Download presentation
Presentation is loading. Please wait.

1
Morning Report: Friday, February 3 rd

3
Neonatal seizures (NS) result from a rapid depolarization of brain cells excessive synchronous electrical activity Brain cells of newborns are immature and vulnerable to insults Therefore, neonatal seizures often indicate an underlying neurologic disturbance REQUIRE IMMEDIATE ASSESSMENT TO DETERMINE THE UNDERLYING CAUSE AND NECESSARY INTERVENTIONS!!!
 result from a rapid depolarization of brain cells excessive synchronous electrical activity Brain cells of newborns are immature and vulnerable to insults Therefore, neonatal seizures often indicate an underlying neurologic disturbance REQUIRE IMMEDIATE ASSESSMENT TO DETERMINE THE UNDERLYING CAUSE AND NECESSARY INTERVENTIONS!!!")
4
Incidence varies widely Gestational age Weight Cause of NS Some statistics: Preterm infants <1,500g: 19-57.5/1000 live births Preterm/ term infants >2,500g: 2.8/1000 live births

5
Hypoxic-ischemic encephalopathy Intracranial infections Intracranial hemorrhage Non-accidental trauma Cortical (structural) brain malformations Metabolic derangements Inborn errors of metabolism Genetic epileptic syndromes
 brain malformations Metabolic derangements Inborn errors of metabolism Genetic epileptic syndromes")
6
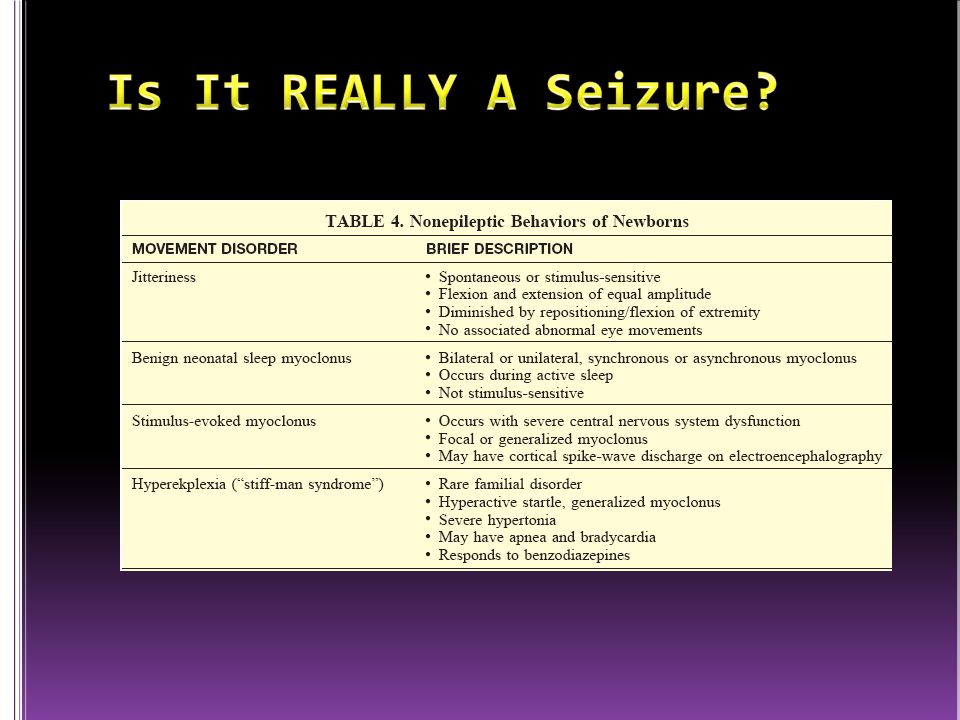
A term 3500g male infant is admitted to the NICU after precipitous vaginal delivery in the ED to a G3 4 P4 24 yo mother without PNC. On PE, the infant has normal VS, a HC of 35.5cm, and normal general examination findings. 12h after birth, the nurse notes brief jerking in one of the infant’s arms. Thirty minutes later, the other arm jerks, and the nurse places a hand on the arm, noting the jerking is not suppressible. Of the following, the most likely cause of the jerking is: A. Benign neonatal myoclonus B. Jitteriness due to drug withdrawl C. Seizure due to CMV infection D. Seizure due to hypocalcemia E. Seizure due to hypoxic-ischemic injury

7
Most common cause of NS 50-60% of cases *Seizures usually occur within the first 24h after birth Severity can increase with time *Majority of full term newborn with NS secondary to asphyxia do NOT manifest long-term neurodevelopmental sequelae

8
Account for 10-20% of NS Most common cause in developing countries Seizures usually begin during the end of the first week of life Pathogens Bacteria Listeria GBS E.Coli Viruses HSV CMV Rubella

9
Accounts for ~10% of NS cases Preterm infants Intraventricular hemorrhage Grade I-II usually asymptomatic Grade III-IV symptomatic Seizures focal and persistant Term infants Subarachnoid hemorrhage Most common type of ICH Birth trauma

10
Term infants Subarachnoid hemorrhage (con’t) Not associated with long-term neurologic sequelae Subdural hemorrhage Birth trauma Consider NAT in an infant who has been d/ed from the hospital
 Not associated with long-term neurologic sequelae Subdural hemorrhage Birth trauma Consider NAT in an infant who has been d/ed from the hospital")
11
Intraventricular hemorrhage Subdural Hemorrhage

