Download presentation
Presentation is loading. Please wait.

1
Malignant Breast Disease
Juhi Asad, DO Alison Estrabrook, MD Dept. of Breast Surgery

2
Breast Cancer Over 180,000 new cases ~62,000 are in situ (30%)
2nd leading cause of all cancer deaths 80% of cases occur >50yo In situ cases have stablized since late 1990s due to early detection~40,000 deaths will occur due to breast cancer in 2007

3
Pre-op History Physical Imaging Diagnosis Treatment options

4
Surgical Options Partial Mastectomy (lumpectomy) Total Mastectomy
Reconstruction Sentinel lymph node biopsy Axillary lymph node dissection

5
Surgical Treatment Partial Mastectomy Radiation therapy Free margins
Aesthetic results NSABP B-06 no significant difference in survival between MRM, lump w/radiaton, and lump w/o radiation

8
Partial Mastectomy Contraindications Size relative to breast
Multifocality Early pregnancy Inability to receive radiation Connective tissue disease Prior radiation

9
Surgical Treatment Radial Mastectomy Historical – mid 70s
Breast, pectoralis, regional lymph nodes along axillary vein to costoclavicular ligament

10
Surgical Treatment Total Mastectomy axillary dissection
TM + Skin sparing w/reconstruction

11
Reconstruction Implants Flaps TRAM Latissimus DIEP

12
Tissue Expanders

13
TRAM

15
Oncoplastic Surgery

19
Preop Days Postop

20
Surgical Treatment Sentinel Node Biopsy
The 1st node in the ipsilateral axilla to drain the tumor >97% concordance rate

21
Sentinel Lymph Node Contraindications Clinically positive lymph nodes

22
Sentinel Lymph Node Technetium-99m sulfur colloid Isosulfan blue dye
Intradermal : peritumoral or periareolar Isosulfan blue dye Intraparenchymal Problems: Anaphylactic reaction (1-3%) Skin discoloration Contraindicated in pregnancy
 Skin discoloration. Contraindicated in pregnancy.")
24
Sentinel Lymph Node Intra-op evaluation
Frozen section Touch prep Benefits over axillary node dissection more accurate pathology less lymphedema – ( very rare vs 10-50%) less sensory disturbances less shoulder dysfunction less wound infection less incisional pain
 less sensory disturbances. less shoulder dysfunction. less wound infection. less incisional pain.")
25
Axillary Lymph Node Dissection
Indications Clinically + nodes + SLN Level I & II

27
Pathology DCIS Invasive Ductal Invasive Lobular

28
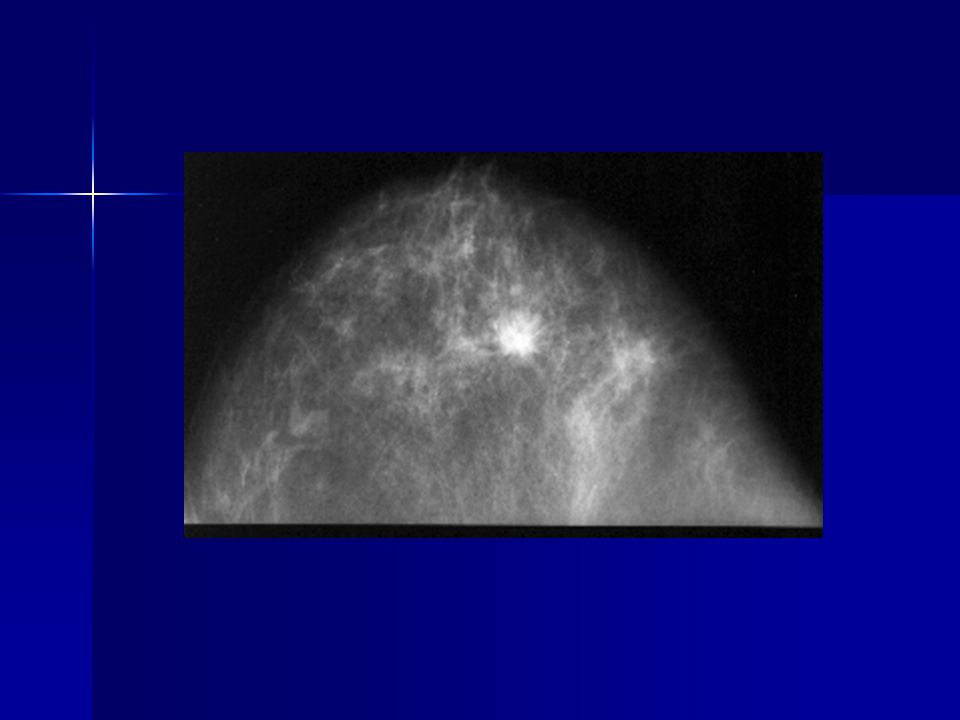
DCIS 200% b/w 1983-1992 15-30% all screen-detected tumors Diagnosis
Screening mammogram Microcalcifications Linear, heterogenous Biopsy Stereotactic Open biopsy

