP fails to rise by 20 mmHg – Grp with Abnormal exercise response 19% symptom free survival at 2 yrs – Normal 85% symptom free survival at 2 yrs – 6% experienced SCD;all had positive stress test")
22
Das P et al, Eur Heart J,2005 – 125 pts,12 mth follow up – Positive test Limiting symptoms(chest tightness,breathlessness,dizziness) Abnormal BP response(BP at peak exercise same or below baseline) ST dep >2mm – Exercise limiting symptoms independent predictor of outcome – Exercise brought out symptoms in 37% pts – In this group spontaneous symptoms developed in 51% compared to 11% in others
 Abnormal BP response(BP at peak exercise same or below baseline) ST dep >2mm – Exercise limiting symptoms independent predictor of outcome – Exercise brought out symptoms in 37% pts – In this group spontaneous symptoms developed in 51% compared to 11% in others")
24
Management strategy In most asymptomatic patients with aortic stenosis,risk of surgery(3-4% for AVR-STS database) is higher than risk of watchful waiting Early surgery – older pts to higher mortality(8.8% in >65 yr, US medicare data) – Younger pts-morbidity and mortality of prosthetic valve
 is higher than risk of watchful waiting Early surgery – older pts to higher mortality(8.8% in >65 yr, US medicare data) – Younger pts-morbidity and mortality of prosthetic valve")
25
Early AVR may be considered – Severe valve calcification – Rapid progression Increase in jet velocity >0.3 m/s/yr Decrease in valve area >0.1 cm2 /yr – Expected delays in surgery

26
Symptomatic AS Critical point in natural history of AS Average survival is 2-3 years High risk of sudden cardiac death AVR improves symptoms and survival

27
Ross J Jr, Braunwald E: Aortic stenosis. Circulation 38:61, 1968

28
Low flow low gradient aortic stenosis Dobutamine stress echocardiography(IIa) – Transvalvular PG,valve area calculated in baseline and low dose dobutamine stress Severe AS-fixed valve area,increase in stroke volume and gradient AS not severe-valve area increases >0.2 cm2,increase stroke volume,no change in gradient Lack of contractile reserve-increase in stroke volume <20%-poor prognosis with medical or surgical therapy
 – Transvalvular PG,valve area calculated in baseline and low dose dobutamine stress Severe AS-fixed valve area,increase in stroke volume and gradient AS not severe-valve area increases >0.2 cm2,increase stroke volume,no change in gradient Lack of contractile reserve-increase in stroke volume <20%-poor prognosis with medical or surgical therapy")
29
Cardiac biomarkers Berger klein et al(circulation 2004) – 130 pts with severe AS – NT-BNP < 80 pmol/L predicted symptom free survival in asymptomatic patients followed up for one year(69% vs 18%)
 – 130 pts with severe AS – NT-BNP < 80 pmol/L predicted symptom free survival in asymptomatic patients followed up for one year(69% vs 18%)")
30
EBCT Messika et al (circulation 2004) Valve calcification assessed by EBCT Event-free survival at 5 years was 92% Vs 40% comparing grps above and below 500 Agatston units
 Valve calcification assessed by EBCT Event-free survival at 5 years was 92% Vs 40% comparing grps above and below 500 Agatston units")
31
Recommendations for AVR Class I – Severe AS and symptoms – Severe AS (with or without symptom) need for CABG,valve replacement or aortic surgery – Severe AS and LV systolic dysfunction(EF <50 %) Class IIa – Moderate AS and need for other cardiac surgery
 need for CABG,valve replacement or aortic surgery – Severe AS and LV systolic dysfunction(EF <50 %) Class IIa – Moderate AS and need for other cardiac surgery")
32
Class II b – asymptomatic severe AS With abnormal exercise response(devt.of symptoms,hypotension) Likelihood of rapid progression,expected delays at symptom onset Extremely severe AS(area 60mmHg,jet velocity>5 m/s) with expected mortality<1% Mild AS undergoing CABG,evidence of rapid progression Not useful for prevention of SCD in asymptomatic severe AS without above criteria
 Likelihood of rapid progression,expected delays at symptom onset Extremely severe AS(area 60mmHg,jet velocity>5 m/s) with expected mortality<1% Mild AS undergoing CABG,evidence of rapid progression Not useful for prevention of SCD in asymptomatic severe AS without above criteria")
35
Aortic balloon valvotomy Class II b – Bridge to surgery in hemodynamically unstable patient who are at high risk for AVR – Palliation in whom AVR cannot be performed

