Download presentation
Presentation is loading. Please wait.

1
Dr. Carles Pericay Pijaume
“Enfermedad limitada al hígado en cáncer colorrectal metastásico RAS WT: ¿qué aporta Panitumumab?”. Dr. Carles Pericay Pijaume Oncología Médica, Hospital Universitari de Sabadell, Corporació Sanitària Parc Taulí (Sabadell) Madrid, 12 de Febrero de 2015
 Madrid, 12 de Febrero de")
2
CRC liver metastases are common and predict a poor prognosis if untreated
In 2012, CRC was the 2nd most common cancer in Europe:1 447,000 new cases 215,000 deaths ~ 50% of CRC patients develop liver metastases2 Liver metastases responsible for 2/3 of CRC patient deaths2 0-6% 5 year survival for untreated CRC liver metastases3 From an estimated 3.45 million new cases of cancer (excluding non-melanoma skin cancer) in Europe in 2012, the most common sites were female breast (464,000 cases), followed by colorectal (447,000), prostate (417,000) and lung (410,000).1 The most common causes of death from cancer were cancers of the lung (353,000 deaths), colorectal (215,000), breast (131,000) and stomach (107,000).1 Hepatic metastases develop in 50% of patients and are responsible for two thirds of colorectal cancer patient deaths.2 A 5-year survival rate of 90.3% was reported for localised cancer of the colon and rectum for the period in 18 regions of the USA by the National Cancer Institute (NCI) Surveillance, Epidemiology, and End Results (SEER) Program.3 A median 5-year survival of 0% (range 0–6%) for patients with colorectal hepatic metastases who did not undergo resection was concluded from a review of six relevant studies in a systematic review that aimed to include all relevant prospective and retrospective series reporting the outcomes of surgical resection with curative intent of colorectal hepatic metastases.4 REFERENCES 1. Ferlay J, et al. Cancer incidence and mortality patterns in Europe: Estimates for 40 countries in Eur J Cancer 2013;49:1374–403. 2. Van den Eynde M, Hendlisz A. Treatment of colorectal liver metastases: a review. Rev Recent Clin Trials 2009;4:56–62. 3. Howlader N, et al. SEER Cancer Statistics Review (CSR), Natl. Cancer Inst (accessed 19 Mar2014). 4. Simmonds PC, et al. Surgical resection of hepatic metastases from colorectal cancer: a systematic review of published studies. Br J Cancer 2006;94:982–99. 1. Ferlay J et al. Eur J Cancer. 2013;49(6):1374–403; 2. Van den Eynde M, and Hendlisz A. Rev Recent Clin Trials. 2009;4(1):56–62; 3. Simmonds PC et al. Br J Cancer. 2006;94(7):982–99. CRC, colorectal cancer.
 in Europe in 2012, the most common sites were female breast (464,000 cases), followed by colorectal (447,000), prostate (417,000) and lung (410,000).1. The most common causes of death from cancer were cancers of the lung (353,000 deaths), colorectal (215,000), breast (131,000) and stomach (107,000).1. Hepatic metastases develop in 50% of patients and are responsible for two thirds of colorectal cancer patient deaths.2. A 5-year survival rate of 90.3% was reported for localised cancer of the colon and rectum for the period in 18 regions of the USA by the National Cancer Institute (NCI) Surveillance, Epidemiology, and End Results (SEER) Program.3. A median 5-year survival of 0% (range 0–6%) for patients with colorectal hepatic metastases who did not undergo resection was concluded from a review of six relevant studies in a systematic review that aimed to include all relevant prospective and retrospective series reporting the outcomes of surgical resection with curative intent of colorectal hepatic metastases.4. REFERENCES. 1. Ferlay J, et al. Cancer incidence and mortality patterns in Europe: Estimates for 40 countries in Eur J Cancer 2013;49:1374– Van den Eynde M, Hendlisz A. Treatment of colorectal liver metastases: a review. Rev Recent Clin Trials 2009;4:56– Howlader N, et al. SEER Cancer Statistics Review (CSR), Natl. Cancer Inst (accessed 19 Mar2014). 4. Simmonds PC, et al. Surgical resection of hepatic metastases from colorectal cancer: a systematic review of published studies. Br J Cancer 2006;94:982– Ferlay J et al. Eur J Cancer. 2013;49(6):1374–403; 2. Van den Eynde M, and Hendlisz A. Rev Recent Clin Trials. 2009;4(1):56–62; 3. Simmonds PC et al. Br J Cancer. 2006;94(7):982–99. CRC, colorectal cancer.")
3
Resection of liver metastases improves survival
70 60 50 40 30 20 10 R0 resected (16 studies) Median 5-year survival, % Resected, R0/R1 unclear (19 studies) Non-radical resection (11 studies) Not resected (6 studies) 30% 32% 7% 0% This slide shows results from a qualitative systematic review reporting the available evidence for the effectiveness of surgical resection of colorectal liver metastases.1 Out of 529 independent studies, 30 met all eligibility criteria for the review, which included surgical series published after 1980 reporting the outcomes of at least 100 patients who underwent surgical resection of colorectal liver metastases with curative intent.1 Median 5-year survival in 16 studies of patients undergoing R0 resection of colorectal liver metastases with curative intent was 30% (range 15–67%).1 In contrast, patients with colorectal liver metastases who did not undergo resection in 6 studies had a median 5-year survival of 0% (range 0–6%).1 A more recent systematic review of 142 studies published between 1999 and 2010 revealed a median 5-year survival for patients with liver metastases after resection of 38% (range of 16%–71%).2 Results from the LiverMetSurvey, involving 14,774 patients from 330 centres in 58 countries, who underwent surgery for liver metastases, reported a 5-year survival of 42% in patients who underwent liver resection, compared with 8% in unresected patients.3 REFERENCES 1. Simmonds PC, Primrose JN, Colquitt JL, et al. Surgical resection of hepatic metastases from colorectal cancer: a systematic review of published studies. Br J Cancer 2006;94:982–99. 2. Kanas GP, Taylor A, Primrose JN, et al. Survival after liver resection in metastatic colorectal cancer: review and meta-analysis of prognostic factors. Clin Epidemiol 2012;4:283–301. 3. Adam R, De Gramont A, Figueras J, et al. The oncosurgery approach to managing liver metastases from colorectal cancer: a multidisciplinary international consensus. Oncologist 2012;17:1225–39. Surgical series published after 1980 Simmonds PC et al. Br J Cancer. 2006;94(7):982–99 Error bars indicate range.
 Median 5-year survival, % Resected, R0/R1 unclear (19 studies) Non-radical resection (11 studies) Not resected (6 studies) 30% 32% 7% 0% This slide shows results from a qualitative systematic review reporting the available evidence for the effectiveness of surgical resection of colorectal liver metastases.1. Out of 529 independent studies, 30 met all eligibility criteria for the review, which included surgical series published after 1980 reporting the outcomes of at least 100 patients who underwent surgical resection of colorectal liver metastases with curative intent.1. Median 5-year survival in 16 studies of patients undergoing R0 resection of colorectal liver metastases with curative intent was 30% (range 15–67%).1. In contrast, patients with colorectal liver metastases who did not undergo resection in 6 studies had a median 5-year survival of 0% (range 0–6%).1. A more recent systematic review of 142 studies published between 1999 and 2010 revealed a median 5-year survival for patients with liver metastases after resection of 38% (range of 16%–71%).2. Results from the LiverMetSurvey, involving 14,774 patients from 330 centres in 58 countries, who underwent surgery for liver metastases, reported a 5-year survival of 42% in patients who underwent liver resection, compared with 8% in unresected patients.3. REFERENCES. 1. Simmonds PC, Primrose JN, Colquitt JL, et al. Surgical resection of hepatic metastases from colorectal cancer: a systematic review of published studies. Br J Cancer 2006;94:982– Kanas GP, Taylor A, Primrose JN, et al. Survival after liver resection in metastatic colorectal cancer: review and meta-analysis of prognostic factors. Clin Epidemiol 2012;4:283– Adam R, De Gramont A, Figueras J, et al. The oncosurgery approach to managing liver metastases from colorectal cancer: a multidisciplinary international consensus. Oncologist 2012;17:1225–39. Surgical series published after Simmonds PC et al. Br J Cancer. 2006;94(7):982–99. Error bars indicate range.")
4
Current definition of liver metastases resectability
The criteria for liver metastasis resectability have not been standardized1-3 Medical fitness for surgery Resectability1-5 Oncological considerations Technical considerations e.g. Resectable extrahepatic disease Number of lesions ≥ 5 Tumour progression R0 with ≥ 25%–30% FLR Complex procedure Until recently, the classic contraindications for resection of CRC liver metastases have been: 4 metastases, disease outside the liver; metastatic nodes in the liver pedicule; a resection margin of <1 cm; the presence of co-morbid disease; incomplete resection; the involvement of more than 2 sushepatic veins.1 However, these limitations for resectability are currently now outdated since advances in surgery and chemotherapy have increased the feasibility of liver metastases resection. However, there remains no consensus regarding which factors have the best prognostic value.1–5 In addition to the definition of resectability in the NCCN Guidelines6, other example definitions include: “The potential for complete resection with tumour-free margins (R0 resection) with preservation of at least two disease-free liver segments with viable vascular inflow, outflow, and biliary drainage and an FLR volume of 30%.”4 “After confirmation of medical fitness for general anaesthesia and major abdominal surgery, [...] eligibility is determined by two domains: oncological and technical. From an oncological perspective, evaluation for extrahepatic disease and the response to pre-operative systemic therapy are the main considerations. From a technical perspective, resection is the preferred treatment option if all viable tumours can be removed with negative margins, while leaving an adequate functional liver remnant.”5 The R classification denotes absence or presence of residual tumour after treatment.7 R0 corresponds to resection for cure or complete remission with microscopically negative margins; R1 to microscopic residual tumour; R2 to macroscopic residual tumour.3,7 REFERENCES: 1. Van den Eynde M, Hendlisz A. Treatment of colorectal liver metastases: a review. Rev Recent Clin Trials 2009;4:56–62. 2. Schmoll HJ, Van Cutsem E, Stein A, et al. ESMO Consensus Guidelines for management of patients with colon and rectal cancer. a personalized approach to clinical decision making. Ann Oncol 2012;23:2479–516. 3. Spolverato G, Ejaz A, Azad N, et al. Surgery for colorectal liver metastases: The evolution of determining prognosis. World J Gastrointest Oncol 2013;5:207–21. 4. Adam R, De Gramont A, Figueras J, et al. The oncosurgery approach to managing liver metastases from colorectal cancer: a multidisciplinary international consensus. Oncologist 2012;17:1225–39. 5. Adams RB, Aloia T a, Loyer E, et al. Selection for hepatic resection of colorectal liver metastases: expert consensus statement. HPB 2013;15:91–103. 6. National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: Colon Cancer [v ]. (accessed 20 Feb2014). 7. Hermanek P, Wittekind C. The pathologist and the residual tumor (R) classification. Pathol Res Pr 1994;190:115–23. NCCN Guidelines criteria for resection suitability6 “... the likelihood of achieving complete resection of all evident disease with negative surgical margins and maintaining adequate liver reserve” 1. Schmoll HJ et al. Ann Oncol. 2012;23(10):2479–516; 2. Spolverato G et al. World J Gastrointest Oncol. 2013;5(12):207–21; 3. Van den Eynde M, and Hendlisz A. Rev Recent Clin Trials. 2009;4(1):56–62; 4. Adams RB et al. HPB. 2013;15(2):91–103; 5. Adam R et al. Oncologist. 2012;17(10):1225–39; 6. NCCN Clinical Practice Guidelines in Oncology: Colon Cancer [v ]. (accessed 20/02/2014). FLR, functional liver remnant; R0, resection with microscopically negative margins
 with preservation of at least two disease-free liver segments with viable vascular inflow, outflow, and biliary drainage and an FLR volume of 30%. 4. After confirmation of medical fitness for general anaesthesia and major abdominal surgery, [...] eligibility is determined by two domains: oncological and technical. From an oncological perspective, evaluation for extrahepatic disease and the response to pre-operative systemic therapy are the main considerations. From a technical perspective, resection is the preferred treatment option if all viable tumours can be removed with negative margins, while leaving an adequate functional liver remnant. 5. The R classification denotes absence or presence of residual tumour after treatment.7. R0 corresponds to resection for cure or complete remission with microscopically negative margins; R1 to microscopic residual tumour; R2 to macroscopic residual tumour.3,7 REFERENCES: 1. Van den Eynde M, Hendlisz A. Treatment of colorectal liver metastases: a review. Rev Recent Clin Trials 2009;4:56– Schmoll HJ, Van Cutsem E, Stein A, et al. ESMO Consensus Guidelines for management of patients with colon and rectal cancer. a personalized approach to clinical decision making. Ann Oncol 2012;23:2479– Spolverato G, Ejaz A, Azad N, et al. Surgery for colorectal liver metastases: The evolution of determining prognosis. World J Gastrointest Oncol 2013;5:207– Adam R, De Gramont A, Figueras J, et al. The oncosurgery approach to managing liver metastases from colorectal cancer: a multidisciplinary international consensus. Oncologist 2012;17:1225– Adams RB, Aloia T a, Loyer E, et al. Selection for hepatic resection of colorectal liver metastases: expert consensus statement. HPB 2013;15:91– National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: Colon Cancer [v ]. (accessed 20 Feb2014). 7. Hermanek P, Wittekind C. The pathologist and the residual tumor (R) classification. Pathol Res Pr 1994;190:115–23. NCCN Guidelines criteria for resection suitability the likelihood of achieving complete resection of all evident disease with negative surgical margins and maintaining adequate liver reserve 1. Schmoll HJ et al. Ann Oncol. 2012;23(10):2479–516; 2. Spolverato G et al. World J Gastrointest Oncol. 2013;5(12):207–21; 3. Van den Eynde M, and Hendlisz A. Rev Recent Clin Trials. 2009;4(1):56–62; 4. Adams RB et al. HPB. 2013;15(2):91–103; 5. Adam R et al. Oncologist. 2012;17(10):1225–39; 6. NCCN Clinical Practice Guidelines in Oncology: Colon Cancer [v ]. (accessed 20/02/2014). FLR, functional liver remnant; R0, resection with microscopically negative margins.")
