Download presentation
Presentation is loading. Please wait.

1
Early Stage NSCLC: Imprimatur of Adjuvant Therapy
Overview of Recent Data Corey J Langer MD, FACP Professor of Medicine Director of Thoracic Oncology Abramson Cancer Center University of Pennsylvania Philadelphia, PA 19104

2
Disclosures: Past 10 yrs Grant/Research Support: Scientific Advisor:
Bristol Myers Squibb, Pfizer, Imclone, Lilly, Schering-Plough Research Institute, Sanofi-Aventis, Amgen, Cell Therapeutics, OrthoBiotech, Celgene, Vertex, Genentech, OSI, AstraZeneca, Pfizer, Medimmune, GSK Scientific Advisor: Bristol Myers Squibb, Imclone, Sanofi-Aventis, Pfizer, GlaxoSmithKline, Pharmacyclics, Amgen, AstraZeneca, Novartis, Genentech, OSI, Savient, Bayer/Onyx, Abraxis, Clarient, Morphotek, Biodesix, AVEO, Synta Speakers Bureau: curtailed as of 12/10 Bristol Myers Squibb, Imclone, Sanofi-Aventis, Lilly, Genentech, OSI

3
Welcome to Winter in NJ 2-14

4
Stage is Destiny!

5
New Staging System (IASLC ’07) to be instituted 2009
UICC6 T/M Descriptor Proposed T/M N0 N1 N2 N3 T1 (< 2 cm) T1a IA IIA IIIA IIIB T1 (> 2-3 cm) T1b T2 ( 3 to < 5 cm) T2a IB T2 (>5-7) T2b IIB T2 (> 7 cm) T3 T3 invasion T4 (same lobe nodules) T4 (extension) T4 M1 (ipsilateral Lung) T4 (pleural effusion) M1a IV M1 (contralateral lung) M1 (distant) M1b
 T1a. IA. IIA. IIIA. IIIB. T1 (> 2-3 cm) T1b. T2 ( 3 to < 5 cm) T2a. IB. T2 (>5-7) T2b. IIB. T2 (> 7 cm) T3. T3 invasion. T4 (same lobe nodules) T4 (extension) T4. M1 (ipsilateral Lung) T4 (pleural effusion) M1a. IV. M1 (contralateral lung) M1 (distant) M1b.")
6
New Staging System (IASLC ’07) Instituted 2009
UICC6 T/M Descriptor Proposed T/M N0 N1 N2 N3 T1 (< 2 cm) T1a IA IIA IIIA IIIB T1 (> 2-3 cm) T1b T2 ( 3 to < 5 cm) T2a IB T2 (>5-7) T2b IIB T2 (> 7 cm) T3 T3 invasion T4 (same lobe nodules) T4 (extension) T4 M1 (ipsilateral Lung) T4 (pleural effusion) M1a IV M1 (contralateral lung) M1 (distant) M1b
 T1a. IA. IIA. IIIA. IIIB. T1 (> 2-3 cm) T1b. T2 ( 3 to < 5 cm) T2a. IB. T2 (>5-7) T2b. IIB. T2 (> 7 cm) T3. T3 invasion. T4 (same lobe nodules) T4 (extension) T4. M1 (ipsilateral Lung) T4 (pleural effusion) M1a. IV. M1 (contralateral lung) M1 (distant) M1b.")
7
Limitations of Earlier Adjuvant Trials
Use of regimens with marginal activity in advanced NSCLC Inclusion of patients with compromised PS and multiple co-morbidities Difficulty administering systemic therapy in the post-op setting Inadequate power or overly ambitious survival endpoints

8
Adjuvant Cisplatin Trials n=1394
1995 Meta-Analysis Adjuvant Cisplatin Trials n=1394 100 HR 0.87 p=0.08 80 60 Percentage Survival 40 Surgery plus Chemotherapy Surgery 20 12 18 24 36 48 54 60 Time from Randomization (months) 5% absolute survival benefit at 5 years, NS BMJ 31: , 1995
 5% absolute survival benefit at 5 years, NS. BMJ 31: ,")
9
Plaitnum-Based Adjuvant Trials in Resected NSCLC
N. of Patients HR (95%CI) BMJ meta 1394 0.87 ( ) IALT 1867 0.86 ( ) ALPI 1209 0.96 ( ) E3590 488 0.93 ( ) BLT 381 1.02 ( ) BR-10 482 0.70 ( ) CALGB9633 344 0.63 ( ) ANITA 840 0.79 ( ) LACE meta 4584 0.89 ( ) NEJM 00; JNCI 03; EuroJTS 04, NEJM 04; NEJM 05; ASCO 04+06; Lancet Oncology 06
 BMJ meta ( ) IALT ( ) ALPI ( ) E ( ) BLT ( ) BR ( ) CALGB ( ) ANITA ( ) LACE meta ( ) NEJM 00; JNCI 03; EuroJTS 04, NEJM 04; NEJM 05; ASCO 04+06; Lancet Oncology 06.")
10
Plaitnum-Based Adjuvant Trials in Resected NSCLC: Longterm Results
N. of Patients HR (95%CI) BMJ meta 1394 0.87 ( ) IALT 1867 0.91 ( ) ALPI 1209 0.96 ( ) E3590 488 0.93 ( ) BLT 381 1.02 ( ) BR-10 482 0.70 ( ) CALGB9633 344 0.80 ( ) ANITA 840 0.79 ( ) LACE meta 4584 0.89 ( ) NEJM 00; JNCI 03; EuroJTS 04, NEJM 04; NEJM 05; ASCO 04+06; Lancet Oncology 06
 BMJ meta ( ) IALT ( ) ALPI ( ) E ( ) BLT ( ) BR ( ) CALGB ( ) ANITA ( ) LACE meta ( ) NEJM 00; JNCI 03; EuroJTS 04, NEJM 04; NEJM 05; ASCO 04+06; Lancet Oncology 06.")
11
Intl Adjuvant Lung Cancer Trial (IALT) 1867 pts, I-III
Randomized to obs vs. 4 cycles post-op chemo* Radiation therapy optional (~30%) 4.1% absolute benefit at 5 years, p<0.03† Stage III > Stage I benefit Diminished at 7 yr follow-up HR 0.86 [ ] 0.91 [ ]; p = 0.04 0.1 after 5 yrs due to non-cancer deaths ^ *cisplatin + etoposide or vinca alkaloid †Arriagado, NEJM 350:351, 2004, ^ Le Chevalier ASCO 2008
 4.1% absolute benefit at 5 years, p<0.03† Stage III > Stage I benefit. Diminished at 7 yr follow-up. HR 0.86 [ ] 0.91 [ ]; p = 0.04 0.1 after 5 yrs due to non-cancer deaths ^ *cisplatin + etoposide or vinca alkaloid. †Arriagado, NEJM 350:351, 2004, ^ Le Chevalier ASCO")
12
Randomized International Adjuvant Lung Cancer Trial (IALT): Cisplatin-Based Chemotherapy vs No Chemotherapy for Resected NSCLC Arm A* Cisplatin 80 mg/m2 4 cycles OR Cisplatin 100 mg/m2 3-4 cycles OR Cisplatin 120 mg/m2 3 cycles PLUS Etoposide 100 mg/m2 3 days/cycle OR Vinorelbine 30 mg/m2 weekly OR Vinblastine 4 mg/m2 weekly OR Vindesine 3 mg/m2 weekly n=935 RANDOMIZE Stage I-III NSCLC Complete surgical resection within 60 days N=1867 Arm B Observation ± thoracic radiotherapy 60 Gy† n=932 *Each center selected which chemotherapy it would use. †Optional, but predefined by N stage at each center. Le Chevalier et al. Proc Am Soc Clin Oncol. 2003;22:2. Abstract and oral presentation; Arriagada et al. N Engl J Med. 2004;350:351.