31
DCIS Treatment Partial Mastectomy Total mastectomy
Followed by radiation +/- hormonal therapy Total mastectomy Diffuse disease Multifocal Persistent positive margins Inability to give radiation Patient choice

32
DCIS Sentinel Lymph Node Biopsy Total Mastectomy Palpable mass
Microinvasion

33
DCIS Radiation Therapy Hormonal Therapy 50% decrease in recurrence LE
NSABP B-24 – LE, RT, +TAM vs LE, RT only TAM – 8.2% incidence of IBTR Placebo – 13.4% incidence of IBTR

34
Invasive Ductal Ca Most common – 50-70% of invasive ca

36
Invasive Lobular Ca 10-15% of breast ca Fail to form masses
Multifocal and multicentric Bilateral – 20-29%

37
ILC

38
Staging Primary Tumor (T) TX: unable to assess
T0: no evidence of primary tumor Tis: DCIS, LCIS or Paget’s (nipple only) T1: <2cm T2: 2cm-5cm T3: >5cm T4: extension
 T1: <2cm. T2: 2cm-5cm. T3: >5cm. T4: extension.")
39
Regional Lymph Nodes (N)
NX: unable to assess N0: negative N1: 1-3 nodes N2: 4-9 nodes N3: >10 nodes

40
Distant metastatsis: (M)
MX: unable to assess M0: negative M1: distant mets

41
AJCC Staging Stage 0 Stage I Stage IIA Stage IIB Stage IIIA Stage IIIB
Tis, N0, M0 Stage I T1*, N0, M0 Stage IIA T0, N1, M0 T1*, N1, M0 T2, N0, M0 Stage IIB T2, N1, M0 T3, N0, M0 Stage IIIA T0, N2, M0 T1*, N2, M0 T2, N2, M0 T3, N1, M0 T3, N2, M0 Stage IIIB T4, N0, M0 T4, N1, M0 T4, N2, M0 Stage IIIC** Any T, N3, M0 Stage IV Any T, Any N, M1 [Note: T1 includes T1mic]

42
5 year Survival Stage 5-year Relative Survival Rate 100% I IIA 92% IIB
100% I IIA 92% IIB 81% IIIA 67% IIIB 54% IV 20%

43
Adjuvant Therapy www.adjuvantonline.com
Assess the risks and benefits of additional therapy after surgery

44
Prognostic Indicators
Hormone Receptors – improved prognosis ER – 70-80% PR – indicator for a functional ER receptor Epidermal growth factor HER/erbB2 EGFR HER2/neu Cell proliferation & differentiation erbB2

45
Prognostic Indicators
P53 – tumor suppressor gene Overexpression of p53 Poorer prognosis Shorter disease-free and survival

46
Oncotype Dx ER (+); node (-) Genetic profile – 21 gene assay
Recurrence score (3 groups) Low – hormonal therapy Intermediate – TailorRx trial Hormonal vs chemo + hormonal High – chemo + hormonal therapy
 Low – hormonal therapy. Intermediate – TailorRx trial. Hormonal vs chemo + hormonal. High – chemo + hormonal therapy.")
47
Adjuvant Therapy Hormonal therapy Antiestrogen therapy – Tamoxifen
Pre & post-menopausal women Reduces risk of contralateral disease & mets Side effects Endometrial ca Thromoembolic events

48
Adjuvant Therapy Hormonal Therapy
Aromastase Inhibitors – blocks the conversion of androstenedione to estrone Post-menopausal women ATAC trial – anastrozole decreased the risk of contralateral cancers compared to TAM Side effects Bone loss and joint pain