5
ESMO 2012 Clinical Guidelines Stratification of mCRC patients for 1st-line treatment
Metastatic colorectal cancer Group 0 Group 1 Group 2 Group 3 Yes Initially R0 resectable No Potentially R0 resectable with CT & patient can tolerate CT and surgery Yes No Yes Symptomatic or aggressive disease As described in ESMO 2012 Guidelines, mCRC patients can be divided into four clinical groups, by a hierarchy of parameters describing localization, extent, and resectability of the disease, tumour dynamics, co-morbidity, potential of the patient to tolerate chemotherapy and secondary surgical treatment. Treatment strategy, aim and intensity for each of these groups is described in the guidelines. REFERENCE: Schmoll HJ, et al. ESMO Consensus Guidelines for management of patients with colon and rectal cancer. A personalized approach to clinical decision making. Ann Oncol 2012;23: No Yes Yes Far advanced/bulky disease Patient can tolerate CT No No Schmoll HJ et al. Ann Oncol. 2012;23(10):2479–516 CT, chemotherapy; R0, resection with microscopically negative margins.
:2479–516. CT, chemotherapy; R0, resection with microscopically negative margins.")
6
Metastatic colorectal cancer
mCRC patient distribution between ESMO guideline first-line treatment stratification groups Metastatic colorectal cancer ~15%1,2 ~85%1,2 Initially R0 resectable Non-resectable at clinical presentation 10-30%2 70-90%2 The only potentially curative standard treatment in CRC patients with liver metastases is liver resection or local ablative treatment (e.g., radiofrequency, cryoablation).1 Unfortunately, approximately 85% of patients with stage IV CRC, referred to specialist centres, have metastatic liver disease which is considered to be unresectable at presentation.1,2 However, up to 30 % of initially unresectable patients may become resectable following preoperative, neoadjuvant, combination chemotherapy.2 REFERENCES: 1. Van den Eynde M, Hendlisz A. Treatment of colorectal liver metastases: a review. Rev Recent Clin Trials 2009;4:56–62. 2. Nordlinger B et al. Does chemotherapy prior to liver resection increase the potential for cure in patients with metastatic colorectal cancer? A report from the European Colorectal Metastases Treatment Group. Eur J Cancer. 2007;43(14):2037–45. 3. Schmoll HJ, et al. ESMO Consensus Guidelines for management of patients with colon and rectal cancer. A personalized approach to clinical decision making. Ann Oncol 2012;23: Potentially resectable Never resectable Group 2* Group 1 Group 3 Group 0 Schmoll HJ et al. Ann Oncol. 2012;23(10):2479–516; 1. Van den Eynde M, and Hendlisz A. Rev Recent Clin Trials. 2009;4(1):56–62; 2. Nordlinger B et al. Eur J Cancer. 2007;43(14):2037–45. *Some patients may become resectable following exceptional response to treatment. CT, chemotherapy; R0, resection with microscopically negative margins.
.1. Unfortunately, approximately 85% of patients with stage IV CRC, referred to specialist centres, have metastatic liver disease which is considered to be unresectable at presentation.1,2. However, up to 30 % of initially unresectable patients may become resectable following preoperative, neoadjuvant, combination chemotherapy.2. REFERENCES: 1. Van den Eynde M, Hendlisz A. Treatment of colorectal liver metastases: a review. Rev Recent Clin Trials 2009;4:56– Nordlinger B et al. Does chemotherapy prior to liver resection increase the potential for cure in patients with metastatic colorectal cancer A report from the European Colorectal Metastases Treatment Group. Eur J Cancer. 2007;43(14):2037– Schmoll HJ, et al. ESMO Consensus Guidelines for management of patients with colon and rectal cancer. A personalized approach to clinical decision making. Ann Oncol 2012;23: Potentially resectable. Never resectable. Group 2* Group 1. Group 3. Group 0. Schmoll HJ et al. Ann Oncol. 2012;23(10):2479–516; 1. Van den Eynde M, and Hendlisz A. Rev Recent Clin Trials. 2009;4(1):56–62; 2. Nordlinger B et al. Eur J Cancer. 2007;43(14):2037–45. *Some patients may become resectable following exceptional response to treatment. CT, chemotherapy; R0, resection with microscopically negative margins.")
7
Metastatic colorectal cancer
mCRC patient distribution between ESMO guideline first-line treatment stratification groups Metastatic colorectal cancer ~15%1,2 ~85%1,2 Initially R0 resectable Non-resectable at clinical presentation 10-30%2 70-90%2 The only potentially curative standard treatment in CRC patients with liver metastases is liver resection or local ablative treatment (e.g., radiofrequency, cryoablation).1 Unfortunately, approximately 85% of patients with stage IV CRC, referred to specialist centres, have metastatic liver disease which is considered to be unresectable at presentation.1,2 However, up to 30 % of initially unresectable patients may become resectable following preoperative, neoadjuvant, combination chemotherapy.2 REFERENCES: 1. Van den Eynde M, Hendlisz A. Treatment of colorectal liver metastases: a review. Rev Recent Clin Trials 2009;4:56–62. 2. Nordlinger B et al. Does chemotherapy prior to liver resection increase the potential for cure in patients with metastatic colorectal cancer? A report from the European Colorectal Metastases Treatment Group. Eur J Cancer. 2007;43(14):2037–45. 3. Schmoll HJ, et al. ESMO Consensus Guidelines for management of patients with colon and rectal cancer. A personalized approach to clinical decision making. Ann Oncol 2012;23: Potentially resectable Never resectable Group 2* Group 1 Group 3 Group 0 Schmoll HJ et al. Ann Oncol. 2012;23(10):2479–516; 1. Van den Eynde M, and Hendlisz A. Rev Recent Clin Trials. 2009;4(1):56–62; 2. Nordlinger B et al. Eur J Cancer. 2007;43(14):2037–45. *Some patients may become resectable following exceptional response to treatment. CT, chemotherapy; R0, resection with microscopically negative margins.
.1. Unfortunately, approximately 85% of patients with stage IV CRC, referred to specialist centres, have metastatic liver disease which is considered to be unresectable at presentation.1,2. However, up to 30 % of initially unresectable patients may become resectable following preoperative, neoadjuvant, combination chemotherapy.2. REFERENCES: 1. Van den Eynde M, Hendlisz A. Treatment of colorectal liver metastases: a review. Rev Recent Clin Trials 2009;4:56– Nordlinger B et al. Does chemotherapy prior to liver resection increase the potential for cure in patients with metastatic colorectal cancer A report from the European Colorectal Metastases Treatment Group. Eur J Cancer. 2007;43(14):2037– Schmoll HJ, et al. ESMO Consensus Guidelines for management of patients with colon and rectal cancer. A personalized approach to clinical decision making. Ann Oncol 2012;23: Potentially resectable. Never resectable. Group 2* Group 1. Group 3. Group 0. Schmoll HJ et al. Ann Oncol. 2012;23(10):2479–516; 1. Van den Eynde M, and Hendlisz A. Rev Recent Clin Trials. 2009;4(1):56–62; 2. Nordlinger B et al. Eur J Cancer. 2007;43(14):2037–45. *Some patients may become resectable following exceptional response to treatment. CT, chemotherapy; R0, resection with microscopically negative margins.")
8
What is conversion chemotherapy?
Resection mCRC with initially non-resectable liver metastases Tumour shrinkage In patients with unresectable liver metastases, emerging data have shown that neoadjuvant chemotherapy can render some metastases resectable, hence opening up the possibility of prolonged survival.1 Chemotherapy given to convert unresectable liver metastases to resectable is referred to as “conversion chemotherapy.”2 Note: the term “neoadjuvant chemotherapy” is reserved for chemotherapy for resectable and potentially resectable disease prior to surgery with or without adjuvant chemotherapy after surgery.2 The goal of conversion chemotherapy is not specifically the eradication of micrometastatic disease, but rather optimal size regression of visible metastases.3 When chemotherapy is initiated to achieve resectability, the aim should be for as short a treatment course as possible and surgery performed as soon as the metastases become resectable.2,4 REFERENCES: 1. Nordlinger B, Benoist S. Benefits and risks of neoadjuvant therapy for liver metastases. J Clin Oncol 2006;24:4954–5. 2. Adam R, De Gramont A, Figueras J, et al. The oncosurgery approach to managing liver metastases from colorectal cancer: a multidisciplinary international consensus. Oncologist 2012;17:1225–39. 3. National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: Colon Cancer [v ]. (accessed 20/02/2014). 4. Nordlinger B, Vauthey J-N, Poston G, et al. The timing of chemotherapy and surgery for the treatment of colorectal liver metastases. Clin Color Cancer 2010;9:212–8. 1. Adam R, et al. Oncologist 2012;17:1225–39; 2. Nordlinger B, Benoist S. J Clin Oncol 2006;24:4954–5; 3. Nordlinger B, et al. Clin Colorectal Cancer 2010;9:212–8; 4. Schmoll HJ et al. Ann Oncol. 2012;23(10):2479–516. *Chemotherapy to convert unresectable liver metastases to resectable.
. 4. Nordlinger B, Vauthey J-N, Poston G, et al. The timing of chemotherapy and surgery for the treatment of colorectal liver metastases. Clin Color Cancer 2010;9:212–8. 1. Adam R, et al. Oncologist 2012;17:1225–39; 2. Nordlinger B, Benoist S. J Clin Oncol 2006;24:4954–5; 3. Nordlinger B, et al. Clin Colorectal Cancer 2010;9:212–8; 4. Schmoll HJ et al. Ann Oncol. 2012;23(10):2479–516. *Chemotherapy to convert unresectable liver metastases to resectable.")