13
Adjuvant Chemotherapy IALT n=1867
cDDP was 80 q 3 weeks X 4 100 q 4 weeks X 3-4 120 q 4 weeks X 3 56% + Etoposide 100 27% + Vinorelbine 30 11% + Vinblastine 4 6% + Vindesine 3 Le Chevalier, ASCO 2003 abstract 6, NEJM 2004

14
Adjuvant Chemotherapy IALT (International Adjuvant Lung Trial) n=1867
33 countries, initial accrual goal was 3300 80/20 M/F Mean age 59 (all < 75) Squamous 47%, ACAs 40% Chemo to start < 60 days after surgery Median f/u: 56 months Le Chevalier, ASCO 2003 abstract 6, NEJM 1/04
 Squamous 47%, ACAs 40% Chemo to start < 60 days after surgery. Median f/u: 56 months. Le Chevalier, ASCO 2003 abstract 6, NEJM 1/04.")
15
IALT: Cisplatin-Based Chemotherapy vs No Chemotherapy for Resected NSCLC: Overall Survival (Med F/U 56 mos) 100 HR=0.86 ( ) Chemotherapy 80 Observation ± RT P<0.03 60 % Survival 40 20 12 24 36 48 60 Months Le Chevalier et al. Proc Am Soc Clin Oncol. 2003;22:2. Abstract and oral presentation. NEJM 1/04
 Chemotherapy. 80. Observation ± RT. P< % Survival Months. Le Chevalier et al. Proc Am Soc Clin Oncol. 2003;22:2. Abstract and oral presentation. NEJM 1/04.")
16
IALT Trial ARM Adjuvant chemo Control Number of enrollees 935 932
Dead of disease progression 361 405 Tx-related deaths (n) 14 2 Compliance with RT (%) 71 85 Median DFS (mo) 39.4 34.3 2-yr DFS (%) 61 55 5-yr DFS (%) 39 34 Median Survival Time (mo) 50.8 44.4 2-yr OS (%) 70 67 5-yr OS (%) 44.5 40.4
 Compliance with RT (%) Median DFS (mo) yr DFS (%) yr DFS (%) Median Survival Time (mo) yr OS (%) yr OS (%)")
17
IALT: Cisplatin-Based Chemotherapy vs No Chemotherapy for Resected NSCLC: Overall Survival
Benefit seen across all demographic variables Gender type of surgery use of RT geographical location Greatest benefit in stage III pts (~7.5%) In subgroup analyses, survival advantage for stage I and II was not statistically significant Adj Control Rel %↑ Stage I Stage II Stage III
 In subgroup analyses, survival advantage for stage I and II was not statistically significant. Adj Control Rel %↑ Stage I Stage II Stage III")
18
IALT: Cisplatin + a Vinca or Etoposide 2008 Update: 7
IALT: Cisplatin + a Vinca or Etoposide 2008 Update: 7.5-Year Median Follow-Up 100% chemotherapy: 578 deaths - 495 deaths before 5 years 80% - 83 deaths after 5 years 60% HR: 0.91 ( , P = 0.10) 40% control 590 deaths 20% - 534 deaths before 5 years - 56 deaths after 5 years 0% 1 2 3 4 5 6 7 8 years 935 775 619 520 447 372 282 208 125 932 780 650 550 487 399 300 208 133 Le Chevalier T, et al. J Clin Oncol. 2008(May 20 suppl). Abstract 7507.
 40% control 590 deaths. 20% deaths before 5 years deaths after 5 years. 0% years Le Chevalier T, et al. J Clin Oncol. 2008(May 20 suppl). Abstract")
19
Criticisms of IALT Heterogenous staging, chemo and application of RT (HR favored stage III, not stage I or II) Study actually closed earlier than planned because of emerging interest in neoadjuvant Tx Potential Molecular Imbalances: Results of ERCC1 suggest that one can select a group more likely to benefit; other bio-correlatives still pending Elderly (> 75) excluded; how do we address this expanding cohort? Dissipation of survival benefit after 5 years Why was this trial positive when so many similar trials proved negative?
 excluded; how do we address this expanding cohort Dissipation of survival benefit after 5 years. Why was this trial positive when so many similar trials proved negative")
20
Recent (-) Trials of Adjuvant CT in Completely Resected NSCLC
Study Country CT Regimen # of Patients Outcome on OS INT 0115 ALPI/EORTC BLT USA Italy/Europe International VP16-P x 4 MVP x 3 V-P x 4 462 1197 481 Negative

21
2004: Paradigm Shift

22
Recently Completed (+) Randomized Adjuvant Trials in Early Stage NSCLC
2004: Paradigm Shift Recently Completed (+) Randomized Adjuvant Trials in Early Stage NSCLC Stage No Intervention CALGB 9633 IB Carboplatin/Paclitaxel NCI-C* IB-II Cisplatin/Vinorelbine
 Randomized Adjuvant Trials in Early Stage NSCLC. Stage No. Intervention. CALGB 9633 IB 500 Carboplatin/Paclitaxel. NCI-C* IB-II 480 Cisplatin/Vinorelbine.")
23
Recently Completed (+) Randomized Adjuvant Trials in Early Stage NSCLC
2005: Paradigm Shift Recently Completed (+) Randomized Adjuvant Trials in Early Stage NSCLC Stage No Intervention CALGB 9633 IB Carboplatin/Paclitaxel NCI-C* IB-II Cisplatin/Vinorelbine ANITA I-IIIA Cisplatin/Vinorelbine
 Randomized Adjuvant Trials in Early Stage NSCLC. Stage No. Intervention. CALGB 9633 IB 500 Carboplatin/Paclitaxel. NCI-C* IB-II 480 Cisplatin/Vinorelbine. ANITA I-IIIA 840 Cisplatin/Vinorelbine.")
24
CALGB pts, stage IB 4 cycles carboplatin/paclitaxel vs. observation Radiation therapy not allowed HR 0.62; p = 0.028 HR 0.80; p = 0.10 Strauss Proc ASCO 2004 abs 7019, 2006 abs 7007, JCO 2009

25
CALGB 9633 Overall Survival by Tumor Size
Tumor ≥4 cm Tumor <4 cm Observation Paclitaxel + Carboplatin Observation Paclitaxel + Carboplatin n=74 n=97 n=74 Probability Probability n=99 HR = 0.66; 90% CI, ; P=0.04 HR = 1.02; 90% CI, ; P=0.51 Years Years Strauss Proc ASCO 2004 abs 7019, 2006 abs 7007, JCO 2008

26
JBR.10 N = 240 N = 242 RANDOMI Observation ELIGIBLE:
Z E Observation ELIGIBLE: Resected IB and II T2N0, T1N1, or T2N1 No prior chemo No RT N = 240 Vinorelbine 25 mg/m2 weekly x 16 plus Cisplatin 50 mg/m2 day 1 & 8 q4wk x 4 cycles N = 242 Stratification: Nodal status – N0 vs N1 RAS status Primary endpoint = overall survival Winton T, et al. N Engl J Med. 2005;352: 26 26