12
Subarachnoid Hemorrhage

13
Seizures with variable onset Dysmorphic features, microcephaly or cutaneous lesions may suggest this diagnosis

14
Electrolyte abnormalities Hypoglycemia Hypocalemia Hyper or hyponatremia At risk patients: IDM (hypoglycemia and hypocalcemia) Preterm infants SGA infants
 Preterm infants SGA infants")
15
Aminoacidopathies (PKU, MSUD) Urea cycle defects (OTC deficiency) Mitochondrial disorders Beta-oxidation defects (MCAD, LCAD) Pyridoxine dependency
 Urea cycle defects (OTC deficiency) Mitochondrial disorders Beta-oxidation defects (MCAD, LCAD) Pyridoxine dependency")
16
Benign familial neonatal convulsions May occur 15-20 times per day Outgrown by 1 yo “Fifth day fits” Observed in term infants during the first postnatal week Resolve within 24h Ohtahara syndrome (early infantile epileptic encephalopathy ?Due to malformations in cortical development Brief, repetitive tonic spasms Progressive neurologic deterioration and poor prognosis

18
You are called to the nursery to evaluate a 12h old infant for episodes of jerking. She had been born following a term pregnancy. Vaginal birth was attempted after a prior C/S. Fetal monitoring had shown an apparently reassuring HR and normal status PTD. After replacing the monitor following transport from the labor room to the delivery room, the tracing indicated an abrupt decrease in HR. A stat C/S revealed that the uterus had ruptured and the infant was out of the uterus and in the abdominal cavity. The baby required intubation and chest compressions (no epi). Apgars were 1, 1 and 5 at 1, 5, and 10 mins. You question the parents and nurse about any possible seizures. Of the following, the description that MOST likely indicates that the child is having a NS is: A. Episodes of apnea and bradycardia B. Fatiguing and vomiting during feeds C. Focal jerking in both arms simultaneously but asynchronously D. Limb jerking triggered by touching the child E. Spontaneous limb jerking that stops when a hand is placed on the child
. Apgars were 1, 1 and 5 at 1, 5, and 10 mins. You question the parents and nurse about any possible seizures. Of the following, the description that MOST likely indicates that the child is having a NS is: A. Episodes of apnea and bradycardia B. Fatiguing and vomiting during feeds C. Focal jerking in both arms simultaneously but asynchronously D. Limb jerking triggered by touching the child E. Spontaneous limb jerking that stops when a hand is placed on the child.")
19
Preterm Infants Roving eyes Sustained eye opening or fixation Bicycling Lip smacking Unresponsiveness Term infants Sustained tonic horizontal eye deviation +/- Jerking +/- Apnea

22
Top priority is identifying an underlying etiology NEONATAL SEIZURES ARE VERY RARELY IDIOPATHIC!! Detailed history and PE Maternal RF Complications of pregnancy, labor and delivery

23
Screening labs Acucheck Electrolytes Ammonia Blood gas LP Additional studies Neuroimaging Serum AA, lactate, UOA Viral titers Karyotype Tox screen

24
Due to the immature myelination of the neuronal network Some behavioral or motor manifestations of NS may not be detected on surface EEG Surface EEG findings may be present when there are no observable clinical manifestations

25
ABCs!! Treat underlying problem Treat seizures

26
A term infant is delivered via emergency C/S following the acute onset of maternal vaginal bleeding and profound fetal bradycardia. Apgars are 1, 2, and 3 at 1, 5, and 10 minutes, respectively. Resuscitation includes intubation and assisted ventilation, chest compressions, and IV epi. The infant is admitted to the NICU and has seizures at 6h of life. Of the following, a TRUE statement about infants who have seizures following perinatal asphyxia is that most: A. Develop epilepsy B. Develop microcephaly C. Do not have long-term neurodevelopmental delay D. Experience hearing loss E. Require multiple anticonvulsant medications

27
Cause is the MOST important factor that determines the outcome of NS Patients with self-resolving conditions (i.e.: “fifth day fits”) do well Patients with underlying brain disorders are more likely to have long-term sequelae Other factors that affect prognosis: Gestational age and BW 60% of term infants >25oog with NS were later found to be developmentally normal 20% of preterm infants <1500g with NS were found to be normal
 do well Patients with underlying brain disorders are more likely to have long-term sequelae Other factors that affect prognosis: Gestational age and BW 60% of term infants >25oog with NS were later found to be developmentally normal 20% of preterm infants <1500g with NS were found to be normal")
28
Other factors that affect prognosis (con’t) Apgar scores Need for mechanical ventilation Neurologic findings Findings on EEG and U/S Overall, high incidence of: Early death (24 to 30 percent) Neurologic impairments (20 to 60 percent) Developmental delay (up to 55 percent) Postneonatal epilepsy (20 to 30 percent)
 Apgar scores Need for mechanical ventilation Neurologic findings Findings on EEG and U/S Overall, high incidence of: Early death (24 to 30 percent) Neurologic impairments (20 to 60 percent) Developmental delay (up to 55 percent) Postneonatal epilepsy (20 to 30 percent)")
29
Noon Conference: Asthma: Part Deux, Dr. Roy

Similar presentations







.>")