9
unresectable liver metastases
Conversion CT + surgery for treatment of mCRC with unresectable liver metastases Single centre study of consecutive patients F O L W - U P mCRC with unresectable liver metastases (n = 184) Conversion chemotherapy* Surgery Response evaluated every 2 months Minimum follow-up 5 years The aim of this study was to evaluate long-term outcome after combining downsizing chemotherapy and rescue surgery in patients with initially unresectable colorectal liver metastases (CLM) and to define prognostic factors of cure. Inclusion: all patients with unresectable CLM at the time of diagnosis who underwent rescue surgery after conversion chemotherapy and had a minimum follow-up of 5 years from surgery were included. Definition of technically unresectable disease: when complete resection of all metastases would leave < 30% of liver remnant, or < 40% when patients received intensive preoperative chemotherapy. Definition of cure: a disease-free interval of ≥ 5 years after the last hepatectomy or last resection of extrahepatic metastases. Furthermore, patients had to be free of disease at last follow-up. Patients who died of not curatively resected metastases or disease recurrence were defined as “noncured.” Response to chemotherapy was evaluated every 2 months by a multidisciplinary team according to the WHO guidelines during the initial study period and to RECIST (Response Evaluation Criteria in Solid Tumours) during the final period. Patients responding to chemotherapy were reconsidered for surgery when the overall strategy could achieve complete clearance of intra- and extrahepatic metastases. However, when tumour-free margins were not possible owing to major vascular or biliary contact, resection was still indicated provided that all tumours could be macroscopically resected. REFERENCE: Adam R, Wicherts DA, de Haas RJ, et al. Patients with initially unresectable colorectal liver metastases: is there a possibility of cure? J Clin Oncol 2009;27: Study objectives: evaluation of possibility of cure, determination of predictive factors of disease cure Adam R, et al. J Clin Oncol 2009; 27: *Last preoperative regimen, FL (18%), FOLFOX (62%), FOLFIRI (6%), FOLFOXIRI (9%), Other (5%)
 Conversion. chemotherapy* Surgery. Response evaluated every 2 months. Minimum follow-up 5 years. The aim of this study was to evaluate long-term outcome after combining downsizing chemotherapy and rescue surgery in patients with initially unresectable colorectal liver metastases (CLM) and to define prognostic factors of cure. Inclusion: all patients with unresectable CLM at the time of diagnosis who underwent rescue surgery after conversion chemotherapy and had a minimum follow-up of 5 years from surgery were included. Definition of technically unresectable disease: when complete resection of all metastases would leave < 30% of liver remnant, or < 40% when patients received intensive preoperative chemotherapy. Definition of cure: a disease-free interval of ≥ 5 years after the last hepatectomy or last resection of extrahepatic metastases. Furthermore, patients had to be free of disease at last follow-up. Patients who died of not curatively resected metastases or disease recurrence were defined as noncured. Response to chemotherapy was evaluated every 2 months by a multidisciplinary team according to the WHO guidelines during the initial study period and to RECIST (Response Evaluation Criteria in Solid Tumours) during the final period. Patients responding to chemotherapy were reconsidered for surgery when the overall strategy could achieve complete clearance of intra- and extrahepatic metastases. However, when tumour-free margins were not possible owing to major vascular or biliary contact, resection was still indicated provided that all tumours could be macroscopically resected. REFERENCE: Adam R, Wicherts DA, de Haas RJ, et al. Patients with initially unresectable colorectal liver metastases: is there a possibility of cure J Clin Oncol 2009;27: Study objectives: evaluation of possibility of cure, determination of predictive factors of disease cure. Adam R, et al. J Clin Oncol 2009; 27: *Last preoperative regimen, FL (18%), FOLFOX (62%), FOLFIRI (6%), FOLFOXIRI (9%), Other (5%)")
10
An oncosurgical approach offers the chance of cure to a subgroup of initially non-resectable patients 1.0 OS (n = 184) DFS (n = 184) 0.8 0.6 5-year survival 10-year survival Survival probability 0.4 33% 27% 0.2 19% 15% Graph shows overall and disease-free survival curves of patients with initially unresectable disease who underwent resection after downsizing chemotherapy. 184 patients with liver metastases considered potentially resectable after downsizing. 55% were male and median age was 56.9 years. Patients had a median of 5 (range 1-22) metastases and median size at diagnosis was 50mm (range 6-160mm). Metastases were bilobar in 76% of cases. Surgery was possible after one line of chemotherapy in 88% of cured patients. Noncured patients more often received two or more lines of chemotherapy before hepatectomy could be reconsidered (33% v 13%; P = 0.05). Patients who achieved cure were administered a median number of 8 cycles (range, 4-29 cycles) and a last preoperative regimen that most often consisted of fluorouracil, leucovorin, and oxaliplatin (75%). 148 patients (80%) had a follow-up of 5 years or more after hepatectomy. Of these, 24 patients (16%) were considered cured. 112 patients (76%) died of disease and formed the non-cured patient group. 12 patients (8%) were excluded because of a disease-free interval of < 5 years after last resection (n = 3), the presence of disease recurrence at last follow-up (n = 8), or death from a nontumoral cause (n = 1; 9 months after hepatectomy). REFERENCE: Adam R, Wicherts DA, de Haas RJ, et al. Patients with initially unresectable colorectal liver metastases: is there a possibility of cure? J Clin Oncol 2009;27: 1 2 3 4 5 6 7 8 9 10 Cure was achieved in 16% of CRC patients with liver metastases who became eligible for surgery after response to conversion chemotherapy Time (years) Adam R, et al. J Clin Oncol 2009; 27: Cure = disease-free ≥ 5 years after last hepatectomy / last resection of extrahepatic metastases; CRC, colorectal cancer; DFS, disease-free survival; OS, overall survival.
 DFS (n = 184) year survival. 10-year survival. Survival probability % 27% % 15% Graph shows overall and disease-free survival curves of patients with initially unresectable disease who underwent resection after downsizing chemotherapy. 184 patients with liver metastases considered potentially resectable after downsizing. 55% were male and median age was 56.9 years. Patients had a median of 5 (range 1-22) metastases and median size at diagnosis was 50mm (range 6-160mm). Metastases were bilobar in 76% of cases. Surgery was possible after one line of chemotherapy in 88% of cured patients. Noncured patients more often received two or more lines of chemotherapy before hepatectomy could be reconsidered (33% v 13%; P = 0.05). Patients who achieved cure were administered a median number of 8 cycles (range, 4-29 cycles) and a last preoperative regimen that most often consisted of fluorouracil, leucovorin, and oxaliplatin (75%). 148 patients (80%) had a follow-up of 5 years or more after hepatectomy. Of these, 24 patients (16%) were considered cured. 112 patients (76%) died of disease and formed the non-cured patient group. 12 patients (8%) were excluded because of a disease-free interval of < 5 years after last resection (n = 3), the presence of disease recurrence at last follow-up (n = 8), or death from a nontumoral cause (n = 1; 9 months after hepatectomy). REFERENCE: Adam R, Wicherts DA, de Haas RJ, et al. Patients with initially unresectable colorectal liver metastases: is there a possibility of cure J Clin Oncol 2009;27: Cure was achieved in 16% of CRC patients with liver metastases who became eligible for surgery after response to conversion chemotherapy. Time (years) Adam R, et al. J Clin Oncol 2009; 27: Cure = disease-free ≥ 5 years after last hepatectomy / last resection of extrahepatic metastases; CRC, colorectal cancer; DFS, disease-free survival; OS, overall survival.")
11
Response to CT correlates with liver resectability
Rate of liver resection following CT Response rate 0.3 0.4 0.6 0.5 0.7 0.8 0.0 0.2 0.1 Selected patients, r = 0.96 P = 0.002 Non-selected patients, r = 0.74 P < Phase III trial data, r = 0.67 P = 0.024 Resection rate This study reviewed reviewed the literature to explore the relationship between tumour response and resectability following chemotherapy. Studies and reports of retrospective analyses and prospective trials (phases I–III) in patients with CRC cancer treated with systemic chemotherapy were divided into: Studies that included only patients that have liver limited metastases (‘selected’ patients); 5 prospective phase II trials and 1 retrospective study Studies that included all mCRC patients (‘non-selected’ patients); 9 phase II studies and 5 phase III studies. The slide shows the correlation between objective response and resection rate. For selected patients (filled squares): A strong and highly significant correlation between the rates of liver resection and the tumour response to chemotherapy was found (r = 0.96, P = 0.002). The rate of R0 resection did not significantly correlate with the response rate (r = 0.43). For non-selected patients (triangles) a positive correlation between the response rate and the resection rate of liver metastases. This was true for the analysis of: all trials combined, open triangles, (r = 0.74, P <0.001), or phase III trials only, filled triangles, (r = 0.67, P = 0.024). A non-significant trend toward correlation was observed for R0 resections (r = 0.62, P = 0.08). The correlation in selected patients was not only steeper but also on a higher level than in unselected patients, meaning that a higher number of patients could be rendered potentially resectable. REFERENCE: Folprecht G, et al. Neoadjuvant treatment of unresectable colorectal liver metastases: correlation between tumour response and resection rates. Ann Oncol 2005;16:1311–9. 0.9 Patient selection and efficacy of pre-operative CT were strong predictors for resectability of liver metastases Folprecht G, et al. Ann Oncol 2005;16:1311–9. CT, chemotherapy
 in patients with CRC cancer treated with systemic chemotherapy were divided into: Studies that included only patients that have liver limited metastases (‘selected’ patients); 5 prospective phase II trials and 1 retrospective study. Studies that included all mCRC patients (‘non-selected’ patients); 9 phase II studies and 5 phase III studies. The slide shows the correlation between objective response and resection rate. For selected patients (filled squares): A strong and highly significant correlation between the rates of liver resection and the tumour response to chemotherapy was found (r = 0.96, P = 0.002). The rate of R0 resection did not significantly correlate with the response rate (r = 0.43). For non-selected patients (triangles) a positive correlation between the response rate and the resection rate of liver metastases. This was true for the analysis of: all trials combined, open triangles, (r = 0.74, P <0.001), or. phase III trials only, filled triangles, (r = 0.67, P = 0.024). A non-significant trend toward correlation was observed for R0 resections (r = 0.62, P = 0.08). The correlation in selected patients was not only steeper but also on a higher level than in unselected patients, meaning that a higher number of patients could be rendered potentially resectable. REFERENCE: Folprecht G, et al. Neoadjuvant treatment of unresectable colorectal liver metastases: correlation between tumour response and resection rates. Ann Oncol 2005;16:1311– Patient selection and efficacy of pre-operative CT were strong predictors for resectability of liver metastases. Folprecht G, et al. Ann Oncol 2005;16:1311–9. CT, chemotherapy.")
12
Placebo + FOLFOX4/XELOX
NO16966: BEV + CT significantly improves PFS but not RR or OS in combination with XELOX/FOLFOX4 (ITT) Response rate (%) 10 20 30 40 50 60 70 Placebo + FOLFOX4/XELOX BEV + FOLFOX4/XELOX 38 p=0.99 RR AVF2107g: Bevacizumab significantly improves RR, PFS and OS in combination with IFL (ITT) Response rate (%) 10 20 30 40 50 60 70 Placebo + IFL BEV + IFL 45 35 p=0.004 RR Saltz LB, et al. Bevacizumab in Combination With Oxaliplatin-Based Chemotherapy As First-Line Therapy in Metastatic Colorectal Cancer: A Randomized Phase III Study J Clin Oncol 2008;26(12): Reprinted with permission. © American Society of Clinical Oncology. All rights reserved Months Months 12
 Response rate (%) Placebo + FOLFOX4/XELOX. BEV + FOLFOX4/XELOX. 38. p=0.99. RR. AVF2107g: Bevacizumab significantly improves RR, PFS and OS in combination with IFL (ITT) Response rate (%) Placebo + IFL. BEV + IFL p= RR. Saltz LB, et al. Bevacizumab in Combination With Oxaliplatin-Based Chemotherapy As First-Line Therapy in Metastatic Colorectal Cancer: A Randomized Phase III Study. J Clin Oncol 2008;26(12): Reprinted with permission. © American Society of Clinical Oncology. All rights reserved. Months. Months. 12.")
13
CRYSTAL: Cetuximab + FOLFIRI significantly improves RR, PFS and OS vs FOLFIRI (KRAS wt)
Response rate (%) 10 20 30 40 50 60 70 FOLFIRI Cetuximab + FOLFIRI 57 p<0.001 RR OPUS: Cetuximab + FOLFOX4 significantly improves RR and PFS vs FOLFOX4 (KRAS wt) Response rate (%) 10 20 30 40 50 60 70 FOLFOX4 Cetuximab + FOLFOX4 57 34 p=0.0027 RR Van Cutsem E, et al. Cetuximab Plus Irinotecan, Fluorouracil, and Leucovorin As First-Line Treatment for Metastatic Colorectal Cancer: Updated Analysis of Overall Survival According to Tumor KRAS and BRAF Mutation Status. J Clin Oncol 2011;29 (15):2011–2019 Reprinted with permission. © (2011) American Society of Clinical Oncology. All rights reserved
 FOLFIRI. Cetuximab + FOLFIRI. 57. p< RR. OPUS: Cetuximab + FOLFOX4 significantly improves RR and PFS vs FOLFOX4 (KRAS wt) Response rate (%) FOLFOX4. Cetuximab + FOLFOX p= RR. Van Cutsem E, et al. Cetuximab Plus Irinotecan, Fluorouracil, and Leucovorin As First-Line Treatment for Metastatic Colorectal Cancer: Updated Analysis of Overall Survival According to Tumor KRAS and BRAF Mutation Status. J Clin Oncol 2011;29 (15):2011–2019. Reprinted with permission. © (2011) American Society of Clinical Oncology. All rights reserved.")
14
PRIME: Panitumumab + FOLFOX4 significantly improves RR and PFS vs FOLFOX4 (KRAS wt)
Response rate (%) 10 20 30 40 50 60 70 FOLFOX Pani + FOLFOX 57 48 p=0.018 RR Douillard JY, et al. Randomized, Phase III Trial of Panitumumab With Infusional Fluorouracil, Leucovorin, and Oxaliplatin (FOLFOX4) Versus FOLFOX4 Alone As First-Line Treatment in Patients With Previously Untreated Metastatic Colorectal Cancer: The PRIME Study. J Clin Oncol 2010;28(31):4697–4705. Reprinted with permission. © (2010) American Society of Clinical Oncology. All rights reserved.