36
Indications of BAV in adolescents and young adults Class I – Symptomatic AS(angina,syncope,DOE),PSG>50 mmHg,valve not heavily calcified – Asymptomatic,PSG >60 mmHg – Asymptomatic,PSG >50mmHg,with ST or T wave changes in left precordial leads at rest or with exercise Class II a – Asymptomatic,PSG > 50mmHg,wants to play competitive sports or planning pregnancy – When possible BAV preferred over surgery in adolescent or young adult
,PSG>50 mmHg,valve not heavily calcified – Asymptomatic,PSG >60 mmHg – Asymptomatic,PSG >50mmHg,with ST or T wave changes in left precordial leads at rest or with exercise Class II a – Asymptomatic,PSG > 50mmHg,wants to play competitive sports or planning pregnancy – When possible BAV preferred over surgery in adolescent or young adult")
37
AR-Pathophysiology AR –volume overload and pressure overload Volume overload – ↑ EDV – ↑ chamber compliance – Combination concentric and eccentric hypertrophy Pressure overload – ↑ chamber size- ↑ wall stress-elevates afterload Preload reserve and compensatory hypertrophy maintain ejection performance-asymptomatic patient

38
Latent phase of AR, like AS, may last decades Decompensation – Preload reserve exhausted – Hypertrophy inadequate – Impaired contractility LV systolic dysfunction-initially reversible-afterload excess Impaired contractility predominates later-irreversible – Chamber enlargement – Spherical geometry LV systolic function and ESD-most important predictors of postoperative survival and recovery of LV function

40
Natural history Asymptomatic patient with normal LV function – 9 published studies,593 patients,mean follow up of 6.6 yrs – 25% of patients who die or develop LV dysfunction do so before the onset of symptoms – Quantitative evaluation of LV function indispensable

41
Natural history

42
End systolic dimension in relation to devt of symptoms,LV Dysfunction or death Bonow et al,circulation 1991 – ESD>50mm-19% /yr – ESD 40-50 mm-6% /yr – ESD <40- 0%

43
Survival without surgery in symptomatic patients withAR

44
Symptomatic patients Poor outcome with medical therapy Mortality 10% /yr in patients with angina Mortality 20% /yr in heart failure

45
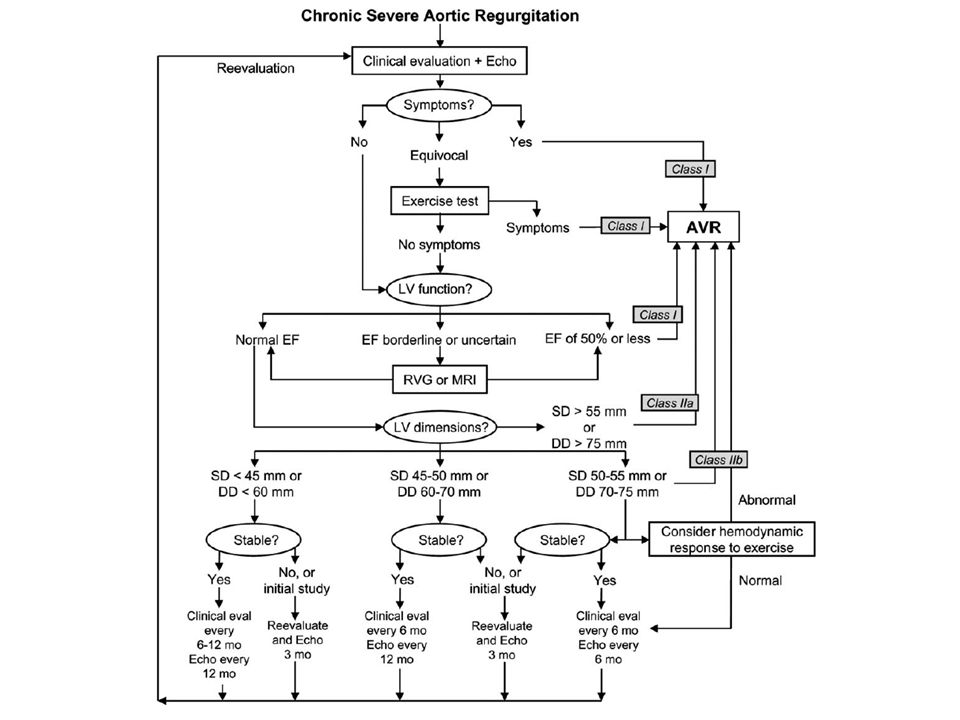
Indications for AVR or aortic valve repair Class I – Symptomatic severe AR – Asymptomatic severe AR with LVD(EF<0.50 at rest) CABG,valve surgery,aortic surgery Class II a – Asymptomatic severe AR with severe LV dilatation(EDD>75mm,ESD>55mm)
 CABG,valve surgery,aortic surgery Class II a – Asymptomatic severe AR with severe LV dilatation(EDD>75mm,ESD>55mm)")
46
Class II b – Asymptomatic severe AR with borderline LV dilatation(EDD 70-75,ESD 50-55) abnormal hemodynamic response to exercise progressive LV dilatation Declining exercise tolerance – Moderate AR undergoing CABG or aortic surgery
 abnormal hemodynamic response to exercise progressive LV dilatation Declining exercise tolerance – Moderate AR undergoing CABG or aortic surgery")
48
Bicuspid aortic valve with dilated ascending aorta Class I – Surgery to repair aortic root or replacement of ascending aorta Diameter of ascending aorta or root >5cm Rate of increase in size >0.5 cm/yr Diameter>4.5 cm undergoing AVR

