Download presentation
Presentation is loading. Please wait.

1
An audit of Endometrial Pathology cases referred to NGOC Dr Paul Cross Consultant Cellular Pathologist Queen Elizabeth Hospital Gateshead

2
Background Endometrial cancer is one of the commonest female malignancies, and is on the increase In the North of England Cancer guidelines, it outlines that for the northern part of the region: –All cases of suspected or proven endometrial cancer should be discussed at the NGOC MDT (based at the QEH Gateshead) –Cases of Grade 1 or 2 endometrial cancer can be treated at Cancer Units –Cases of Grade 3 of special type (i.e. High grade serous, clear cell, carcinosarcoma) should be treated at the NGOC Cancer centre
 should be treated at the NGOC Cancer centre.")
3
WRCFI 2008

4
MDT review basis As far as is known all cases of suspected/proven endometrial malignancy are referred to the NGOC for MDT discussion Most cases are routinely reviewed by an NGOC Pathologist for NGOC MDT discussion Cases from South Tyneside, Durham Sunderland, Northumbria, QEH are routinely reviewed. Cases from Newcastle and Carlisle are reviewed if required (but are always shown by a base pathologist via a TC link for the NGOC MDT discussion)
.")
5
Study - 1 It appeared that at MDT review/discussion some cases had the original diagnosis amended, sometimes significantly in that it would affect patient management The purpose of the audit was to review all cases referred to the NGOC MDT for discussion of possible/proven endometrial cancer in 2010

6
Study - 2 All cases referred to the NGOC MDT (GYREF) for the calendar year 2010 were identified from the QEH Pathology laboratory computer All such cases were then ordered by SNOMED code for endometrial pathology Cases of non-epithelial uterine malignancy (e.g. Endometrial stromal tumour) were excluded
 were excluded.")
7
Results - 1 In 2010, 506 cases were referred for central pathology review for the NGOC MDT Of these 206 (40.7%) were cases of suspected/proven endometrial cancer Of these 206, 121 related to biopsies classed as complex atypical hyperplasia (CAH) or worse (23.9% overall, and 58.7% of endometrial cases overall)
 were cases of suspected/proven endometrial cancer Of these 206, 121 related to biopsies classed as complex atypical hyperplasia (CAH) or worse (23.9% overall, and 58.7% of endometrial cases overall)")
8
Review vs original biopsy diagnosis (n=121)CAHCAH?G1G1G2G3SPECIAL TYPE CAH (n=28) 127441 (HG SEROUS) CAH?G1 (n=19) 10621 (HG SEROUS) G1 (n=30) 2721 (HG SEROUS) G2 (n=20) 182 (HG SEROUS X2) G3 (=11) 101 (CLEAR CELL) SPECIAL TYPE (n=13) 13 (HG SEROUS 6, CARCINOSA RCOMA 4, CLEAR CELL 3)
CAHCAH G1G1G2G3SPECIAL TYPE CAH (n=28) (HG SEROUS) CAH G1 (n=19) (HG SEROUS) G1 (n=30) 2721 (HG SEROUS) G2 (n=20) 182 (HG SEROUS X2) G3 (=11) 101 (CLEAR CELL) SPECIAL TYPE (n=13) 13 (HG SEROUS 6, CARCINOSA RCOMA 4, CLEAR CELL 3)")
9
Outcome where known on hysterectomy vs biopsy review diagnosis (n=90)CAHG1G2G3SPECIAL TYPE CAH (n=4) 31 G1 (n=43) 3652 G2 (n=20) 21611 (HG SEROUS) G3 (n=14) 113 (CARCINO SACRCOM A 3) SPECIAL TYPE (n=9) 9 (HG SEROUS 6, CLEAR CELL 3)
CAHG1G2G3SPECIAL TYPE CAH (n=4) 31 G1 (n=43) 3652 G2 (n=20) (HG SEROUS) G3 (n=14) 113 (CARCINO SACRCOM A 3) SPECIAL TYPE (n=9) 9 (HG SEROUS 6, CLEAR CELL 3)")
10
Results Of the 121 original biopsies, on review 91 (75.2%) were fully agreed with Two main areas of disagreement on review were: –i) identification of special type (esp HG serous) carcinoma (6 cases uplifted, 5 HG serous)(5% overall) –ii) confident separation of CAH from grade 1 (or worse) endometrial cancer (of 28 cases originally diagnosed as CAH, 11 were uplifted to G1 or G2, and 5 to G3 or special type. Of the 19 CAH?G1 group, 8 were uplifted to G1 or G2, and 1 to special type (HG serous) (42.5% of these two groups overall)
 (42.5% of these two groups overall).")
11
WHO classification – a problem? Endometrial hyperplasia –Hyperplasia (typical) Simple hyperplasia without atypia Complex hyperplasia without atypia (adenomatous without atypia) –Atypical Hyperplasia Simple complex hyperplasia (rare) Complex atypical hyperplasia (adenomatous with atypia) “Atypia” refers to cytological atypia
 Simple hyperplasia without atypia Complex hyperplasia without atypia (adenomatous without atypia) –Atypical Hyperplasia Simple complex hyperplasia (rare) Complex atypical hyperplasia (adenomatous with atypia) Atypia refers to cytological atypia.")
12
Why does it matter? CAH, G1 or G2 tumours are typically treated with a simple hysterectomy G3 or special type typically would require hysterectomy, nodal sampling and may require other omental/peritoneal biopsies Washings taken in all cases, but do not affect FIGO staging (under FIGO 2009) Understaging (if it can be avoided) may mean a second surgery for the woman
 Understaging (if it can be avoided) may mean a second surgery for the woman.")
13
CAH vs G1 endometrial cancer Features favouring endometrial G1 cancer are: –Complex back-to-back glands with scanty intervening stroma –Cribriform glands/complex meandering lumina –Intra-glandular bridging –Complex/multi-layered/papillary epithelial projections –Solid non-squamous non-morular areas –Necrosis (glandular +/- stroma) –Bizarre nuclei –Foamy stromal macrophage groups –Often little/no normal endometrium –Invasion (seldom seen!) –High grade features (true clear cell areas, HG serous features, CS )
 –Bizarre nuclei –Foamy stromal macrophage groups –Often little/no normal endometrium –Invasion (seldom seen!) –High grade features (true clear cell areas, HG serous features, CS )")
14
Back - to - back glands