 FOLFOX. Pani + FOLFOX p= RR. Douillard JY, et al. Randomized, Phase III Trial of Panitumumab With Infusional Fluorouracil, Leucovorin, and Oxaliplatin (FOLFOX4) Versus FOLFOX4 Alone As First-Line Treatment in Patients With Previously Untreated Metastatic Colorectal Cancer: The PRIME Study. J Clin Oncol 2010;28(31):4697–4705. Reprinted with permission. © (2010) American Society of Clinical Oncology. All rights reserved.")
15
CRYSTAL y OPUS (KRAS WT)
n RR (%) R0 resections (%) CRYSTAL FOLFIRI + ERBITUX FOLFIRI p<0.001 p=0.03 OPUS FOLFOX + ERBITUX FOLFOX 82 97 p<0.003 p=0.22 FOLFIRI + ERBITUX FOLFIRI 68 72 p=0.002 p=0.15 FOLFOX + ERBITUX FOLFOX 25 23 p=0.018 p=0.35 All patients Liver limited Van Cutsem ASCO-GI 2011
 R0 resections (%) CRYSTAL FOLFIRI + ERBITUX FOLFIRI p< p=0.03. OPUS FOLFOX + ERBITUX FOLFOX p< p=0.22. FOLFIRI + ERBITUX FOLFIRI p= p=0.15. FOLFOX + ERBITUX FOLFOX p= p=0.35. All patients. Liver limited. Van Cutsem ASCO-GI")
16
PRIME: Increased R0 resection rate in LLD
KRAS wt KRAS wt: LLD Patients (%) Patients (%) Douillard J-Y, et al. J Clin Oncol 2010;28:4697–4705; Petrelli F, et al. Int J Colorectal Dis 2012;27:997–1004
 Patients (%) Douillard J-Y, et al. J Clin Oncol 2010;28:4697–4705; Petrelli F, et al. Int J Colorectal Dis 2012;27:997–1004.")
17
Conceptualizing the relevance of DpR for survival
OS Lethal tumor load No tumor shrinkage Baseline tumor load PFS Tumor shrinkage PFS PFS Time under treatment Mansmann UR, et al. ASCO GI 2013 (Abstract no. 427)
")
18
CRYSTAL and OPUS: More patients demonstrate ETS when treated with cetuximab
Cetuximab + FOLFIRI CRYSTAL <20%* (n=115) ≥20%* (n=184) Cetuximab + FOLFIRI 1.0 Probability of OS 0.8 mOS 30.0 mo 0.6 38% 62% <20%* (n=115) ≥20%* (n=184) 0.4 HR p<0.001 0.2 mOS 18.6 mo 0.0 n=299 10 20 30 40 50 60 (months) OPUS Cetuximab + FOLFOX4 Cetuximab + FOLFOX4 1.0 ≥20%* (n=54) <20%* (n=24) Probability of OS 0.8 31% 69% mOS 26.0 mo ≥20%* (n=54) <20%* (n=24) 0.6 HR 0.43 p=0.006 0.4 mOS 15.7 mo 0.2 n=78 0.0 10 20 30 40 *Radiologic evaluation reported by the investigator and reviewed by an IRC (months) Piessevaux H, et al. JSMO 2012 (Abstract No. IS9-3)
 ≥20%* (n=184) Cetuximab + FOLFIRI Probability of OS mOS 30.0 mo % 62% <20%* (n=115) ≥20%* (n=184) 0.4. HR 0.53 p< mOS 18.6 mo n= (months) OPUS. Cetuximab + FOLFOX4. Cetuximab + FOLFOX ≥20%* (n=54) <20%* (n=24) Probability of OS % 69% mOS 26.0 mo. ≥20%* (n=54) <20%* (n=24) 0.6. HR p= mOS 15.7 mo n= *Radiologic evaluation reported by the investigator and reviewed by an IRC. (months) Piessevaux H, et al. JSMO 2012 (Abstract No. IS9-3)")
19
Patients with RECIST response
PRIME: More patients had RECIST response or ETS at week 8 with panitumumab + CT than with CT alone Patients with RECIST response Patients with ETS 39 51 10 20 30 40 50 60 70 80 38 39 69 10 20 30 40 50 60 70 80 56 Patients (%) Patients (%) FOLFOX (n = 298) Pani + FOLFOX (n=286) FOLFOX (n = 298) Pani + FOLFOX (n=284) Douillard J-Y, et al. ESMO 2012 (Abstract No. 558P)
 Patients (%) FOLFOX. (n = 298) Pani + FOLFOX (n=286) FOLFOX. (n = 298) Pani + FOLFOX (n=284) Douillard J-Y, et al. ESMO 2012 (Abstract No. 558P)")
20
OS was significantly longer in patients achieving RECIST response or ETS in both arms
FOLFOX FOLFOX + pani ETS <20% (n=130) ≥20% (n=158) <20% (n=87) ≥20% (n=197) Median OS, months (95% CI) 16.6 (12.4–18.8) 25.1 (22.1–32.8) 10.7 (9.4–16.1) 30.0 (27.2–33.1) HR, p-value HR=0.52, p<0.0001 HR=0.43, p<0.0001 Patients demonstrating ETS who received pantitumumab plus FOLFOX showed a greater OS benefit compared with those receiving FOLFOX alone (30.0 vs months) FOLFOX FOLFOX + pani RECIST response <30% (n=130) ≥30% (n=112) <30% (n=141) ≥30% (n=145) Median OS, months (95% CI) 17.6 (15.4–20.2) 29.5 (22.5–34.5) 18.0 (14.0–21.7) 30.3 (26.6–36.8) HR, p-value HR=0.54, p<0.0001 HR=0.53, p<0.0001 Douillard J-Y, et al. ESMO 2012 (Abstract No. 558P)
 ≥20% (n=158) <20% (n=87) ≥20% (n=197) Median OS, months. (95% CI) (12.4–18.8) (22.1–32.8) (9.4–16.1) (27.2–33.1) HR, p-value. HR=0.52, p< HR=0.43, p< Patients demonstrating ETS who received pantitumumab plus FOLFOX showed a greater OS benefit compared with those receiving FOLFOX alone (30.0 vs 25.1 months) FOLFOX. FOLFOX + pani. RECIST response. <30% (n=130) ≥30% (n=112) <30% (n=141) ≥30% (n=145) Median OS, months. (95% CI) (15.4–20.2) (22.5–34.5) (14.0–21.7) (26.6–36.8) HR, p-value. HR=0.54, p< HR=0.53, p< Douillard J-Y, et al. ESMO 2012 (Abstract No. 558P)")
21
Initially non-resectable
Downsizing initially unresectable metastases offers similar 5-year survival as initially resectable patients CRC liver metastases Initially resectable Initially non-resectable Conversion CT Resection Resection Untreated The long-term survival rates for those patients with unresectable metastases brought to surgery thanks to a response to chemotherapy are similar to those of patients with initially resectable metastases.1 Kanas et al. conducted a systematic review of 142 studies published between 1999 and 2010 of patients with colorectal liver metastases who underwent surgical liver resection.2 Median 5-year survival after resection for all patients with liver metastases was 38% (range 16%–71%; data from 86 studies). Median 5-year survival after resection for patients with initially resectable liver metastases was 38% (range 30%–68%; data from 10 studies). Median 5-year survival after resection for patients with initially unresectable liver metastases, who required pre-operative chemotherapy, was 37% (range 7.8%–79%; data from 13 studies). Simmonds et al. conducted a systematic review of studies published between 1999 and 2010 reporting the outcomes of at least 100 patients who underwent surgical resection of colorectal liver metastases with curative intent.3 Of the 30 studies that met eligibility criteria, 6 studies reported patients who did not undergo resection; these patients had a median 5-year survival of 0% (range 0-6%). 16 studies presented 5-year survival for patients undergoing R0 resection; median 5-year survival for these studies was 30% (range 15–67%). REFERNCES: 1. Van den Eynde M, Hendlisz A. Treatment of colorectal liver metastases: a review. Rev Recent Clin Trials 2009;4:56–62. 2. Kanas GP, et al. Survival after liver resection in metastatic colorectal cancer: review and meta-analysis of prognostic factors. Clin Epidemiol 2012;4:283–301. 3. Simmonds PC, et al. Surgical resection of hepatic metastases from colorectal cancer: a systematic review of published studies. Br J Cancer 2006;94:982–99. 5-year survival* (range) 38% (30-68%)2 37% (8-79%)2 0% (0-6%)3 1. Van den Eynde M, and Hendlisz A. Rev Recent Clin Trials. 2009;4(1):56–62; 2. Kanas GP, et al. Clin Epidemiol 2012;4:283–301; 3. Simmonds PC et al. Br J Cancer. 2006;94(7):982–99. *median; CRC, colorectal cancer; CT, chemotherapy.
. Median 5-year survival after resection for patients with initially resectable liver metastases was 38% (range 30%–68%; data from 10 studies). Median 5-year survival after resection for patients with initially unresectable liver metastases, who required pre-operative chemotherapy, was 37% (range 7.8%–79%; data from 13 studies). Simmonds et al. conducted a systematic review of studies published between 1999 and 2010 reporting the outcomes of at least 100 patients who underwent surgical resection of colorectal liver metastases with curative intent.3. Of the 30 studies that met eligibility criteria, 6 studies reported patients who did not undergo resection; these patients had a median 5-year survival of 0% (range 0-6%). 16 studies presented 5-year survival for patients undergoing R0 resection; median 5-year survival for these studies was 30% (range 15–67%). REFERNCES: 1. Van den Eynde M, Hendlisz A. Treatment of colorectal liver metastases: a review. Rev Recent Clin Trials 2009;4:56– Kanas GP, et al. Survival after liver resection in metastatic colorectal cancer: review and meta-analysis of prognostic factors. Clin Epidemiol 2012;4:283– Simmonds PC, et al. Surgical resection of hepatic metastases from colorectal cancer: a systematic review of published studies. Br J Cancer 2006;94:982–99. 5-year survival* (range) 38% (30-68%)2. 37% (8-79%)2. 0% (0-6%)3. 1. Van den Eynde M, and Hendlisz A. Rev Recent Clin Trials. 2009;4(1):56–62; 2. Kanas GP, et al. Clin Epidemiol 2012;4:283–301; 3. Simmonds PC et al. Br J Cancer. 2006;94(7):982–99. *median; CRC, colorectal cancer; CT, chemotherapy.")
22
A meta analysis of resectability and outcomes with anti-EGFR mAb therapy (KRAS exon 2 WT, LLD)
Comparison of first-line CT + / - cetuximab or panitumumab KRAS WT initially unresectable liver-limited mCRC Meta analysis of RCTs: Primary outcome: rate of R0 resection Secondary outcomes: PFS, OS and ORR Four RCTs involving 484 KRAS WT patients were included: PRIME, Douillard 2010 COIN, Maughan 2011 CRYSTAL, Van Cutsem 2011 OPUS, Van Cutsem 2011 This slide describes a systematic review that compared the performance of chemotherapy plus an anti-EGFR monoclonal antibody to that of chemotherapy alone in permitting R0 resection of liver-confined CRC metastases in a KRAS wild-type population. Publications (prior to August 2011) were identified that reported RCTs of patients with unresectable, liver-only, KRAS WT colorectal metastases, treated with or without cetuximab or panitumumab. Studies were selected if they reported: (1) total number of patients with KRAS wild-type, liver confined disease, (2) number of R0 resected patients, (3) number of responses (if available) and (4) hazard ratio (HR) for PFS and/or OS (if available). REFERENCE: Petrelli F, Barni S. Resectability and outcome with anti-EGFR agents in patients with KRAS wild-type colorectal liver-limited metastases: a meta-analysis. Int J Colorectal Dis 2012;27: Petrelli F, Barni S. Int J Colorectal Dis 2012;27: CT, chemotherapy; mCRC, metastatic colorectal cancer; LLD, liver limited disease; mAb, monoclonal antibody; ORR, overall response rate; OS, overall survival; PFS, progression-free survival.
 were identified that reported RCTs of patients with unresectable, liver-only, KRAS WT colorectal metastases, treated with or without cetuximab or panitumumab. Studies were selected if they reported: (1) total number of patients with KRAS wild-type, liver confined disease, (2) number of R0 resected patients, (3) number of responses (if available) and (4) hazard ratio (HR) for PFS and/or OS (if available). REFERENCE: Petrelli F, Barni S. Resectability and outcome with anti-EGFR agents in patients with KRAS wild-type colorectal liver-limited metastases: a meta-analysis. Int J Colorectal Dis 2012;27: Petrelli F, Barni S. Int J Colorectal Dis 2012;27: CT, chemotherapy; mCRC, metastatic colorectal cancer; LLD, liver limited disease; mAb, monoclonal antibody; ORR, overall response rate; OS, overall survival; PFS, progression-free survival.")