27
NCIC-CTG JBR.10 482 pts, stage IB-II
Stage IB-II only 4 cycles of post-op cis/vin vs. observation No radiation therapy 15% survival advantage at 5 years 54% vs 69% alive (NEJM paper) HR 0.69, p=.012 in 482 pts Benefit only in stage II in subset analysis Although post-hoc analysis shows a benefit in IB > 4cm Winton, Proc ASCO 2004 Abs:7018, 2004, NEJM 2005
 HR 0.69, p=.012 in 482 pts. Benefit only in stage II in subset analysis. Although post-hoc analysis shows a benefit in IB > 4cm. Winton, Proc ASCO 2004 Abs:7018, 2004, NEJM")
28
Overall Survival by Treatment Arm
All Patients Fig.1 5 yr: 67% vs 56% MST 94m vs 72m HR 0.69 5 yr: 69% vs 54% MST 94 m vs 73 m Absolute improvement in 5 yr OS = 15% (69% vs 54%) Winton et al. NEJM 2005 Absolute improvement in 5 yr OS = 11% (67% vs 56%); benefit persists at 9+ yrs Vincent, Butts et al, 2009, ASCO -7501
 Winton et al. NEJM Absolute improvement in 5 yr OS = 11% (67% vs 56%); benefit persists at 9+ yrs Vincent, Butts et al, 2009, ASCO")
29
Cumulative Incidence Plots for Disease and Non-disease Related Deaths

30
Stage IB Analysis T < 4 cm T ≥ 4 cm HR OS p CALGB 9633 1.02 .51
0.66 .04 JBR.10 1.73 .07 .13 No Chemo Benefit Potential Chemo Benefit Strauss JCO 2008

31
ANITA - 840 pts, stage IB-IIIA
1:1 Randomization post-resection Vinorelbine (30 mg/m2) Q wk X 16 + Cisplatin 100 mg/m2 Q 4 wks X 4 vs Observation Radiation therapy allowed 8.6% survival advantage at 5 years (persists at 7 yr) 42.6% vs 51.2% alive HR 0.7 [ ], p =.013 Benefit only in stage II and IIIA Douillard Lancet Oncol. 7:719, 2006
 Q wk X 16 + Cisplatin 100 mg/m2 Q 4 wks X 4 vs. Observation. Radiation therapy allowed. 8.6% survival advantage at 5 years (persists at 7 yr) 42.6% vs 51.2% alive. HR 0.7 [ ], p =.013. Benefit only in stage II and IIIA. Douillard Lancet Oncol. 7:719,")
32
840 pts accrued from 12/94 through 12/00 Median F/U > 70 mos
ANITA: Rand Phase III Trial of Vinorelbine and Cisplatin vs Obs in Resected stage I-III NSCLC: Demographics 840 pts accrued from 12/94 through 12/00 Median F/U > 70 mos Each arm well balanced Median age 59 (18 – 75) 86% male 95% PS 0-1 59% Squamous ca 37% pneumonectomy Stage I – 35% II – 30% III – 35% Douillard Lancet Oncol. 7:719, 2006
 86% male. 95% PS % Squamous ca. 37% pneumonectomy. Stage. I – 35% II – 30% III – 35% Douillard Lancet Oncol. 7:719,")
33
Overall survival - ITT population
Abstract #7013: ANITA Trial Overall survival - ITT population OBS. NVB + CDDP Median months 43.8 65.8 P-value 0.013 Hazard Ratio 0.79 [ ] 1.00 0.75 0.50 0.25 Survival Distribution Function Obs NVB + CDDP 20 40 60 80 100 120 months Douillard Lancet Oncol. 7:719, 2006

34
ANITA: Randomized Phase III Trial of Vinorelbine and Cisplatin vs Observation in resected stage I-III NSCLC Arm Observation Adjuvant No 433 407 RFS (mo) 21 36 Median Surv (mo)* 44 66 2 yr OS 63 68 5 yr OS 43 51 7 yr OS 37 48 Stage I 62 Stage II 39 52 Stage III 26 42 * P =0.002, HR 0.76 Douillard Lancet Oncol. 7:719, 2006
 Median Surv (mo)* yr OS yr OS yr OS Stage I. 62. Stage II Stage III * P =0.002, HR Douillard Lancet Oncol. 7:719,")
35
ANITA: Randomized Phase III Trial of Vinorelbine and Cisplatin vs Observation in resected stage I-III NSCLC Arm Observation Adjuvant No 433 407 RFS (mo) 21 36 Median Surv (mo)* 44 66 2 yr OS 63 68 5 yr OS 43 51 7 yr OS 37 48 Stage I 62 Stage II 39 52 Stage III 26 42 * P =0.002, HR 0.76 Douillard Lancet Oncol. 7:719, 2006
 Median Surv (mo)* yr OS yr OS yr OS Stage I. 62. Stage II Stage III * P =0.002, HR Douillard Lancet Oncol. 7:719,")
36
Peripheral Neuropathy 3% Drug-Related Fatality 1%
ANITA: Randomized Phase III Trial of Vinorelbine and Cisplatin vs Obs in resected stage I-III NSCLC Adjuvant Toxicities Neutropenia Gr 3+4 86% Febrile Neutropenia 12.5% Nausea-Vomiting Gr 3+4 27% Aesthenia 28% Constipation 5% Peripheral Neuropathy 3% Drug-Related Fatality 1% Douillard et al ASCO 2005, A-7013, p624

37
LACE:Trials and patients
5 trials including 4,584 patients Median follow-up: 5.1 years (3.1 – 5.9) 80% male Median age 59 years, 9% > 70 years old Pathological Stage: IA: 8%, IB: 30%, II: 35%, III: 27% Surgery: 31% pneumonectomy Histology: 49% squamous cell, 39% adenocarcinoma, 12% other Pignon Proc ASCO 2006 abs 7008
 80% male. Median age 59 years, 9% > 70 years old. Pathological Stage: IA: 8%, IB: 30%, II: 35%, III: 27% Surgery: 31% pneumonectomy. Histology: 49% squamous cell, 39% adenocarcinoma, 12% other. Pignon Proc ASCO 2006 abs")
38
Survival curve

39
CT effect & stage CT may be detrimental for stage IA, but stage IA patients were generally not given the potentially best combination cisplatin+vinorelbine (13% of stage IA patients versus ~43% for other stages)
")
40
CT effect & stage CT may be detrimental for stage IA, but stage IA patients were generally not given the potentially best combination cisplatin+vinorelbine (13% of stage IA patients versus ~43% for other stages)
")
41
Stage-Specific Hazard Ratios Recent Adjuvant Trials
I < 4 cm I > 4 cm II IIIA IALT 0.95 0.93 0.79 BR-10 1.73 0.66 0.59 N/A ANITA 1.10 0.71 0.69 CALGB 1.02 LACE 1.41* 0.91* 0.83 Negative Positive Indeterminate Not studied * 3 cm as cut point

42
Therapeutic Implications
Short course adjuvant, platinum-based therapy has emerged as standard practice in resected stage Ib-IIIa NSCLC Ongoing controversies re: Molecular Selection Influence of Age on Outcome Ideal platinating agent: carbo vs cisplatin Choice of partner agent Impact of Stage Role of targeted agents Utility of RT in IIIA (N2)
")
43
Potential Benefit from Adjuvant Systemic Therapy
100 Patients with residual micrometastases resistant to adjuvant therapy Patients with residual micrometastases sensitive to adjuvant therapy 80 Predictive Markers ? 60 Disease Free Patients (%) 40 20 Patients cured with local regional therapy Prognostic Markers ? 2 4 6 8 10 Years
 Patients cured with local regional therapy. Prognostic Markers Years.")
44
Influence of Age on Outcome