49
Mitral stenosis Narrowing of valve area to < 2.5 cm2 occurs before devt.of symptoms Symptoms at rest occur when valve area <1.5 cm2 Developed countries- – Long latent period from RF to symptoms (20-40 years) – A decade from symptom onset to disabling symptoms Rpted streptococcal infection and recurrent carditis-rapid progression in poor countries
 – A decade from symptom onset to disabling symptoms Rpted streptococcal infection and recurrent carditis-rapid progression in poor countries")
50
Asymptomatic-10 yr survival-80% Symptomatic-0-15 % 10 yr survival Devt of PAH-mean survival <3 years annual loss of mtral valve area-0.09 cm2

51
Grading of severity MV area(cm2)Mean gradient(mmHg) PASP(mmHg) mild>1.5<5<30 Moderate1-1.55-1030-50 severe<1.0>10>50
Mean gradient(mmHg) PASP(mmHg) mild>1.5<5<30 Moderate severe<1.0>10>50")
55
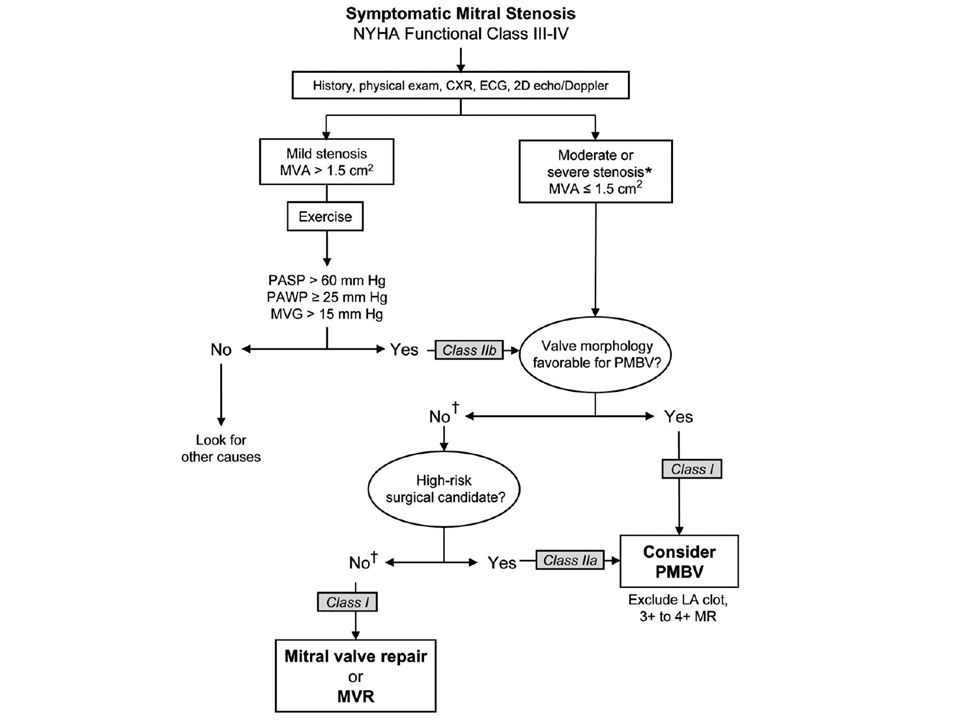
Indications for PMBV CLASS I – Symptomatic(II,III,IV) moderate or severe MS when valve morphology favourable – Asymptomatic moderate or severe MS,PASP>50 mmHg at rest or >60 mmHg with exercise Class IIa – Symptomatic (III,IV) moderate or severe MS,non pliable calcified valve if not candidates for surgery Class II b – Asymptomatic moderate MS when new AF – Symptomatic mild MS,exercise PASP >60 mmHg,PAWP>25mmHg,Mean grad >15 mmHg
 moderate or severe MS when valve morphology favourable – Asymptomatic moderate or severe MS,PASP>50 mmHg at rest or >60 mmHg with exercise Class IIa – Symptomatic (III,IV) moderate or severe MS,non pliable calcified valve if not candidates for surgery Class II b – Asymptomatic moderate MS when new AF – Symptomatic mild MS,exercise PASP >60 mmHg,PAWP>25mmHg,Mean grad >15 mmHg")
56
Indications for surgery CLASS I – Symptomatic(III or IV),moderate or severe MS PMBV unavailable or contraindicated Valve morphology not favourable Moderate MR CLASS II a – MV replacement in severe MS,class I or II symptoms,PASP>60 mmHg and not considered for PMBV
,moderate or severe MS PMBV unavailable or contraindicated Valve morphology not favourable Moderate MR CLASS II a – MV replacement in severe MS,class I or II symptoms,PASP>60 mmHg and not considered for PMBV")
57
Event free survival after BMV-50-65% at 3-7 yrs Survival higher (80%) in pts with favourable MV morphology
 in pts with favourable MV morphology")
58
MS in young adults,adolescents Class I – Symptomatic(III,IV) with MV mean gradient >10 mmHg Class IIa – MV gradient >10mmHg with Mild symptoms Asymptomatic with PASP>50 mmHg Type of surgery – Parachute MV-creation of fenestration among fused chordae – Annulus enlarging operation-hypoplastic mitral annulus – Ballon dilatation in congenital MS-usefulness limited
 with MV mean gradient >10 mmHg Class IIa – MV gradient >10mmHg with Mild symptoms Asymptomatic with PASP>50 mmHg Type of surgery – Parachute MV-creation of fenestration among fused chordae – Annulus enlarging operation-hypoplastic mitral annulus – Ballon dilatation in congenital MS-usefulness limited")