23
Impact of anti-EGFR mAb therapy on outcomes (KRAS exon 2 WT, LLD)
Response rate R0 resection rate P = 0.001 P = 0.04 This slide shows the results of a systematic review and meta analysis comparing the performance of chemotherapy plus an anti-EGFR mAb to that of chemotherapy alone in permitting R0 resection of liver-confined CRC metastases in a KRAS wild-type population. The results show that chemotherapy plus cetuximab or panitumumab increases the likelihood of obtaining a disease response by 70% (from 43% to 72%) and a R0 liver resection by 60% (from 11% to 18%) in an unselected population with liver-only disease enrolled in four randomized trials. These data confirm the notion that a strong correlation exists between ORR and the resection rate in patients with isolated liver metastases. This meta-analysis confirmed that in a selected CRC population with unresectable liver-limited disease, the addition of an anti-EGFR mAb to 5-fluorouracil + oxaliplatin (or irinotecan-based) chemotherapy confers a significant benefit in terms of resectability and PFS compared to standard multi-agent chemotherapy alone. REFERENCE: Petrelli F, Barni S. Resectability and outcome with anti-EGFR agents in patients with KRAS wild-type colorectal liver-limited metastases: a meta-analysis. Int J Colorectal Dis 2012;27: CT alone CT+ EGFR mAb CT alone CT + EGFR mAb Meta-analysis indicates EGFR inhibitors increase R0 resection rate by 60% in mCRC patients with unresectable liver-limited disease Petrelli F, Barni S. Int J Colorectal Dis 2012;27: CT, chemotherapy; mAb, monoclonal antibody; R0, resection with microscopically negative margins.
 and a R0 liver resection by 60% (from 11% to 18%) in an unselected population with liver-only disease enrolled in four randomized trials. These data confirm the notion that a strong correlation exists between ORR and the resection rate in patients with isolated liver metastases. This meta-analysis confirmed that in a selected CRC population with unresectable liver-limited disease, the addition of an anti-EGFR mAb to 5-fluorouracil + oxaliplatin (or irinotecan-based) chemotherapy confers a significant benefit in terms of resectability and PFS compared to standard multi-agent chemotherapy alone. REFERENCE: Petrelli F, Barni S. Resectability and outcome with anti-EGFR agents in patients with KRAS wild-type colorectal liver-limited metastases: a meta-analysis. Int J Colorectal Dis 2012;27: CT alone. CT+ EGFR mAb. CT alone. CT + EGFR mAb. Meta-analysis indicates EGFR inhibitors increase R0 resection rate by 60% in mCRC patients with unresectable liver-limited disease. Petrelli F, Barni S. Int J Colorectal Dis 2012;27: CT, chemotherapy; mAb, monoclonal antibody; R0, resection with microscopically negative margins.")
24
20060314 Trial FOLFIRI + panitumumab in 1st-line mCRC
D O F T R A M F O L W - U P S A E T Y S T U D Y E N O F mCRC (n = 150) FOLFIRI (Q2W) + panitumumab 6 mg/kg (Q2W on day 1 of each cycle) Disease assessment every 8 weeks until week 48, then every 3 months until disease progression 8 weeks after end of treatment This was a first-line, single-arm phase 2 study prospectively evaluating the relationship between KRAS status and response to combination therapy with panitumumab and FOLFIRI. Eligible patients received panitumumab (6 mg/kg; intravenous infusion [IV]) on day 1 of a 14-day cycle with the initial dose administered over 60 minutes ± 15 minutes prior to chemotherapy. If the first dose was well tolerated subsequent infusions were given over 30 minutes ± 10 minutes prior to chemotherapy. No panitumumab-specific pre-medication was given before administration. Treatment was to be given until progression or unacceptable toxicity. All analyses were descriptive. REFERENCE: Köhne CH, Hofheinz R, Mineur L, et al. First-line panitumumab plus irinotecan/5-fluorouracil/leucovorin treatment in patients with metastatic colorectal cancer. J Cancer Res Clin Oncol 2012;138:65-72. Study endpoints: ORR (1°), PFS, disease control rate, DoR, TTP, DoSD, TTF, safety The incidence of R0 resection was also reported protocol ID: ; ClinicalTrials.gov ID: NCT Köhne C-H, et al. J Cancer Res Clin Oncol 2012; 138:65-72. DoR, duration of response; PFS, progression-free survival; TTP, time to progression; DoSD, duration of stable disease; TTF, time to treatment failure; ORR, overall response rate.
 FOLFIRI (Q2W) + panitumumab 6 mg/kg (Q2W on day 1 of each cycle) Disease assessment every 8 weeks until week 48, then every 3 months until disease progression. 8 weeks after end of treatment. This was a first-line, single-arm phase 2 study prospectively evaluating the relationship between KRAS status and response to combination therapy with panitumumab and FOLFIRI. Eligible patients received panitumumab (6 mg/kg; intravenous infusion [IV]) on day 1 of a 14-day cycle with the initial dose administered over 60 minutes ± 15 minutes prior to chemotherapy. If the first dose was well tolerated subsequent infusions were given over 30 minutes ± 10 minutes prior to chemotherapy. No panitumumab-specific pre-medication was given before administration. Treatment was to be given until progression or unacceptable toxicity. All analyses were descriptive. REFERENCE: Köhne CH, Hofheinz R, Mineur L, et al. First-line panitumumab plus irinotecan/5-fluorouracil/leucovorin treatment in patients with metastatic colorectal cancer. J Cancer Res Clin Oncol 2012;138: Study endpoints: ORR (1°), PFS, disease control rate, DoR, TTP, DoSD, TTF, safety. The incidence of R0 resection was also reported. protocol ID: ; ClinicalTrials.gov ID: NCT Köhne C-H, et al. J Cancer Res Clin Oncol 2012; 138: DoR, duration of response; PFS, progression-free survival; TTP, time to progression; DoSD, duration of stable disease; TTF, time to treatment failure; ORR, overall response rate.")
25
KRAS WT tumours were more likely to respond to treatment with panitumumab plus FOLFIRI
Objective response rate R0 resection rate, patients with LLD This study involved 154 patients, enrolled at 36 study centres in Austria, Belgium, France, Germany, and Sweden, during 2007 and 2008. KRAS data were available for 145/154 (94%) patients: 59% were KRAS WT and 41% were KRAS MT. Objective responses occurred in 49% of patients: 56% versus 38% in the KRAS WT versus MT groups [(18% difference (95% CI 1–35%); odds ratio 2.1 (95% CI 1.0–4.4)]. Median duration of response was 13.0 versus 7.4 months. More patients in the KRAS WT group underwent R0 resection (8% vs. 5%). Overall, 11 patients (7%; 95% CI 4–12%) had a R0 resection. In patients with liver-only metastases at baseline (n = 52), R0 resections were performed in 8 patients (15%) overall and 6/31 patients (19%) versus 1/16 patients (6%) in the KRAS WT and MT groups, respectively. Median progression-free survival also favoured the KRAS WT group (8.9 vs. 7.2 months). The most common adverse events (any grade) were integument toxicities (98%), diarrhoea (79%) and stomatitis/oral mucositis (51%). REFERENCE: Köhne CH, Hofheinz R, Mineur L, et al. First-line panitumumab plus irinotecan/5-fluorouracil/leucovorin treatment in patients with metastatic colorectal cancer. J Cancer Res Clin Oncol 2012;138:65-72 KRAS MT KRAS WT KRAS MT KRAS WT A higher proportion of patients with KRAS WT than with KRAS MT had an objective response and R0 resection Köhne C-H, et al. J Cancer Res Clin Oncol 2012; 138:65-72. CT, chemotherapy; R0, resection with microscopically negative margins.
 patients: 59% were KRAS WT and 41% were KRAS MT. Objective responses occurred in 49% of patients: 56% versus 38% in the KRAS WT versus MT groups [(18% difference (95% CI 1–35%); odds ratio 2.1 (95% CI 1.0–4.4)]. Median duration of response was 13.0 versus 7.4 months. More patients in the KRAS WT group underwent R0 resection (8% vs. 5%). Overall, 11 patients (7%; 95% CI 4–12%) had a R0 resection. In patients with liver-only metastases at baseline (n = 52), R0 resections were performed in 8 patients (15%) overall and 6/31 patients (19%) versus 1/16 patients (6%) in the KRAS WT and MT groups, respectively. Median progression-free survival also favoured the KRAS WT group (8.9 vs. 7.2 months). The most common adverse events (any grade) were integument toxicities (98%), diarrhoea (79%) and stomatitis/oral mucositis (51%). REFERENCE: Köhne CH, Hofheinz R, Mineur L, et al. First-line panitumumab plus irinotecan/5-fluorouracil/leucovorin treatment in patients with metastatic colorectal cancer. J Cancer Res Clin Oncol 2012;138: KRAS MT. KRAS WT. KRAS MT. KRAS WT. A higher proportion of patients with KRAS WT than with KRAS MT had an objective response and R0 resection. Köhne C-H, et al. J Cancer Res Clin Oncol 2012; 138: CT, chemotherapy; R0, resection with microscopically negative margins.")