45
Elderly Specific Analyses: BR10 Pepe et al ASCO ’06, A-7009
65: designated cut-off 327 younger pts (68 %) 155 older pts (32 %) Baseline demographics similar except for histology and PS Cohort Younger Older P value Adenoca 58% 43% 0.001 Squamous 32% 59% PS 0 53% 42% 0.01
 155 older pts (32 %) Baseline demographics similar except for histology and PS. Cohort. Younger. Older. P value. Adenoca. 58% 43% Squamous. 32% 59% PS 0. 53% 42%")
46
JBR-10 Outcomes by Age Worse PS in older; fewer PS 0 >65 (53% vs 41%, = 0.01) adeno>squam in younger, squam>adeno in older pts. Patients >65 received significantly less chemo no significant diff. in toxicity, or growth factor support more elderly patients refused treatment OS 46% vs. 66% for obs. vs. chemo in pts >65 Overall Survival HR 0.61 [ ], p =.04 in elderly OS 58% vs. 70% for obs. vs. chemo in pts <65 Overall Survival HR 0.77 [ ], p = 0.14 in young Older patients (>75) Worse survival regardless of Rx, but same when corrected for disease-specific survival Benefit from chemo not seen in pts >75 (?harmful) However, patient numbers are too small to answer clearly Pepe C, et al. Adjuvant vinorelbine and cisplatin in elderly patients: National Cancer Institute of Canada and Intergroup Study JBR.10. J Clin Oncol Apr 20;25(12):
 Worse survival regardless of Rx, but same when corrected for disease-specific survival. Benefit from chemo not seen in pts >75 ( harmful) However, patient numbers are too small to answer clearly. Pepe C, et al. Adjuvant vinorelbine and cisplatin in elderly patients: National Cancer Institute of Canada and Intergroup Study JBR.10. J Clin Oncol Apr 20;25(12):")
47
BR10: Overall Survival by Age Group
1.0 1.0 N = 327 H-R = 2.38 N = 84 0.8 Log-Rank, p = 0.0006 0.8 N = 48 > N = 23 0.6 Probability 0.6 63% 0.4 0.4 75 N = 459 0.2 >75 N = 23 0.2 26% 0.0 0.0 2 4 6 8 10 12 2 4 6 8 10 12 Time (Years) Pepe C, et al Adjuvant vinorelbine and cisplatin in elderly patients: National Cancer Institute of Canada and Intergroup Study JBR.10. J Clin Oncol Apr 20;25(12):
 Pepe C, et al Adjuvant vinorelbine and cisplatin in elderly patients: National Cancer Institute of Canada and Intergroup Study JBR.10. J Clin Oncol Apr 20;25(12):")
48
Ideal Platinating Agent

49
Argument Favoring Carboplatin
The best results obtained in stage IB have been observed with CbPac (not with DDP-based regimens) Subset analysis in > 4 cm tumors demonstrates a survival benefit CbPac has not been tested in stage II/IIIA in the adjuvant setting Absence of data does not prove absence of benefit (….absence of proof is not proof of absence….) Finally, a substantial percentage of adj pts are poor candidates for cisplatin-based therapy due to age, co-morbidities, etc
 Subset analysis in > 4 cm tumors demonstrates a survival benefit. CbPac has not been tested in stage II/IIIA in the adjuvant setting. Absence of data does not prove absence of benefit (….absence of proof is not proof of absence….) Finally, a substantial percentage of adj pts are poor candidates for cisplatin-based therapy due to age, co-morbidities, etc.")
50
Which Agents Partner Best with Platinum