59
MR -pathophysiology Increased preload,reduced or normal afterload Eccentric cardiac hypertrophy Increased LVEDV-compensated phase Prolonged hemodynamic overload ultimately leads to myocardial decompensation Ejection phase indices are initially higher in c/c MR due to reduced afterload Once decompensation occurs –start decreasing Values in low normal range reflect impaired myocardial function

60
Mitral regurgitation Mild to moderate MR –asymptomatic for years Severe MR-asymtomatic for years-compensated phase Natural history of severe MR due to flail leaflet- Sarano et al,1996 – At 10 years 90% required MVR or dead – Mortality -6-7% /yr in MR by flail leaflets in pts with symptoms(class III,IV) or LV dysfunction(EF<60%)
 or LV dysfunction(EF<60%)")
62
Asymptomatic patient with normal LV fn – Sarano et al 2005 EROA>40 mm2 had 4% /yr risk of cardiac death(198 pts follow up 2.7 yr) – Rosenhek et al,2006 132 pts,5 yr follow up Indications of surgery were symptoms,LVD,LV dilatation,devt of PAH or AF One cardiac death in a patient who refused surgery
 – Rosenhek et al, pts,5 yr follow up Indications of surgery were symptoms,LVD,LV dilatation,devt of PAH or AF One cardiac death in a patient who refused surgery")
63
Surgery for asymptomatic patient with normal LV function –only considered if >90% likelihood of successful MV repair Rate of reoperation similar in MVR or MV repair(7% to 10%) at 10 yrs Operative mortality 2% for MV repair,6% for MVR(STS database)
 at 10 yrs Operative mortality 2% for MV repair,6% for MVR(STS database)")
64
Indications for surgery Class I – Symptomatic a/c severe MR – Symptomatic c/c severe MR(class II to IV) in the absence of severe LVD(EF 55mm) – Asymptomatic c/c severe MR with mild to moderate LVD(EF 30% to 60% and/or ESD >40mm) – MV repair recommended over MVR
 in the absence of severe LVD(EF 55mm) – Asymptomatic c/c severe MR with mild to moderate LVD(EF 30% to 60% and/or ESD >40mm) – MV repair recommended over MVR")
65
Class II a – Asymptomatic severe MR with normal LV fn(EF >60% AND ESD<40 mm) if MV repair likely to be successful New onset AF,PAH(PASP >50 mmHg at rest or >60 mmHg with exercise) – Symptomatic severe MR with severe LVD,if MV repair likely Class II b – c/c severe MR secondary to severe LVD,persistent symptoms despite optimal therapy for heart failure
 if MV repair likely to be successful New onset AF,PAH(PASP >50 mmHg at rest or >60 mmHg with exercise) – Symptomatic severe MR with severe LVD,if MV repair likely Class II b – c/c severe MR secondary to severe LVD,persistent symptoms despite optimal therapy for heart failure")
67
Tricuspid valve disease Severe TR –poor long term outcome due to RV dysfunction&systemic venous congestion Management strategy depends on clinical status and cause of tricuspid valve abnormality TR a/w dilatation of tricuspid annulus should be repaired – Tricuspid dilatation is an ongoing process – Annuloplasty improves functional status independent of degree of TR