26
panitumumab 6 mg/kg (Q2W)
PRIME study FOLFOX4 ± panitumumab in 1st-line treatment of metastatic CRC FOLFOX4 (Q2W) + panitumumab 6 mg/kg (Q2W) E N D O F T R A M F O L W - U P N G T E R M mCRC KRAS* WT (n = 1183) R FOLFOX4 (Q2W) 1:1 Disease assessment every 8 weeks Patients were stratified by:1 Performance status (ECOG 0-1 vs. 2) Geographic region: Western Europe, Canada, and Australia vs. rest of the world The evaluation of changes in HRQoL using the EQ-5D was a tertiary objective.3 Patients were evaluated every 8 weeks until progression. Responses were confirmed at least 4 weeks after the criteria for response were first met. Patients were followed for safety 30 days after the last study drug administration and for survival every 3 months. Enrolment period was from Aug 2006 to Feb 2008. Participating countries: Argentina, Australia, Belgium, Brazil, Canada, Chile, Costa Rica, Czech Republic, Estonia, France, Hungary, Italy, Latvia, Mexico, Poland, South Africa, Spain, Switzerland, United Kingdom. Please refer to Douillard JY, et al. J Clin Oncol 2010;28: for further information. REFERENCES: 1. Douillard JY, Siena S, Cassidy J, et al. Randomized, phase III trial of panitumumab with infusional fluorouracil, leucovorin, and oxaliplatin (FOLFOX4) versus FOLFOX4 alone as first-line treatment in patients with previously untreated metastatic colorectal cancer: the PRIME study. J Clin Oncol 2010;28: 2. Douillard JY, Oliner KS, Siena S, et al. Panitumumab–FOLFOX4 Treatment and RAS Mutations in Colorectal Cancer. N Engl J Med 2013;369: 3. Bennett L, Zhao Z, Barber B, et al. Health-related quality of life in patients with metastatic colorectal cancer treated with panitumumab in first- or second-line treatment. Br J Cancer 2011;105: Study endpoints: PFS (1°), OS, ORR, TTR, DoR, safety and tolerability Primary Analysis: pre-specified; after >50% of KRAS exon 2 WT patients had died1,2 Updated OS Analysis: exploratory; after >80% of KRAS exon 2 WT & MT patients died2 *KRAS status was prospectively analysed; FOLFOX4, infusional fluorouracil, leucovorin, and oxaliplatin; DoR, duration of response; ORR, objective response rate; OS, overall survival; TTR, time to response; Q2W, every 2 weeks. ID: ; ClinicalTrials.gov ID: NCT ; 1. Douillard JY, et al. J Clin Oncol 2010; 28: ; 2. Douillard JY, et al. N Engl J Med 2013; 369:
 + panitumumab 6 mg/kg (Q2W) E. N. D. O. F. T. R. A. M. F. O. L. W. - U. P. N. G. T. E. R. M. mCRC. KRAS* WT. (n = 1183) R. FOLFOX4 (Q2W) 1:1. Disease assessment every 8 weeks. Patients were stratified by:1. Performance status (ECOG 0-1 vs. 2) Geographic region: Western Europe, Canada, and Australia vs. rest of the world. The evaluation of changes in HRQoL using the EQ-5D was a tertiary objective.3. Patients were evaluated every 8 weeks until progression. Responses were confirmed at least 4 weeks after the criteria for response were first met. Patients were followed for safety 30 days after the last study drug administration and for survival every 3 months. Enrolment period was from Aug 2006 to Feb Participating countries: Argentina, Australia, Belgium, Brazil, Canada, Chile, Costa Rica, Czech Republic, Estonia, France, Hungary, Italy, Latvia, Mexico, Poland, South Africa, Spain, Switzerland, United Kingdom. Please refer to Douillard JY, et al. J Clin Oncol 2010;28: for further information. REFERENCES: 1. Douillard JY, Siena S, Cassidy J, et al. Randomized, phase III trial of panitumumab with infusional fluorouracil, leucovorin, and oxaliplatin (FOLFOX4) versus FOLFOX4 alone as first-line treatment in patients with previously untreated metastatic colorectal cancer: the PRIME study. J Clin Oncol 2010;28: Douillard JY, Oliner KS, Siena S, et al. Panitumumab–FOLFOX4 Treatment and RAS Mutations in Colorectal Cancer. N Engl J Med 2013;369: Bennett L, Zhao Z, Barber B, et al. Health-related quality of life in patients with metastatic colorectal cancer treated with panitumumab in first- or second-line treatment. Br J Cancer 2011;105: Study endpoints: PFS (1°), OS, ORR, TTR, DoR, safety and tolerability. Primary Analysis: pre-specified; after >50% of KRAS exon 2 WT patients had died1,2. Updated OS Analysis: exploratory; after >80% of KRAS exon 2 WT & MT patients died2. *KRAS status was prospectively analysed; FOLFOX4, infusional fluorouracil, leucovorin, and oxaliplatin; DoR, duration of response; ORR, objective response rate; OS, overall survival; TTR, time to response; Q2W, every 2 weeks. ID: ; ClinicalTrials.gov ID: NCT ; 1. Douillard JY, et al. J Clin Oncol 2010; 28: ; 2. Douillard JY, et al. N Engl J Med 2013; 369:")
27
PRIME study RAS analysis Post-hoc analysis objective
Post-hoc analysis to evaluate tumour shrinkage, resection rates and PFS and OS outcomes for patients with RAS WT and LLD treated in the 1st-line PRIME study In PRIME, patients who had received no prior chemotherapy for mCRC and who had unresectable disease at baseline were randomised 1:1 to panitumumab + FOLFOX4 or FOLFOX4.1 In this exploratory analysis, data were analysed for the subgroup of patients with RAS WT mCRC2 and LLD to determine the following for each treatment:3 The proportion of patients achieving ≥30% tumour shrinkage/ response by week 8 and the ORR; Rates of metastasectomy and complete resection; Median PFS, OS and 3-year OS rates. REFERENCES: 1. Douillard JY, Siena S, Cassidy J, et al. Randomized, phase III trial of panitumumab with infusional fluorouracil, leucovorin, and oxaliplatin (FOLFOX4) versus FOLFOX4 alone as first-line treatment in patients with previously untreated metastatic colorectal cancer: the PRIME study. J Clin Oncol 2010;28: 2. Douillard JY, Oliner KS, Siena S, et al. Panitumumab–FOLFOX4 Treatment and RAS Mutations in Colorectal Cancer. N Engl J Med 2013;369: 3. Peeters M, et al. Resection Rates and Survival in Patients with Wild-Type KRAS/NRAS Metastatic Colorectal Cancer and Liver Metastases: Data from the Prime Study. EJC 2013; 49 (suppl 4):abstract MC (and poster). Peeters M, et al. EJC 2013; 49 (suppl 4):abstract MC (and poster). RAS WT, KRAS & NRAS exons 2/3/4; LLD, liver-limited disease
 versus FOLFOX4 alone as first-line treatment in patients with previously untreated metastatic colorectal cancer: the PRIME study. J Clin Oncol 2010;28: Douillard JY, Oliner KS, Siena S, et al. Panitumumab–FOLFOX4 Treatment and RAS Mutations in Colorectal Cancer. N Engl J Med 2013;369: Peeters M, et al. Resection Rates and Survival in Patients with Wild-Type KRAS/NRAS Metastatic Colorectal Cancer and Liver Metastases: Data from the Prime Study. EJC 2013; 49 (suppl 4):abstract MC (and poster). Peeters M, et al. EJC 2013; 49 (suppl 4):abstract MC (and poster). RAS WT, KRAS & NRAS exons 2/3/4; LLD, liver-limited disease.")
28
PRIME study RAS analysis Patient population and objective (RAS WT LLD patients, updated analysis)
LLD (n = 41) LLD (n = 48) Other only mets (n = 39) Other only mets (n = 36) Liver plus other mets (n = 172) FOLFOX4 (n = 252) First-line mCRC RAS WT (n = 505) FOLFOX4 + Panitumumab (n = 253) Liver plus other mets (n = 169) In PRIME, patients who had received no prior chemotherapy for mCRC and who had unresectable disease at baseline were randomised 1:1 to panitumumab + FOLFOX4 or FOLFOX4.1 In this exploratory analysis, data were analysed for the subgroup of patients with RAS WT mCRC and LLD to determine the following for each treatment:3 The proportion of patients achieving ≥30% tumour shrinkage/ response by week 8 and the ORR; Rates of metastasectomy and complete resection; Median PFS, OS and 3-year OS rates. These analyses included data from an exploratory analysis conducted when ≥ 80% of patients in PRIME had an OS event (updated OS analysis population).3 To determine those patients with RAS WT tumours, banked tumour samples from patients who had KRAS exon 2 WT mCRC were tested for mutations in KRAS and NRAS exon 2,3 and 4.2,3 The primary analysis population excluded patients with mutations in any of the following: KRAS and NRAS exons 2 (codons 12/13), 3 (codon 61) and 4 (codons 117/146).2 This updated exploratory analysis population also excluded patients with mutations at KRAS and NRAS exon 3 (codon 59).2,3 Data were summarised descriptively and tested for significance using Cox’s proportional hazards models and Wilcoxon two-sample test.3 REFERENCES: 1. Douillard JY, Siena S, Cassidy J, et al. Randomized, phase III trial of panitumumab with infusional fluorouracil, leucovorin, and oxaliplatin (FOLFOX4) versus FOLFOX4 alone as first-line treatment in patients with previously untreated metastatic colorectal cancer: the PRIME study. J Clin Oncol 2010;28: 2. Douillard JY, Oliner KS, Siena S, et al. Panitumumab–FOLFOX4 Treatment and RAS Mutations in Colorectal Cancer. N Engl J Med 2013;369: 3. Peeters M, et al. Resection Rates and Survival in Patients with Wild-Type KRAS/NRAS Metastatic Colorectal Cancer and Liver Metastases: Data from the Prime Study. EJC 2013; 49 (suppl 4):abstract MC (and poster). Peeters M, et al. EJC 2013; 49 (suppl 4):abstract MC (and poster). CLM, colorectal liver metastases; LLD, liver-limited disease; RAS, KRAS & NRAS exons 2/3/4.
 LLD (n = 48) Other only mets (n = 39) Other only mets (n = 36) Liver plus other mets (n = 172) FOLFOX4 (n = 252) First-line mCRC RAS WT (n = 505) FOLFOX4 + Panitumumab (n = 253) Liver plus other mets (n = 169) In PRIME, patients who had received no prior chemotherapy for mCRC and who had unresectable disease at baseline were randomised 1:1 to panitumumab + FOLFOX4 or FOLFOX4.1. In this exploratory analysis, data were analysed for the subgroup of patients with RAS WT mCRC and LLD to determine the following for each treatment:3. The proportion of patients achieving ≥30% tumour shrinkage/ response by week 8 and the ORR; Rates of metastasectomy and complete resection; Median PFS, OS and 3-year OS rates. These analyses included data from an exploratory analysis conducted when ≥ 80% of patients in PRIME had an OS event (updated OS analysis population).3. To determine those patients with RAS WT tumours, banked tumour samples from patients who had KRAS exon 2 WT mCRC were tested for mutations in KRAS and NRAS exon 2,3 and 4.2,3. The primary analysis population excluded patients with mutations in any of the following: KRAS and NRAS exons 2 (codons 12/13), 3 (codon 61) and 4 (codons 117/146).2. This updated exploratory analysis population also excluded patients with mutations at KRAS and NRAS exon 3 (codon 59).2,3. Data were summarised descriptively and tested for significance using Cox’s proportional hazards models and Wilcoxon two-sample test.3. REFERENCES: 1. Douillard JY, Siena S, Cassidy J, et al. Randomized, phase III trial of panitumumab with infusional fluorouracil, leucovorin, and oxaliplatin (FOLFOX4) versus FOLFOX4 alone as first-line treatment in patients with previously untreated metastatic colorectal cancer: the PRIME study. J Clin Oncol 2010;28: Douillard JY, Oliner KS, Siena S, et al. Panitumumab–FOLFOX4 Treatment and RAS Mutations in Colorectal Cancer. N Engl J Med 2013;369: Peeters M, et al. Resection Rates and Survival in Patients with Wild-Type KRAS/NRAS Metastatic Colorectal Cancer and Liver Metastases: Data from the Prime Study. EJC 2013; 49 (suppl 4):abstract MC (and poster). Peeters M, et al. EJC 2013; 49 (suppl 4):abstract MC (and poster). CLM, colorectal liver metastases; LLD, liver-limited disease; RAS, KRAS & NRAS exons 2/3/4.")
29
PRIME study RAS analysis Objective response and tumour shrinkage (RAS WT LLD patients, updated analysis) Objective response Tumour shrinkage ≥ 30% at wk 8# Maximum tumour shrinkage§ FOLFOX4 Panitumumab + FOLFOX4 P = 0.231 P = 0.015 P = 0.270 In patients with RAS WT mCRC and LLD, addition of panitumumab to FOLFOX4 resulted in: Numerically higher objective response Greater reduction in tumour burden at week 8 Numerically greater maximum tumour shrinkage REFERENCE: Peeters M, et al. Resection Rates and Survival in Patients with Wild-Type KRAS/NRAS Metastatic Colorectal Cancer and Liver Metastases: Data from the Prime Study. EJC 2013; 49 (suppl 4):abstract MC (and poster). n = 41 n = 48 n = 35 n = 43 n = 39 n = 46 Peeters M, et al. EJC 2013; 49 (suppl 4):abstract MC (and poster). #Patients assessed at baseline and week 8; §Patients assessed at baseline and at least one other time point; LLD, liver-limited disease; RAS, KRAS and NRAS exons 2/3/4; P-values are descriptive.
:abstract MC (and poster). n = 41. n = 48. n = 35. n = 43. n = 39. n = 46. Peeters M, et al. EJC 2013; 49 (suppl 4):abstract MC (and poster). #Patients assessed at baseline and week 8; §Patients assessed at baseline and at least one other time point; LLD, liver-limited disease; RAS, KRAS and NRAS exons 2/3/4; P-values are descriptive.")
30
Metastasectomy (all resections)
PRIME study RAS analysis Metastasectomy and complete resection rates (RAS WT, LLD patients, updated analysis) Metastasectomy (all resections) Complete resection* P = 0.349 P = 0.216 In patients with RAS WT mCRC and LLD, addition of panitumumab to FOLFOX4 resulted in numerically higher rates of metastasectomy and complete resection.. Of the patients receiving Panitumumab + FOLFOX4 (n = 48), 15 underwent metastasectomy and 14 underwent complete resection. Of the patients receiving FOLFOX4 only (n = 41), 9 underwent metastasectomy and 7 underwent complete resection. Overall 20 patients (33%) with colon cancer and four patients (14%) with rectal cancer had metastasectomies. REFERENCE: Peeters M, et al. Resection Rates and Survival in Patients with Wild-Type KRAS/NRAS Metastatic Colorectal Cancer and Liver Metastases: Data from the Prime Study. EJC 2013; 49 (suppl 4):abstract MC (and poster). FOLFOX4 (n= 41) Panitumumab + FOLFOX4 (n= 48) FOLFOX4 (n= 41) Panitumumab + FOLFOX4 (n= 48) Peeters M, et al. EJC 2013; 49 (suppl 4):abstract MC (and poster). *Subgroup of patients with metastasectomy; LLD, liver-limited disease; RAS, KRAS and NRAS exons 2/3/4; P-values are descriptive.
 Metastasectomy (all resections) Complete resection* P = P = In patients with RAS WT mCRC and LLD, addition of panitumumab to FOLFOX4 resulted in numerically higher rates of metastasectomy and complete resection.. Of the patients receiving Panitumumab + FOLFOX4 (n = 48), 15 underwent metastasectomy and 14 underwent complete resection. Of the patients receiving FOLFOX4 only (n = 41), 9 underwent metastasectomy and 7 underwent complete resection. Overall 20 patients (33%) with colon cancer and four patients (14%) with rectal cancer had metastasectomies. REFERENCE: Peeters M, et al. Resection Rates and Survival in Patients with Wild-Type KRAS/NRAS Metastatic Colorectal Cancer and Liver Metastases: Data from the Prime Study. EJC 2013; 49 (suppl 4):abstract MC (and poster). FOLFOX4. (n= 41) Panitumumab. + FOLFOX4. (n= 48) FOLFOX4. (n= 41) Panitumumab. + FOLFOX4. (n= 48) Peeters M, et al. EJC 2013; 49 (suppl 4):abstract MC (and poster). *Subgroup of patients with metastasectomy; LLD, liver-limited disease; RAS, KRAS and NRAS exons 2/3/4; P-values are descriptive.")