51
Randomized phase 2 Trial on
Refinement of Early stage NSCLC Adjuvant chemotherapy with cisplatin and pemetrexed (CPx) versus cisplatin and vinorelbine (CVb) - TREAT M. Kreuter, J. Vansteenkiste, J. Fischer, W. Eberhardt, H. Zabeck, J. Kollmeier, M. Serke, N. Frickhofen, M. Reck, W. Engel-Riedel, S. Neumann, M. Thomeer, C. Schumann, P. De Leyn, T. Graeter, G. Stamatis, I. Zuna, F. Griesinger and M. Thomas on behalf of the TREAT investigators
 versus cisplatin and vinorelbine (CVb) - TREAT. M. Kreuter, J. Vansteenkiste, J. Fischer, W. Eberhardt, H. Zabeck, J. Kollmeier, M. Serke, N. Frickhofen, M. Reck, W. Engel-Riedel, S. Neumann, M. Thomeer, C. Schumann, P. De Leyn, T. Graeter, G. Stamatis, I. Zuna, F. Griesinger and M. Thomas. on behalf of the TREAT investigators.")
52
Rationale: Dose delivery: Adjuvant CTX
LACE-Metaanalysis NCIC-JBR .10 No treatment 9% 4.5% Treatment incomplete 24 % (≤ 2 cycles) 50% (< 4 cycles) early death or progression 5% toxicity 34% 13% patient refusal 35% 29% Therapy delay 55% Dose reductions 77% TREAT Rationale: Adjuvant CTX: mainly Cisplatin / Vinorelbine Need: reduction of toxicity, improvement of dose delivery & compliance Cisplatin / Pemetrexed in thoracic malignancies: high dose intensity, low toxicities Pignon, JCO, 2008 ; Winton, N Engl J Med, 2005; Alam, Lung Cancer, 2005; Vogelzang, JCO, 2003; Scagliotti, JCO, 2008; Schmid-Bindert, ASCO, 2009
 50% (< 4 cycles) early death or progression. 5% toxicity. 34% 13% patient refusal. 35% 29% Therapy delay. 55% Dose reductions. 77% TREAT Rationale: Adjuvant CTX: mainly Cisplatin / Vinorelbine. Need: reduction of toxicity, improvement of dose delivery & compliance. Cisplatin / Pemetrexed in thoracic malignancies: high dose intensity, low toxicities. Pignon, JCO, 2008 ; Winton, N Engl J Med, 2005; Alam, Lung Cancer, 2005; Vogelzang, JCO, 2003; Scagliotti, JCO, 2008; Schmid-Bindert, ASCO,")
53
TREAT: Design Cisplatin / Vinorelbine (CVrb) R0
Inclusion • NSCLC stages IB, IIA, IIB, T3N1M0 • ≤ 42 Tage postoperatively, R0, systematic LN-dissection • ECOG 0, 1 • amenable to Cisplatin treatment Stratification • Center • Nodal status (N0 versus N1) • Surgical procedure (lobectomy vs pneumonectomy) Cisplatin / Vinorelbine (CVrb) Cisplatin / Pemetrexed (CPx) 50 mg/m2 d1+8 / 25 mg/m2 d1, 8, 15, 22 q d 29 x 4 75 mg/m2 d1 / mg/m2 d1 q d 22 x 4 Winton et al., N Engl J Med (2005) 352: 258 R0
 • Surgical procedure (lobectomy vs pneumonectomy) Cisplatin / Vinorelbine (CVrb) Cisplatin / Pemetrexed (CPx) 50 mg/m2 d1+8 / 25 mg/m2 d1, 8, 15, 22 q d 29 x mg/m2 d1 / 500 mg/m2 d1 q d 22 x 4. Winton et al., N Engl J Med (2005) 352: 258. R0.")
54
TREAT: Conduct / endpoints
Study conduct Study concept 2005, Inclusion 10/ /2009 (16 sites, 132 patients) Treatment until 2/2010, primary endpoint analysis 12/2010 Primary endpoint Clinical Feasibility No death due to cancer, toxicity, comorbidity No Non-acceptance by patients leading to premature withdrawal No observation of DLT Neutropenia grade > 7 d Neutropenia grade 3/ with fever/infection Thrombocytopenia grade > 7 d Thrombocytopenia any grade with bleeding Non-hematologic toxicity grade 3/ related to CTX Secondary endpoints Dose delivery, safety, TTTF, RFS, OS, DMFS, LRFS, site of relapse Kreuter et al., BMC Cancer, 2007
 Treatment until 2/2010, primary endpoint analysis 12/2010. Primary endpoint. Clinical Feasibility. No death due to cancer, toxicity, comorbidity. No Non-acceptance by patients leading to premature withdrawal. No observation of DLT. Neutropenia grade 4 > 7 d. Neutropenia grade 3/4 with fever/infection. Thrombocytopenia grade 4 > 7 d. Thrombocytopenia any grade with bleeding. Non-hematologic toxicity grade 3/4 related to CTX. Secondary endpoints. Dose delivery, safety, TTTF, RFS, OS, DMFS, LRFS, site of relapse. Kreuter et al., BMC Cancer,")
55
TREAT: Conduct / endpoints
Study conduct Study concept 2005, Inclusion 10/ /2009 (16 sites, 132 patients) Treatment until 2/2010, primary endpoint analysis 12/2010 Primary endpoint Clinical Feasibility [considered promising if > 80%] No death due to cancer, toxicity, comorbidity No Non-acceptance by patients leading to premature withdrawal No observation of DLT Neutropenia grade > 7 d Neutropenia grade 3/ with fever/infection Thrombocytopenia grade > 7 d Thrombocytopenia any grade with bleeding Non-hematologic toxicity grade 3/ related to CTX Secondary endpoints Dose delivery, safety, TTTF, RFS, OS, DMFS, LRFS, site of relapse Kreuter et al., BMC Cancer, 2007
 Treatment until 2/2010, primary endpoint analysis 12/2010. Primary endpoint. Clinical Feasibility [considered promising if > 80%] No death due to cancer, toxicity, comorbidity. No Non-acceptance by patients leading to premature withdrawal. No observation of DLT. Neutropenia grade 4 > 7 d. Neutropenia grade 3/4 with fever/infection. Thrombocytopenia grade 4 > 7 d. Thrombocytopenia any grade with bleeding. Non-hematologic toxicity grade 3/4 related to CTX. Secondary endpoints. Dose delivery, safety, TTTF, RFS, OS, DMFS, LRFS, site of relapse. Kreuter et al., BMC Cancer,")
56
TREAT: Characteristics
CPx (n=67) CVb (n=65) Total (n=132) Age (years [range]) 58 [40-73] 60 [38-74] 59 [38-74] Gender (%) male female 72 28 77 23 74 26 Smoking status (%) Smoker Ex-smoker Non-smoker Not available 33 61 6 71 1.5 29 66 4 1 Stage (%) IB 37 38 IIA 12 8 10 IIB 46 48 47 T3N1 5
 CVb. (n=65) Total. (n=132) Age (years [range]) 58 [40-73] 60 [38-74] 59 [38-74] Gender (%) male. female Smoking status (%) Smoker. Ex-smoker. Non-smoker. Not available Stage (%) IB IIA IIB T3N1. 5.")
57
TREAT : Characteristics
CPx (n=67) CVb (n=65) Total (n=132) Surgical procedures (%) Lobectomy 84 82 83 Pneumonectomy 12 15 14 Complex resections 4 3 Histology (%) Squamous cell carcinoma 45 42 43 Non-squamous 55 58 57 Adenocarcinoma 37 44 41 Large cell carcinoma 9 Mixed cell carcinoma 5 7
 CVb. (n=65) Total. (n=132) Surgical procedures (%) Lobectomy Pneumonectomy Complex resections Histology (%) Squamous cell carcinoma Non-squamous Adenocarcinoma Large cell carcinoma. 9. Mixed cell carcinoma")
58
Results: Primary endpoint - feasibility
CPx CVb Feasibility rate (%) 95.5 (CI ) 75.4 (CI ) Death (%) 1.5 3.1 Withdrawal of consent (%) 6.2 DLT (%) 3.0 15.4 Reasons for DLT (events) * patients (n=2) patients (n=10) G4 neutropenia >7d 4 G4 thrombocytopenia >7d G3/4 febrile neutropenia 1 5 Thrombocytopenia with bleeding G3/4 non-hematologic toxicity 2 p = * multiple reasons possible
 (CI ) (CI ) Death (%) Withdrawal of consent (%) 6.2. DLT (%) Reasons for DLT (events) * patients (n=2) patients (n=10) G4 neutropenia >7d. 4. G4 thrombocytopenia >7d. G3/4 febrile neutropenia Thrombocytopenia with bleeding. G3/4 non-hematologic toxicity. 2. p = * multiple reasons possible.")
59
Results: End of therapy
EOT CPx CVb Regular EOT (%) 77.6 36.9 Earlier termination of therapy (%) 22.4 63.1 Reasons for earlier termination (events)* patients (n=15) patients (n=41) Unacceptable toxicity according to protocol** 4 19 Unacceptable toxicity perceived by patient 6 7 Relapse of disease 2 Withdrawal of consent Death (therapy related) 1 (0) 2 (0) Non-compliance to protocol Medical decision by investigator 5 Major protocol violation 1 Other reasons *multiple reasons possible **delay >2 weeks due to toxicity or in case of G3/4 non-hem toxicity
 Earlier termination of therapy (%) Reasons for earlier termination (events)* patients (n=15) patients (n=41) Unacceptable toxicity according to protocol** Unacceptable toxicity perceived by patient Relapse of disease. 2. Withdrawal of consent. Death (therapy related) 1 (0) 2 (0) Non-compliance to protocol. Medical decision by investigator. 5. Major protocol violation. 1. Other reasons. *multiple reasons possible. **delay >2 weeks due to toxicity or in case of G3/4 non-hem toxicity.")
60
Hematologic Toxicity (%)
TREAT: Toxicity Toxicity CPx CVb Mean Number (AE / SAE) 6.8 / 0.3 6.9 / 0.2 Hematologic Toxicity G3/4 (%) 10.5 76.5 Non-hematologic Toxicity G3/4 (%) 33 31 Hematologic Toxicity (%) G3/4 Anemia 1.5 Thrombocytopenia Neutropenia 9 69 Febrile Neutropenia 6 p<0.0001 p=0.7988
 6.8 / / 0.2. Hematologic. Toxicity G3/4 (%) Non-hematologic Toxicity G3/4 (%) Hematologic Toxicity (%) G3/4. Anemia Thrombocytopenia. Neutropenia Febrile Neutropenia. 6. p< p=")
61
TREAT: Time to treatment failure
TtTF: Time from surgery to withdrawal due to AE progression / relapse / death failure to return to therapy refusal of treatment / withdrawal of consent p<0.001 Withdrawal probability

62
TREAT: Conclusions CPx safe and feasible
less toxicity compared to CVb superior dose delivery compared to CVb high dose density (mg/m2/week) Dose delivery failure in CVb mostly due to Vb (delivery d15, d22) Efficacy: longer follow up to be awaited
 Dose delivery failure in CVb mostly due to Vb (delivery d15, d22) Efficacy: longer follow up to be awaited.")
63
Molecular Selection

64
Immunohistochemical (IHC) Staining of the Excision Repair Cross-Complementing 1 (ERCC1) Protein as Predictor of Benefit from adjuvant chemotherapy (CT) in the International Lung Cancer Trial (IALT) 761 pts. (28 centers,14 countries) evaluable for ERCC1 expression ERCC1 repairs cisplatin-DNA adducts, so expression indicates platinum resistance ERCC1 a “double-edged sword”; worse prognosis of NSCLC if low expression, but more responsive to platinum Soria, Proc ASCO 2006 A#7010; Olaussen K et al. N Engl J Med 2006;355:
 evaluable for ERCC1 expression. ERCC1 repairs cisplatin-DNA adducts, so expression indicates platinum resistance. ERCC1 a double-edged sword ; worse prognosis of NSCLC if low expression, but more responsive to platinum. Soria, Proc ASCO 2006 A#7010; Olaussen K et al. N Engl J Med 2006;355:")
65
ERCC1-Negative: Overall Survival
ERCC1-Positive: Overall Survival ERCC1-Negative: Overall Survival 47% 39% 46% 40% Adjusted HR = 0.65 95% PI [ ], p = 0.002 Adjusted HR = 1.14, 95% CI [ ], p = 0.40 Soria, Proc ASCO 2006 A#7010; Olaussen K et al. N Engl J Med 2006;355:

66
IFCT-0801 TASTE TAilored post-Surgical Therapy in Early stage NSCLC
Principal Investigator Jean-Charles SORIA Institut Gustave Roussy - Villejuif Biological Coordinator Marie Wislez Hôpital Tenon - Paris

67
TASTE design Non-SCC NSCLC stage II and IIIA (non-N2) Control Arm
CDDP - pemetrexed EGFR mutated Erlotinib Experimental Arm Customized ERCC1+ Observation EGFR wt ERCC1- CDDP-Pemetrexed Non-SCC NSCLC stage II and IIIA (non-N2) 67
 67.")
68
TASTE Results 150 pts randomized between May 2009 and July 2012,
74 in arm A (PEM/DDP) and 76 in arm B (Selected) Most pts were male (61%), > 60 years (51%), and smokers (91%) Pathological stage was IIA in 69 pt, IIB in 48 pt and IIIA in 32 pt. ERCC1 was positive in 38 pts (19 in each arm) – only 25%, not 44% expected EGFR mutation was identified in 10 pts (3 in arm A, 7 in arm B). Arm A, all pts received CP. Arm B, 7 pts received erlotinib, 53 pts received CP 16 were observed Median exposure time to erlotinib was 276 days (10-365). Out of 127 pts allocated to CP, 82% received the expected 4 cycles with a very good tolerability profile (no febrile neutropenia). Success rate was 80% (120 out of 150 pts): appropriate Tx assignment and Tx Soria J-C et al A-7505, ASCO ‘13
 and 76 in arm B (Selected) Most pts were male (61%), > 60 years (51%), and smokers (91%) Pathological stage was IIA in 69 pt, IIB in 48 pt and IIIA in 32 pt. ERCC1 was positive in 38 pts (19 in each arm) – only 25%, not 44% expected. EGFR mutation was identified in 10 pts (3 in arm A, 7 in arm B). Arm A, all pts received CP. Arm B, 7 pts received erlotinib, 53 pts received CP. 16 were observed. Median exposure time to erlotinib was 276 days (10-365). Out of 127 pts allocated to CP, 82% received the expected 4 cycles with a very good tolerability profile (no febrile neutropenia). Success rate was 80% (120 out of 150 pts): appropriate Tx assignment and Tx. Soria J-C et al A-7505, ASCO ‘13.")
69
TASTE Conclusions TASTE Implications
Met its primary end point for the phase II component, demonstrating feasibility of a national biology-driven trial in the adjuvant setting. Nevertheless, the phase III was canceled due to the unexpected unreliability of the ERCC1 IHC read-out. Current commercial antibodies are unable to distinguish all isoforms of ERCC1 TASTE Needs to be redone with accurate ERCC1 IHC Ab May have been responsible for the (-) MadeIT phase III trial in advanced NSCLC (relied on PCR mRNA probes and AQUA) TASTE Implications Soria J-C et al A-7505, ASCO ‘13
 MadeIT phase III trial in advanced NSCLC (relied on PCR mRNA probes and AQUA) TASTE Implications. Soria J-C et al A-7505, ASCO ‘13.")
70
Role of Targeted Therapy

71
ECOG 1505: Adjuvant Bevacizumab
RANDOM I Z E ELIGIBLE: Resected IB^-IIIA Lobectomy No prior chemo No planned XRT No h/o CVA/TIA No ATE w/in 1 yr STRATIFIED: Stage Histology Gender Chemo regimen* Chemotherapy X 4 cycles Chemotherapy x 4 cycles Plus Bevacizumab X 1 year *Investigator Choice of 4 chemo regimens ^ Revised to exclude IB < 4cm N >1500; closed to accrual summer 2013

72
ECOG 4599: Overall Survival
0.0 0.2 0.4 0.6 0.8 1.0 Proportion Surviving 6 42 48 18 30 12 24 36 Months HR=0.80; P=0.013 BV/PC 12.3 mo PC 10.3 mo Median Survival 1-year survival 51% vs 44% 2-year survival 23% vs 15% Sandler, et al. NEJM. 355;24. Dec