49
Adjuvant Therapy Chemotherapy Size of tumor Nodal status ER/PR
HER2/Neu -- Herceptin

50
Node (-) & ER/PR (+) & T<1cm & HER2 (-) & no LVI
Low Risk Node (-) & ER/PR (+) & T<1cm & HER2 (-) & no LVI -- Hormonal therapy -- consider Oncotype Intermediate Risk Node (-) & at least 1 of the following T>2cm grade II/III LVI <35 yo HER2 (+) Node + (1-3) & HER2 (-) ER/PR (+) -- OncotypeDX -- hormonal therapy -- Chemo & hormonal therapy ER/PR (-) -- Chemo High Risk Node + (1-3) & HER2 + Node +(>4) -- Chemo & hormone
 & ER/PR (+) & T<1cm & HER2 (-) & no LVI. -- Hormonal therapy. -- consider Oncotype. Intermediate Risk. Node (-) & at least 1 of the following. T>2cm. grade II/III. LVI. <35 yo. HER2 (+) Node + (1-3) & HER2 (-) ER/PR (+) -- OncotypeDX. -- hormonal therapy. -- Chemo & hormonal therapy. ER/PR (-) -- Chemo. High Risk. Node + (1-3) & HER2 + Node +(>4) -- Chemo & hormone.")
51
LCIS Incidental finding Marker for an increased risk
0.8-8% of breast biopsies Marker for an increased risk 1% per year risk Bilateral breasts Most common – Ductal carcinoma

52
LCIS Treatment Annual mammograms 6mos CBE
Discuss bilateral prophylactic mastectomies

54
Paget’s Disease Chronic, eczema-like rash of the nipple and areolar skin ~97% underlying Ca Diagnosis Punch biopsy Core needle biopsy

55
Paget’s Disease Treatment Surgical treatment Adjuvant therapy
TM w/ SLN Central segmentectomy w/ SLN XRT Adjuvant therapy Chemotherapy Hormonal therapy

56
Locally Advanced Disease
Large tumors (>5cm) Chest wall involvment Ulcerations Fixed axillary lymph nodes
 Chest wall involvment. Ulcerations. Fixed axillary lymph nodes.")
57
Locally Advanced Disease

58
Locally Advanced Disease
Treatment Neoadjuvant therapy – 80% shrinkage Downstage BCT vs Mastectomy radiation

59
Post Neoadjuvant therapy

60
Inflammatory Breast Ca
Rare & aggressive Accounts for 5% of all breast ca Younger women higher tendency for distant mets AJCC – T4d Stage IIIB Stage IIIC Stage IV

61
Inflammatory Breast Ca
Presentation Rapid onset of erythema, edema (peau d’orange Often no mass Axillary node involvement Imaging No distinct mass Skin thickening Trabecular thickening

63
Inflammatory Breast Ca
Histology Dermal lymphatic invasion Not associated with a subtype High S-phase fraction Mutation of p53

64
Inflammatory Breast Ca
Survival 3yr – 40-70% 5 yr – 50% 10 yr – 26.7%

65
Male Breast Cancer 1% of all breast ca >90% Ductal Ca ER/PR +
5-10% are hereditary BRCA 2 gene

66
Breast CA during Pregnancy
1 in 3,000 pregnancies Most common non-GYN cancer Present as a painless mass Worse prognosis Advanced stage Stage II-III 75% rate (median 40mos) Hyperestrogenic state
 Hyperestrogenic state.")
67
Breast Ca during Pregnancy
Diagnosis Ultrasound Mammogram Core needle biopsy

68
Breast Ca during Pregnancy
Treatment 1st trimester TM with SLN bx Chemotherapy Significant risk of spontaneous abortion Fetal malformation 2nd & 3rd trimester TM w/ SLN bx or Lumpectomy with SLN bx radiation

69
Question Following an excisional biopsy for microcalifications, the pathology report states there is LCIS present. You discuss with the patient She needs a lumpectomy then RT She would benefit from a mirror biopsy She has a future cancer risk of 1% per yr No known therapy to help her

70
Question 55 yo female underwent a Rt lumpectomy with SLN bx.
Pathology showed a 3.5 cm well-differentiated infiltrating Ductal ca. The sentinel lymph nodes were negative (0/2). No evidence of any distance mets. What is her stage?
. No evidence of any distance mets. What is her stage")
71
40 yo woman presents with a 2cm mass in her right breast first detected by mammo. A core biopsy reveals infiltrating ductal ca. She has no palpable lymph nodes. Appropriate therapy for the patient would include: -- partial mastectomy -- sentinel lymph node biopsy -- consideration of adjuvant chemo -- radiation therapy -- all of the above

Similar presentations