15
Cribriform glands

16
necrosis

17
Solid areas

18
Foamy macrophages

19
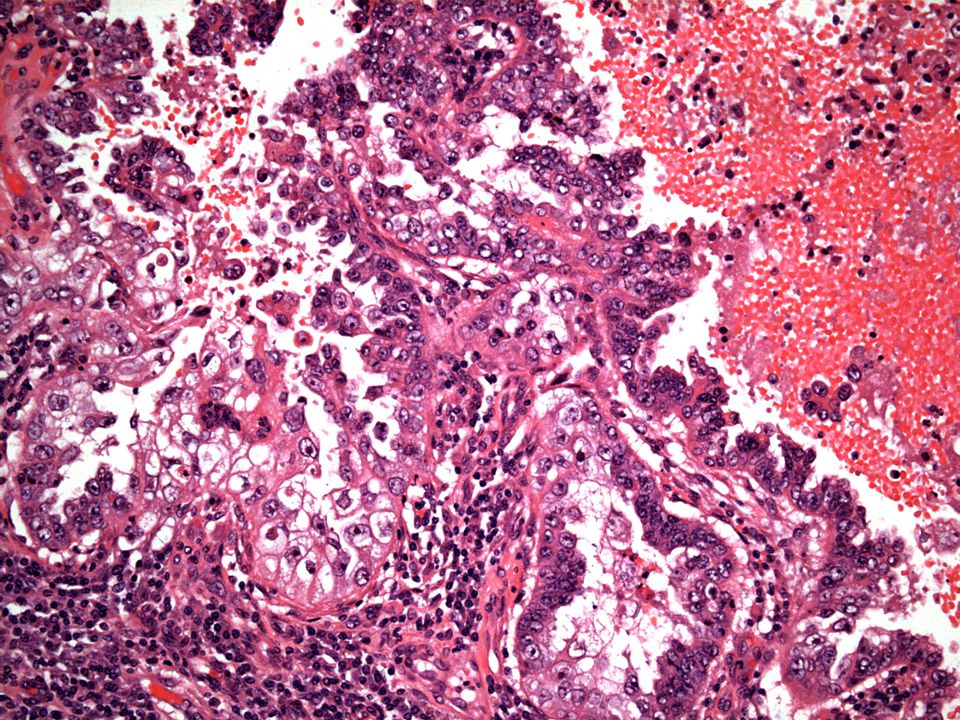
HG endometrial cancer Main types HG serous, clear cell and carcinosarcoma This audit highlights HG serous as an issue Features of HG serous are –Marked cytological atypia of cells on surface of papillary projections –Papillary areas with slit-like spaces –Tufting/stratification of cells –Secondary papillary projections/bridging between papillae –May have psammoma bodies (not diagnostic, but found in ~30- 50% of cases) –may be seen as an “in situ” change not associated with invasion
 –may be seen as an in situ change not associated with invasion")
22
What does this audit highlight? Endometrial pathology is common, and getting more so Diagnosis of hyperplasia is problematic, but neoplasia can (in many cases) be confidently separated from hyperplasia Features of special types (esp HG serous) must not be overlooked Features which may help in diagnosis of these two areas can be re-iterated to help in diagnosis Intend to re-audit in future to assess any future trends
 be confidently separated from hyperplasia Features of special types (esp HG serous) must not be overlooked Features which may help in diagnosis of these two areas can be re-iterated to help in diagnosis Intend to re-audit in future to assess any future trends.")
Similar presentations








 Richard Middleton (Data Manager)>")









>")
>")