73
Chemotherapy Regimens
Therapy to start 6-12 weeks post-operatively Investigator Choice of Chemo - 4 cycles (12 wks) Cisplatin/Vinorelbine Cis 75 mg/m2 d 1, Vin 25 mg/m2 d1,8 q21 d Cisplatin/Docetaxel Cis 75 mg/m2 d 1, Docetaxel 75 mg/m2 d 1 q21 d Cisplatin/Gemcitabine Cis 75 mg/m2 d 1, Gem 1250 mg/m2 d1,8 q 21 d +/- Bevacizumab 15 mg/kg q 21 days x 12 mos
 Cisplatin/Vinorelbine. Cis 75 mg/m2 d 1, Vin 25 mg/m2 d1,8 q21 d. Cisplatin/Docetaxel. Cis 75 mg/m2 d 1, Docetaxel 75 mg/m2 d 1 q21 d. Cisplatin/Gemcitabine. Cis 75 mg/m2 d 1, Gem 1250 mg/m2 d1,8 q 21 d. +/- Bevacizumab 15 mg/kg q 21 days x 12 mos.")
74
Chemotherapy Regimens: amended 2010
Therapy to start 6-12 weeks post-operatively Investigator Choice of Chemo - 4 cycles (12 wks) Cisplatin/Pemetrexed Cis 75 mg/m2 d1, Pemetrexed 500 mg/m2 d1 Cisplatin/Vinorelbine Cis 75 mg/m2 d 1, Vin 25 mg/m2 d1,8 q21 d Cisplatin/Docetaxel Cis 75 mg/m2 d 1, Docetaxel 75 mg/m2 d 1 q21 d Cisplatin/Gemcitabine Cis 75 mg/m2 d 1, Gem 1250 mg/m2 d1,8 q 21 d +/- Bevacizumab 15 mg/kg q 21 days x 12 mos
 Cisplatin/Pemetrexed. Cis 75 mg/m2 d1, Pemetrexed 500 mg/m2 d1. Cisplatin/Vinorelbine. Cis 75 mg/m2 d 1, Vin 25 mg/m2 d1,8 q21 d. Cisplatin/Docetaxel. Cis 75 mg/m2 d 1, Docetaxel 75 mg/m2 d 1 q21 d. Cisplatin/Gemcitabine. Cis 75 mg/m2 d 1, Gem 1250 mg/m2 d1,8 q 21 d. +/- Bevacizumab 15 mg/kg q 21 days x 12 mos.")
75
RADIANT Trial: Adjuvant Trial of Erlotinib in NSCLC
Stage IB, II, or IIIA NSCLC* Complete surgical resection And subsequent adjuvant chemo No prior or concurrent neoadjuvant or adjuvant N=1654 RANDOMIZE٭ 2 Arm A Erlotinib qd 2 years 1 Arm B Placebo qd 2 years *Enriched Population: FISH and/or IHC (+)
")
76
RADIANT Trial: Adjuvant Trial of Erlotinib in NSCLC
Stage IB, II, or IIIA NSCLC* Complete surgical resection And subsequent adjuvant chemo No prior or concurrent neoadjuvant or adjuvant N=1654 RANDOMIZE٭ 2 Arm A Erlotinib qd 2 years Accrual Completed April, 2010 1 Arm B Placebo qd 2 years *Enriched Population: FISH and/or IHC (+)
")
77
IPASS: Progression-free survival in EGFR mutation positive and negative patients
EGFR mutation negative Gefitinib (n=132) Carboplatin/paclitaxel (n=129) Gefitinib (n=91) Carboplatin/paclitaxel (n=85) HR (95% CI) = 0.48 (0.36, 0.64) p<0.0001 No. events gefitinib, 97 (73.5%) No. events C/P, 111 (86.0%) Median PFS G, 9.5 months Median PFS C/P, 6.3 months HR (95% CI) = 2.85 (2.05, 3.98) p<0.0001 No. events gefitinib , 88 (96.7%) No. events C/P, 70 (82.4%) Median PFS G, 1.5 months Median PFS C/P, 5.5 months 1.0 1.0 0.8 0.8 0.6 0.6 Probability of progression-free survival Probability of progression-free survival 0.4 0.4 0.2 0.2 0.0 0.0 4 8 12 16 20 24 4 8 12 16 20 24 Months Months Patients at risk : Gefitinib 132 108 71 31 11 3 91 21 4 2 1 C/P 129 103 37 7 2 1 85 58 14 1 Treatment by subgroup interaction test, p<0.0001 Cox analysis with covariates; HR <1 implies a lower risk of progression on gefitinib; ITT population Fukuoka et al, abstract 8006, ASCO 2009; Mok et al NEJM 2010 77
 Carboplatin/paclitaxel (n=129) Gefitinib (n=91) Carboplatin/paclitaxel (n=85) HR (95% CI) = 0.48 (0.36, 0.64) p< No. events gefitinib, 97 (73.5%) No. events C/P, 111 (86.0%) Median PFS G, 9.5 months Median PFS C/P, 6.3 months. HR (95% CI) = 2.85 (2.05, 3.98) p< No. events gefitinib , 88 (96.7%) No. events C/P, 70 (82.4%) Median PFS G, 1.5 months Median PFS C/P, 5.5 months Probability of progression-free survival. Probability of progression-free survival Months. Months. Patients at risk : Gefitinib C/P Treatment by subgroup interaction test, p< Cox analysis with covariates; HR <1 implies a lower risk of progression on gefitinib; ITT population. Fukuoka et al, abstract 8006, ASCO 2009; Mok et al NEJM")
78
Phase II trial SELECT trial: adjuvant erlotinib in resected, early stage NSCLC pts with EGFR mutations PI L Sequist SCREENING PHASE TREATMENT PHASE Screen tumor for activating EGFR mutations (del 19, L858R) Resected stage IA-IIIA NSCLC +/- adjuvant chemo Adjuvant erlotinib x 2 years surveillance Surveillance CT scans and CTC analysis q 6 mos x 3 years then q 12 mos x 2 years Biopsy at recurrence, sequence EGFR gene for new mutations, FISH for EGFR and MET copy number N=100 Primary Endpoint: Two year disease-free survival Enroll if: screen + or documented EGFR mutation positive –and- No evidence recurrence on baseline CT scans
 Resected stage IA-IIIA NSCLC. +/- adjuvant chemo. Adjuvant erlotinib. x 2 years. surveillance. Surveillance CT scans and CTC analysis q 6 mos x 3 years then q 12 mos x 2 years. Biopsy at recurrence, sequence EGFR gene for new mutations, FISH for EGFR and MET copy number. N=100. Primary Endpoint: Two year disease-free survival. Enroll if: screen + or documented EGFR mutation positive –and- No evidence recurrence on baseline CT scans.")
79
SELECT Trial: Adjuvant Erlotinib in Resected NSCLC Disease Free Survival

80
BR 19: Adjuvant Trial of Gefitinib in NSCLC
RANDOMI ZE٭ Stage IB, II, or IIIA NSCLC Complete surgical resection No prior or concurrent neoadjuvant or adjuvant N=1242 Arm A Gefitinib qd 2 years Arm B Placebo qd 2 years ٭ Modified 2004 to allow adjuvant chemotherapy CAN-NCIC-BR19, CTSU, ECOG-CAN-NCIC-BR19, SWOG-CAN-NCIC-BR19 Protocol. Clinical Trials (PDQ®). At: Commenced October 2002. 80
. At: Commenced October")
81
* Trend toward impaired outcome for EGFR mutation pts receiving Gef [HR of OS: 1.51]
Goss ASCO 2010 Abstr LBA7005
![* Trend toward impaired outcome for EGFR mutation pts receiving Gef [HR of OS: 1.51]](http://slideplayer.com/slide/3232295/11/images/81/%2A+Trend+toward+impaired+outcome+for+EGFR+mutation+pts+receiving+Gef+%5BHR+of+OS%3A+1.51%5D.jpg "Goss ASCO 2010 Abstr LBA7005.")
83
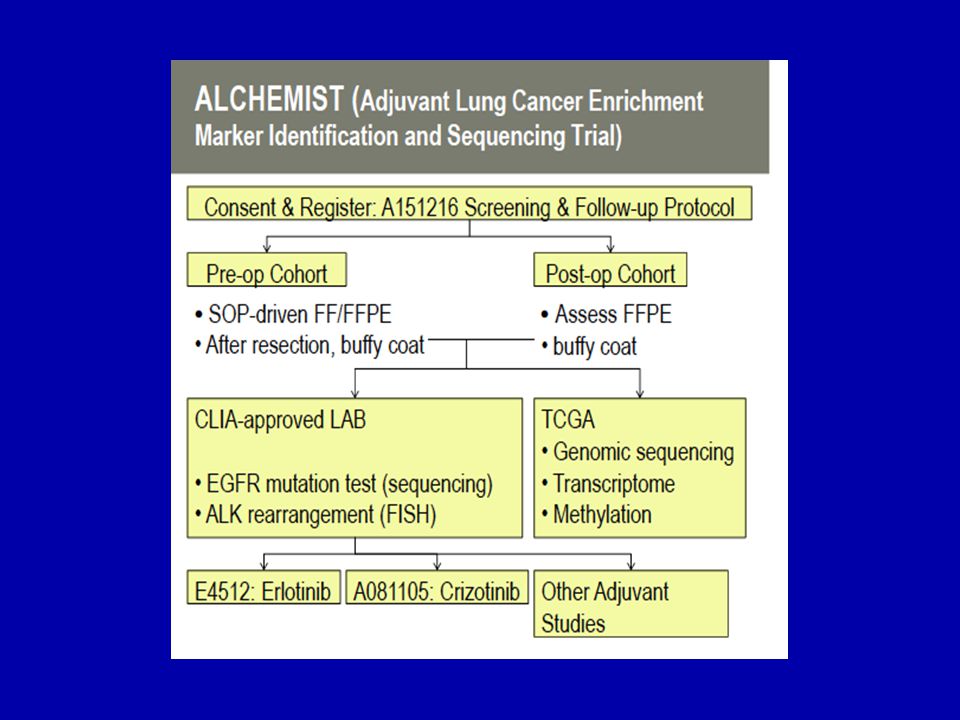
ALCHEMIST E4512 A081105 A151216 Target ALK+ EGFRmut Registry
Prevalence ~5% ~10% All comers n 336 410 Primary Endpt DFS-OS OS -- Power 80% 85% One-sided α 0.025 0.05 HR 0.67 Adjunct Peripheral screening for ALK; RTPCR to identify fusion partners Targeted sequence and kinome analysis; PRO and QOL Extended sequencing for additional targets; correlation with local testing