68
Tricuspid valve and chordal reconstruction can be attempted in some cases(endocarditis,trauma) TVR- when leaflets themselves are diseased,abnormal or destroyed-bioprosthesis preferred TR should be addressed along with left sided valve surgery when annulus is dilated >70 mm peroperatively or >3.5 cm in TTE(Bianchi et al,2009)
 TVR- when leaflets themselves are diseased,abnormal or destroyed-bioprosthesis preferred TR should be addressed along with left sided valve surgery when annulus is dilated >70 mm peroperatively or >3.5 cm in TTE(Bianchi et al,2009)")
69
Indications for tricuspid valve surgery Class I – Tricuspid valve repair for severe TR in patients with mitral valve d/s requiring mitral valve surgery Class II a – TVR or annuloplasty for severe primary TR when symptomatic – TVR for severe TR when not amenable to repair or annuloplasty Class II b – Tricuspid annuloplasty for less than severe TR in patients undergoing mitral valve surgery when there is pulmonary hypertension or annular dilatation

70
Pulmonary stenosis NHCHD study 564 pts – Medical management-46%(mild or moderate) Pressure gradients stable in majority 14% had significant increase of gradient – <2 years – PSG>40 mmHg 4% chance of increase gradients in other pts – surgery moderate to severe disease gradient decreased to insignificant levels in 90% No recurrence in follow up 14 yrs – 22 yr follow up of same cohort(1993) Pts with initial gradient <25 had 96% event free survival
 Pressure gradients stable in majority 14% had significant increase of gradient – <2 years – PSG>40 mmHg 4% chance of increase gradients in other pts – surgery moderate to severe disease gradient decreased to insignificant levels in 90% No recurrence in follow up 14 yrs – 22 yr follow up of same cohort(1993) Pts with initial gradient <25 had 96% event free survival")
71
Recommendations Class I – BPV recommended for symptomatic pt(exertional dyspnoea,angina,syncope,presyncope)with PSG>30 mmHg – Asymptomatic patient with PSG>40 mmHg Class II b – Asymptomatic patient with PSG>30-39 mmHg
with PSG>30 mmHg – Asymptomatic patient with PSG>40 mmHg Class II b – Asymptomatic patient with PSG>30-39 mmHg")
72
Long term follow up of BPV similar to surgery with no recurrence –(10 yr follow up,Mc Crindle et al,circulation 1994 ) Surgery still required for dysplastic pulmonary valve
 Surgery still required for dysplastic pulmonary valve")
73
Pulmonary regurgitation Consequence of BPV or surgical valvotomy or TOF repair RV systolic dysfunction-9% Pulmonary valve replacement indicated in symptomatic patients(class III or IV) with severe PR Asymptomatic patients-before RV function deteriorates
 with severe PR Asymptomatic patients-before RV function deteriorates")
74
THANK YOU

Similar presentations





















 CPP = aortic diastolic.>")







 Assistant Professor of Medicine Medical Unit-4 LUMHS, Jamshoro.>")

 F.R.C.P.(E) F.R.C.P.(LONDON) F.A.C.C. DESIGNED AT A.V. DEPTT F.J.M.C. BY RABIA KAZMI.>")