31
PRIME study RAS analysis PFS, OS (RAS WT, LLD patients, updated analysis)
Months 20 40 60 80 100 90 70 50 30 10 Kaplan-Meier estimate 36 4 8 12 16 28 32 24 44 48 52 20 40 60 80 100 90 70 50 30 10 Kaplan-Meier estimate Months 64 4 8 12 16 24 28 32 56 52 48 44 36 HR (95% CI) = 0.75 (0.48, 1.19) P = HR (95% CI) = 0.71 (0.43, 1.16) P = Median PFS was 1.4 months longer in patients with RAS WT mCRC and LLD receiving panitumumab + FOLFOX4 vs. FOLFOX4, but this difference was not statistically significant. Similarly, median OS was 7.3 months longer in patients with RAS WT mCRC and LLD receiving panitumumab + FOLFOX4 vs. FOLFOX4, but this difference was not statistically significant. The 3-year OS rates for patients with RAS WT mCRC and LLD receiving panitumumab + FOLFOX4 vs. FOLFOX4 were 55% vs. 44%, respectively. Overall, 3-year OS rates for patients who did and did not have a metastasectomy were 78% and 41%, respectively Overall, 3-year OS rates for patients who did and did not have a complete resection were 84% and 41%, respectively. REFERENCE: Peeters M, et al. Resection Rates and Survival in Patients with Wild-Type KRAS/NRAS Metastatic Colorectal Cancer and Liver Metastases: Data from the Prime Study. EJC 2013; 49 (suppl 4):abstract MC (and poster). Events n (%) Median OS months Panitumumab + FOLFOX4 (n = 48) 38 (79) 11.3 FOLFOX4 (n = 41) 37 (90) 9.9 Events n (%) Median OS months Panitumumab + FOLFOX4 (n = 48) 32 (67) 40.7 FOLFOX4 (n = 41) 31 (76) 33.4 Peeters M, et al. EJC 2013; 49 (suppl 4):abstract MC (and poster). LLD, liver-limited disease; PFS progression-free survival; OS, overall survival; RAS, KRAS and NRAS exons 2/3/4; P-values are descriptive.
 = 0.75 (0.48, 1.19) P = HR (95% CI) = 0.71 (0.43, 1.16) P = Median PFS was 1.4 months longer in patients with RAS WT mCRC and LLD receiving panitumumab + FOLFOX4 vs. FOLFOX4, but this difference was not statistically significant. Similarly, median OS was 7.3 months longer in patients with RAS WT mCRC and LLD receiving panitumumab + FOLFOX4 vs. FOLFOX4, but this difference was not statistically significant. The 3-year OS rates for patients with RAS WT mCRC and LLD receiving panitumumab + FOLFOX4 vs. FOLFOX4 were 55% vs. 44%, respectively. Overall, 3-year OS rates for patients who did and did not have a metastasectomy were 78% and 41%, respectively. Overall, 3-year OS rates for patients who did and did not have a complete resection were 84% and 41%, respectively. REFERENCE: Peeters M, et al. Resection Rates and Survival in Patients with Wild-Type KRAS/NRAS Metastatic Colorectal Cancer and Liver Metastases: Data from the Prime Study. EJC 2013; 49 (suppl 4):abstract MC (and poster). Events n (%) Median OS months. Panitumumab + FOLFOX4 (n = 48) 38 (79) FOLFOX4 (n = 41) 37 (90) 9.9. Events n (%) Median OS months. Panitumumab + FOLFOX4 (n = 48) 32 (67) FOLFOX4 (n = 41) 31 (76) Peeters M, et al. EJC 2013; 49 (suppl 4):abstract MC (and poster). LLD, liver-limited disease; PFS progression-free survival; OS, overall survival; RAS, KRAS and NRAS exons 2/3/4; P-values are descriptive.")
33
NEOADJUVANT BEVACIZUMAB IN LIVER METASTASES
Study Treatment Selected patients n TR (%) R0 (%) AVF 21071 B-IFL IFL No 402 45 < 2 NO B-FOLFOX B-XELOX 700 701 38 6.3 4.9 First-BEAT3 B-CT (oxali/CPT) 1914 - 9 (12/7) GONO4 B-FOLFOXIRI No (LLD) 57 (30) 77 (80) (26) TRIBE5 b-FOLFOXIRI FOLFIRI 252 256 65 53 15 (32) 12 (28) LLD CRC patients Gruenberger7 Resectable 56 73 92 BOXER6 B- XELOX non-resectable and borderline 46 78 10-40 OLIVIA8 B-FOLFOX6 non- resectable disease 41 39 80 61 49% 23% 1- Hurwitz 2004, 2- Saltz 2008, 3- Okines 2009, 4- Masi 2010, 5- Falcone 2012, 6- Wong 2011, 7- Gruenberger 2008, 8- Gruenberger 2013 33
 R0 (%) AVF B-IFL. IFL. No < 2. NO B-FOLFOX. B-XELOX First-BEAT3. B-CT (oxali/CPT) (12/7) GONO4. B-FOLFOXIRI. No (LLD) 57 (30) 77 (80) (26) TRIBE5. b-FOLFOXIRI. FOLFIRI (32) 12 (28) LLD CRC patients. Gruenberger7. Resectable BOXER6. B- XELOX. non-resectable and borderline OLIVIA8. B-FOLFOX6. non- resectable disease % 23% 1- Hurwitz 2004, 2- Saltz 2008, 3- Okines 2009, 4- Masi 2010, 5- Falcone 2012, 6- Wong 2011, 7- Gruenberger 2008, 8- Gruenberger")
34
CELIM: Tasas de Respuesta y Resección R0
All patients Cetuximab + FOLFOX6 Cetuximab + FOLFIRI KRAS wt KRAS mt n=106 n=53 n=67 n=27 CR/PR 62% 68% 57% 70% 41% 95% CI 52–72% 54–80% 42–70% 58–81% 22–61% R0 resections 34% 38% 30% 33% 25–44% 25–52% 18–44% 22–45% 14–50% Resultados del estudio: Los pacientes KRAS nativo tratados con Cetuximab + FOLFOX/FOLFIRI en el estudio CELIM obtuvieron una ORR del 70%, con una tasa de resecciones R0 del 33% Folprecht G, et al. Lancet Oncol 2010; 11: 38–47 Folprecht G, et al. EMCC 2011 (Abstract-Poster No. 6009)
")
35
POCHER: Alta tasa de respuestas y resecciones
Response rate R0 resection rate 2-year OS rate Patients (%) 79% 80 70 Patients (%) Patients (%) 60 68% 60% 50 40 30 20 10 Garufi C, Br J Cancer, 2010
 79% Patients (%) Patients (%) % 60% Garufi C, Br J Cancer,")
36
▼Panitumumab in 1st-line mCRC
Phase II trial of panitumumab plus FOLFOX4 or FOLFIRI in subjects with KRAS wild-type colorectal cancer and liver-limited disease: The PLANET study A. Abad1*, B. Massuti2, C. Grávalos3, P. Escudero4, C. Guillén-Ponce5, J.L. Manzano1, A. Gomez6, Mª J. Safont7, J. Gallego8, J. Sastre9, C. Pericay10, R. Dueñas11, C. López- López12, F. Losa13, M. Valladares14, E. González15, A. Yuste2, A. Carrato5, Enrique Aranda6 On behalf of the Spanish Cooperative Group for the Treatment of Digestive Tumors (TTD) 1.Germans Trias i Pujol Hospital –ICO, Badalona, Spain; 2. General Hospital, Alicante, Spain; 3. Doce de Octubre Hospital, Madrid, Spain; 4. Clínico Lozano Blesa Hospital, Zaragoza, Spain; 5. Universitario Ramón y Cajal Hospital, Madrid, Spain; 6. Maimonides Institute of Biomedical Research, IMIBIC, Spain, Reina Sofía Hospital, University of Córdoba. Spanish Cancer Network, (RTICC), Instituto de Salud Carlos III, Spain; 7. General Hospital, Valencia, Spain; 8. General Universitario de Elche Hospital, Alicante, Spain; 9. Hospital Clínico San Carlos, Madrid; Center affiliated to the Red Temática de Investigación Cooperativa, RD06/0020/0021, Spain, Instituto Carlos III, Spanish Ministry of Science and Innovation, Madrid; 10. Sabadell Hospital, Corporación Sanitaria Parc Taulí, Barcelona, Spain; 11. Complejo Hospitalario de Jaén Hospital, Jaén, Spain; 12. Marqués de Valdecilla Hospital, Santander, Spain; 13. General de L´Hospitalet Hospital, Barcelona, Spain; 14. Complejo Hospitalario Universitario Hospital, La Coruña, Spain; 15. Virgen de las Nieves Hospital, Granada, Spain; *actual address: Oncology Unit, Campus CIMA, Barcelona, Spain ▼ This medicinal product is subject to additional monitoring. All suspected adverse reactions should be reported
 1.Germans Trias i Pujol Hospital –ICO, Badalona, Spain; 2. General Hospital, Alicante, Spain; 3. Doce de Octubre Hospital, Madrid, Spain; 4. Clínico Lozano Blesa Hospital, Zaragoza, Spain; 5. Universitario Ramón y Cajal Hospital, Madrid, Spain; 6. Maimonides Institute of Biomedical Research, IMIBIC, Spain, Reina Sofía Hospital, University of Córdoba. Spanish Cancer Network, (RTICC), Instituto de Salud Carlos III, Spain; 7. General Hospital, Valencia, Spain; 8. General Universitario de Elche Hospital, Alicante, Spain; 9. Hospital Clínico San Carlos, Madrid; Center affiliated to the Red Temática de Investigación Cooperativa, RD06/0020/0021, Spain, Instituto Carlos III, Spanish Ministry of Science and Innovation, Madrid; 10. Sabadell Hospital, Corporación Sanitaria Parc Taulí, Barcelona, Spain; 11. Complejo Hospitalario de Jaén Hospital, Jaén, Spain; 12. Marqués de Valdecilla Hospital, Santander, Spain; 13. General de L´Hospitalet Hospital, Barcelona, Spain; 14. Complejo Hospitalario Universitario Hospital, La Coruña, Spain; 15. Virgen de las Nieves Hospital, Granada, Spain; *actual address: Oncology Unit, Campus CIMA, Barcelona, Spain. ▼ This medicinal product is subject to additional monitoring. All suspected adverse reactions should be reported.")
37
PLANET study Objectives
To evaluate the efficacy and safety of the addition of Pmab to standard CT regimens, either FOLFIRI or FOLFOX4, as first-line treatment in WT KRAS CCR patients with liver-only metastases. To explore possible differences in outcomes according to other RAS mutations.