84
Vaccines

85
MAGE-A3 Antigen (melanoma antigen family A, 3)
Truly tumor-specific Not expressed on normal cells (RT-PCR) Expressed by various tumor types Lung % Bladder 35% Head & Neck 49% Melanoma 74% Associated with poorer prognosis (Bolli et al.,2002; Gure et al.,2005) Member of a large family of genes (portfolio)
 Expressed by various tumor types. Lung 35-50% Bladder 35% Head & Neck 49% Melanoma 74% Associated with poorer prognosis. (Bolli et al.,2002; Gure et al.,2005) Member of a large family of genes (portfolio)")
86
MAGE A3 ASCI* randomized phase II
Stage pIB or pII: double-blind, randomly assigned 2:1 to postoperative MAGE-A3 vaccination or placebo. Vaccination was started >6 weeks after surgery, with 5 vaccinations at 3-week intervals, followed by 8 vaccinations every 3 months. Other anti-cancer adjuvant therapy was not allowed. Primary endpoint was time-to-recurrence, other endpoints were recurrence rates at different times, and survival. * antigen-specific cancer immune therapeutic Vansteenkiste et al, ASCO 2006, abstract 7019

87
Safety Status 182 patients / 1214 MAGE-A3 doses administered
Well tolerated Mild grade 1 or 2 toxicities Local or systemic reactions, 48 hours 29 grade 3 or 4 adverse events in 21 patients Three grade 3 events, possibly related to treatment Leading to withdrawal of 2 patients (local pain, COPD exacerbation)
")
88
Disease-Free Interval
HR= (95% CI = ) p= % one-sided Vansteenkiste et al, ASCO 2006, abstract 7019
 p= % one-sided Vansteenkiste et al, ASCO 2006, abstract")
89
Efficacy Endpoints Overview
Final analysis 05 Oct, 2006 Cox regression model (95% confidence interval) P-value from Cox regr. model adjusted for stratification covariates HR with a 10% one-sided 0.73 Disease-Free Interval HR = 0.73 ( ) P=0.107 0.73 Disease-Free Survival HR = 0.73 ( ) 0.66 Overall Survival HR = 0.66 ( ) Hazard ratio « MAGE-A3 » better « Control » better
 P-value from Cox regr. model adjusted for stratification covariates. HR with a 10% one-sided Disease-Free Interval. HR = 0.73 ( ) P= Disease-Free Survival. HR = 0.73 ( ) Overall Survival. HR = 0.66 ( ) Hazard ratio. « MAGE-A3 » better. « Control » better.")
90
Pathological stage IB, II, IIIA platinum based chemotherapy)
MAGE Trial Design Resectable NSCLC Surgery Pathological stage IB, II, IIIA No chemotherapy Chemotherapy (up to 4 cycles platinum based chemotherapy) R MAGE-A3 +AS15 Placebo R MAGE-A3 +AS15 Placebo MAGRIT Trial
 R. MAGE-A3 +AS15. Placebo. R. MAGE-A3 +AS15. Placebo. MAGRIT Trial.")
91
MAGRIT: Phase III Largest lung cancer study EVER Began in October 2007
Goal: 2270 patients from 400 centers in 33 countries in Europe, North and South America, Asia, Australia 2289 ultimately enrolled

92
Role of Adjuvant RT in Stage II and Stage IIIA

93
Should the pt receive adj RT?
Yes No Maybe

94
Adjuvant Radiotherapy: Meta-analysis 1998
Individual data from 9 randomized trials including 2128 patients Treatment details (staging, surgery, RT) highly variable among series PORT: better local control: 29% fewer local recurrences LR vs 276 LR for no RT Overall HR = 1.21 ( ) ~ survival decrement of 7 % at two years (55% vs 48%) Increase risk greater for early stage patients(Stage I/II vs. III) Lancet 25 July 1998
 highly variable among series. PORT: better local control: 29% fewer local recurrences LR vs 276 LR for no RT. Overall HR = 1.21 ( ) ~ survival decrement of 7 % at two years (55% vs 48%) Increase risk greater for early stage patients(Stage I/II vs. III) Lancet 25 July")
95
PORT Meta-analysis Survival Curves
Stewart et al Lancet 1998

96
PORT - Heterogeneity of Hazard
No increased risk for patients with N2 disease Patients with the least to gain have the most to lose Stewart et al Lancet 1998

97
PORT Meta-analysis Methodologic Flaws
Variable and unspecified staging Variable and unspecified interval between resection and PORT Inadequate RT Suboptimal doses; large fields Poor treatment planning Outmoded techniques (e.g.: use of low-energy photons or 60Co for a substantial proportion of patients) Inclusion of N0 patients Unpublished data (2 of 9 studies) Relatively short F/U (< 4 yrs) Stewart et al Lancet 1998
 Inclusion of N0 patients. Unpublished data (2 of 9 studies) Relatively short F/U (< 4 yrs) Stewart et al Lancet")
98
Risks of PORT with Modern Technology
Retrospective review 202 patients treated with surgery and PORT for Stage II and III disease Median dose 55 Gy Actuarial rate of death from intercurrent disease was 13.5% compared to expected rate of 10% Machtay et al JCO 2001

99
ANITA TRIAL: N2 Disease – Influence of RT

100
ANITA TRIAL: N2 Disease – Influence of RT RT Effect? Or Serendipity?

101
ANITA - PORT Evaluation
PORT: 33% on obs, 22% on chemo For all Chemo > XRT = chemo/XRT > 0 For N2 Chemo/XRT > chemo > XRT > 0 XRT No Yes Chemo All pts MST 26mo 93mo 50mo 46mo N2 MST 13mo 24mo 23mo 47mo Rosell, IASLC 11, Abs Pr3, 2005

102
Plot of overall survival for N2 patients stratified by postoperative radiotherapy (PORT) use – SEER data Lally, B. E. et al. J Clin Oncol; 24:

103
PORT Conclusions PORT has no role in N0 or N1 disease
Role of PORT in N2 is controversial Recent subset and retrospective analyses hint at benefit Ongoing “Lung ART” trial in France 700 pts with resected N2 randomized to PORT or not Adjuvant chemo allowed 1st Accrual sluggish

104
“Lung ART” P.I. Dr Cécile Le Pechoux
Completely resected N2 NSCLC Primary end-point: DFS (Sample size: 700 patients) S U R G E Y Conformal RT No post-op RT 54 Gy/27-30 fxs Pre or post-op chemotherapy allowed Concomitant chemo not allowed Sponsors: FNCLCC, IFCT, LARS-G, EORTC
 S. U. R. G. E. Y. Conformal RT. No post-op RT. 54 Gy/27-30 fxs. Pre or post-op chemotherapy allowed. Concomitant chemo not allowed. Sponsors: FNCLCC, IFCT, LARS-G, EORTC.")
105
Conclusions: Adjuvant Therapy
Adjuvant Platinum-based Chemotherapy is the Standard of Care for Resected Stage II-IIIA NSCLC Improves OS 5%-15% at 5 years with newer drugs Fit elderly patients (< 75 yrs) benefit as much as younger patients Ongoing trials with molecularly determined Tx, erlotinib, bevacizumab, vaccines Controversies Benefit in IB Neoadjuvant vs adjuvant therapy Which chemotherapy to use PORT
 benefit as much as younger patients. Ongoing trials with molecularly determined Tx, erlotinib, bevacizumab, vaccines. Controversies. Benefit in IB. Neoadjuvant vs adjuvant therapy. Which chemotherapy to use. PORT.")
Similar presentations

















 patients Policy.>")