38
PLANET study Study design
FOLFOX4 (Q2W) + panitumumab 6 mg/kg (Q2W) FOLFIRI (Q2W) + panitumumab 6 mg/kg (Q2W)) WT KRAS liver-only mCRC not suitable for initial surgery Response Rate, Resectability Rate, Safety, PFS,OS R 1:1 N=80 Sponsor: Spanish Cooperative Group for Digestive Tumour Therapy (TTD) Principal investigators: Dr. Albert Abad & Dr. Alfredo Carrato ClinicalTrials.gov identifier: NCT
 + panitumumab 6 mg/kg (Q2W) FOLFIRI (Q2W) + panitumumab 6 mg/kg (Q2W)) WT KRAS liver-only mCRC. not suitable for initial surgery. Response Rate, Resectability Rate, Safety, PFS,OS. R. 1:1. N=80. Sponsor: Spanish Cooperative Group for Digestive Tumour Therapy (TTD) Principal investigators: Dr. Albert Abad & Dr. Alfredo Carrato. ClinicalTrials.gov identifier: NCT")
39
PLANET study Endpoints
Primary Endpoint: Objective response rate (ORR) over the entire Pmab+CT treatment period Secondary Endpoints: Resection rate (R0+R1) of liver metastases Time to resection Progression-free survival (PFS) Overall survival (OS) Adverse Events (AEs) and peri-operative safety Exploratory Endpoints: Response according to molecular biomarkers (RAS status)
 over the entire Pmab+CT treatment period. Secondary Endpoints: Resection rate (R0+R1) of liver metastases. Time to resection. Progression-free survival (PFS) Overall survival (OS) Adverse Events (AEs) and peri-operative safety. Exploratory Endpoints: Response according to molecular biomarkers (RAS status)")
40
PLANET study Key eligibility criteria
>18 years of age WT KRAS CRC Synchronous or metachronous liver-only metastases deemed resectable or unresectable, meeting one of the following criteria ≥4 liver metastases ≥1 metastasis >10 cm in diameter Liver metastases not resectable No prior anti-EGFR therapy Karnofsky performance status ≥70% Adequate haematologic, renal and metabolic function Key inclusion criteria: >18 years of age WT KRAS CRC with at least one unidimensionally measurable lesion ≥20 mm with the conventional techniques (computed tomography (CT), magnetic resonance imaging) or >10 mm with spiral CT, according to the modified RECIST criteria (Version 1.1). Synchronous or metachronous liver-only metastases deemed resectable or unresectable, including those patients who had undergone complete resection (R0) of the primary tumour at least 4 weeks before randomisation, fulfilling one of the following criteria: ≥4 liver metastases at least 1 metastasis >10 cm in diameter Liver metastases technically not resectable (vascular compromise and/or location in which complete resection is impossible and/or 25-30% of healthy liver would not remain functional after resection) Patients with either: Recurrence after adjuvant treatment with 5- fluorouracil/folinic acid or capecitabine +/- radiotherapy with a disease-free interval >6 months; or after oxaliplatin containing adjuvant treatment with a disease-free interval >12 months Recurrence after surgical treatment and/or radiotherapy with no adjuvant systemic treatment. De novo diagnosis No major contra-indication to liver surgery Karnofsky performance status ≥70% Adequate bone marrow function: neutrophils ≥1.5 x109/ L; platelets ≥100 x109/L; hemoglobin ≥9 g/dL Hepatic and metabolic function as follows: Total bilirubin count ≤1.5 x upper limit of normal (ULN) and not increasing >25% within the last 4 weeks; ALT and AST <5 x ULN Renal function, calculated as creatinine clearance or 24-hour creatinine clearance ≥50 mL/min Magnesium > lower limit of normal Key exclusion criteria: Prior anti-EGFr antibody therapy (e.g., cetuximab) or treatment with small molecule EGFr tyrosine kinase inhibitors (e.g., erlotinib).Subjects who have experienced an infusion reaction to their first dose of anti-EGFR therapy (cetuximab) may participate in this clinical trial Hormonal therapy, immunotherapy or experimental or approved proteins/antibodies (e.g., bevacizumab) ≤ 30 days before inclusion Surgery (not including diagnostic biopsy or central venous catheter placement) and/or radiotherapy in the 4 weeks prior to inclusion Metastasis on any site other than the liver, including extrahepatic lymph nodes. Active disease or treatment for prior malignant tumour in the last 5 years, except a history of basal cell carcinoma or cervical carcinoma in situ Significant cardiovascular disease including unstable angina or myocardial infarction within 12 months before initiating study treatment or a history of ventricular arrhythmia Known positive test for human immunodeficiency virus infection, hepatitis C virus, chronic active hepatitis B infection Reference: Abad A, Massuti B, Grávalos C, et al. Phase II trial of panitumumab plus FOLFOX4 or FOLFIRI in subjects with KRAS wild-type colorectal cancer and liver-limited disease: The PLANET study. J Clin Oncol 2014; 32:5s (suppl):abstract 3560 (and poster). Abad A, et al. J Clin Oncol 2014; 32:5s (suppl):abstract 3560 (and poster). EGFR, epidermal growth factor receptor
, magnetic resonance imaging) or >10 mm with spiral CT, according to the modified RECIST criteria (Version 1.1). Synchronous or metachronous liver-only metastases deemed resectable or unresectable, including those patients who had undergone complete resection (R0) of the primary tumour at least 4 weeks before randomisation, fulfilling one of the following criteria: ≥4 liver metastases. at least 1 metastasis >10 cm in diameter. Liver metastases technically not resectable (vascular compromise and/or location in which complete resection is impossible and/or 25-30% of healthy liver would not remain functional after resection) Patients with either: Recurrence after adjuvant treatment with 5- fluorouracil/folinic acid or capecitabine +/- radiotherapy with a disease-free interval >6 months; or after oxaliplatin containing adjuvant treatment with a disease-free interval >12 months. Recurrence after surgical treatment and/or radiotherapy with no adjuvant systemic treatment. De novo diagnosis. No major contra-indication to liver surgery. Karnofsky performance status ≥70% Adequate bone marrow function: neutrophils ≥1.5 x109/ L; platelets ≥100 x109/L; hemoglobin ≥9 g/dL. Hepatic and metabolic function as follows: Total bilirubin count ≤1.5 x upper limit of normal (ULN) and not increasing >25% within the last 4 weeks; ALT and AST <5 x ULN. Renal function, calculated as creatinine clearance or 24-hour creatinine clearance ≥50 mL/min. Magnesium > lower limit of normal. Key exclusion criteria: Prior anti-EGFr antibody therapy (e.g., cetuximab) or treatment with small molecule EGFr tyrosine kinase inhibitors (e.g., erlotinib).Subjects who have experienced an infusion reaction to their first dose of anti-EGFR therapy (cetuximab) may participate in this clinical trial. Hormonal therapy, immunotherapy or experimental or approved proteins/antibodies (e.g., bevacizumab) ≤ 30 days before inclusion. Surgery (not including diagnostic biopsy or central venous catheter placement) and/or radiotherapy in the 4 weeks prior to inclusion. Metastasis on any site other than the liver, including extrahepatic lymph nodes. Active disease or treatment for prior malignant tumour in the last 5 years, except a history of basal cell carcinoma or cervical carcinoma in situ. Significant cardiovascular disease including unstable angina or myocardial infarction within 12 months before initiating study treatment or a history of ventricular arrhythmia. Known positive test for human immunodeficiency virus infection, hepatitis C virus, chronic active hepatitis B infection. Reference: Abad A, Massuti B, Grávalos C, et al. Phase II trial of panitumumab plus FOLFOX4 or FOLFIRI in subjects with KRAS wild-type colorectal cancer and liver-limited disease: The PLANET study. J Clin Oncol 2014; 32:5s (suppl):abstract 3560 (and poster). Abad A, et al. J Clin Oncol 2014; 32:5s (suppl):abstract 3560 (and poster). EGFR, epidermal growth factor receptor.")
41
PLANET study Patient disposition and characteristics
77 patients were analyzed 38 received Pmab-FOLFOX4 39 received Pmab-FOLFIRI Pmab-FOLFOX4 (N = 38) Pmab-FOLFIRI (N = 39) TOTAL (N = 77) Male, n (%) 31 (81.6) 28 (71.8) 59 (76.6) Median age, years (min, max) 65 (32, 79) 63 (37, 83) 64 (32, 83) Mean body mass index, kg/m2 (SD) 27.4 (4.4) 25.9 (3.6) 26.7 (4.0) Median time since CCR diagnosis, months (Q1, Q3) 3.4 (1.3, 22.7) 1.6 (0.6, 11,5) 1.9 (0.6, 22.2) Technically resectable liver metastases, n (%) 12 (31.6) 12 (30.8) 24 (31.2) Prior surgery for primary tumor, n (%) 26 (68.4) 22 (56.4) 48 (62.3) Prior adjuvant/neoadjuvant CT and/or radiotherapy, n (%) 6 (15.8) 4 (10.3) 10 (13.0) Prior FOLFOX, n (%) 3 (7.9) 3 (7.7) 6 (7.8) Abad et al. Presented at the 16th World Congress on Gastrointestinal Cancer, June 25-28, 2014, Barcelona (Spain); Abstract nº PD-0006
 Pmab-FOLFIRI. (N = 39) TOTAL. (N = 77) Male, n (%) 31 (81.6) 28 (71.8) 59 (76.6) Median age, years (min, max) 65 (32, 79) 63 (37, 83) 64 (32, 83) Mean body mass index, kg/m2 (SD) 27.4 (4.4) 25.9 (3.6) 26.7 (4.0) Median time since CCR diagnosis, months (Q1, Q3) 3.4 (1.3, 22.7) 1.6 (0.6, 11,5) 1.9. (0.6, 22.2) Technically resectable liver metastases, n (%) 12 (31.6) 12 (30.8) 24 (31.2) Prior surgery for primary tumor, n (%) 26 (68.4) 22 (56.4) 48 (62.3) Prior adjuvant/neoadjuvant CT and/or radiotherapy, n (%) 6 (15.8) 4 (10.3) 10 (13.0) Prior FOLFOX, n (%) 3 (7.9) 3 (7.7) 6 (7.8) Abad et al. Presented at the 16th World Congress on Gastrointestinal Cancer, June 25-28, 2014, Barcelona (Spain); Abstract nº PD")
42
PLANET study Response rate and resectability – presented a ESMO
Preliminary median OS in WT KRAS (exon 2) was 32.5 and 42.4 months (p = 0.848). Median OS in WT RAS was 39.0 months with pmab + FOLFOX4 and 45.8 months withp+ FOLFIRI. Reference: Abad A, Massuti B, Grávalos C, et al. Phase II trial of panitumumab plus FOLFOX4 or FOLFIRI in subjects with KRAS wild-type colorectal cancer and liver-limited disease: The PLANET study. J Clin Oncol 2014; 32:5s (suppl):abstract 3560 (and poster).
 was 32.5 and 42.4 months (p = 0.848). Median OS in WT RAS was 39.0 months with pmab + FOLFOX4 and 45.8 months withp+ FOLFIRI. Reference: Abad A, Massuti B, Grávalos C, et al. Phase II trial of panitumumab plus FOLFOX4 or FOLFIRI in subjects with KRAS wild-type colorectal cancer and liver-limited disease: The PLANET study. J Clin Oncol 2014; 32:5s (suppl):abstract 3560 (and poster).")
43
PLANET study OS WT KRAS exon 2 WT RAS Median, months (95% CI)
100 100 90 90 80 80 70 70 60 60 Proportion event-free (%) 50 Proportion event-free (%) 50 40 40 30 30 20 P log rank = 0.848 P Wilcoxon = 0.915 20 P log-rank = 0.935 P Wilcoxon = 0.634 10 10 10 20 30 40 50 60 10 20 30 40 50 Months Months Preliminary median OS in WT KRAS (exon 2) was 32.5 and 42.4 months (p = 0.848). Median OS in WT RAS was 39.0 months with pmab + FOLFOX4 and 45.8 months withp+ FOLFIRI. Reference: Abad A, Massuti B, Grávalos C, et al. Phase II trial of panitumumab plus FOLFOX4 or FOLFIRI in subjects with KRAS wild-type colorectal cancer and liver-limited disease: The PLANET study. J Clin Oncol 2014; 32:5s (suppl):abstract 3560 (and poster). Median, months (95% CI) Panitumumab + FOLFOX4 32.5 (20.6–NA) Panitumumab + FOLFIRI 42.4 (17.8–51.5) Median, months (95% CI) Panitumumab + FOLFOX4 39.0 (26.4–NA) Panitumumab + FOLFIRI 45.8 (32.8–51.5) Abad A, et al. J Clin Oncol 2014; 32:5s (suppl):abstract 3560 (and poster). WT RAS, WT KRAS & NRAS exons 2/3/4; NA, not achieved
 50. Proportion event-free (%) P log rank = P Wilcoxon = P log-rank = P Wilcoxon = Months. Months. Preliminary median OS in WT KRAS (exon 2) was 32.5 and 42.4 months (p = 0.848). Median OS in WT RAS was 39.0 months with pmab + FOLFOX4 and 45.8 months withp+ FOLFIRI. Reference: Abad A, Massuti B, Grávalos C, et al. Phase II trial of panitumumab plus FOLFOX4 or FOLFIRI in subjects with KRAS wild-type colorectal cancer and liver-limited disease: The PLANET study. J Clin Oncol 2014; 32:5s (suppl):abstract 3560 (and poster). Median, months. (95% CI) Panitumumab + FOLFOX (20.6–NA) Panitumumab + FOLFIRI (17.8–51.5) Median, months. (95% CI) Panitumumab + FOLFOX (26.4–NA) Panitumumab + FOLFIRI (32.8–51.5) Abad A, et al. J Clin Oncol 2014; 32:5s (suppl):abstract 3560 (and poster). WT RAS, WT KRAS & NRAS exons 2/3/4; NA, not achieved.")
44
ESMO Clinical Groups for 1st-line treatment Definition of Group 0 (initially resectable) patients
Initially R0 resectable Non-resectable at clinical presentation Group 2 Group 1 Group 3 Group 0 Metastases are: Limited to liver and / or lung Clearly R0-resectable, even without preoperative chemotherapy Treatment aim is curative and to decrease risk of relapse Group 0: This group comprises those patients in whom metastases are limited to liver/lung metastases, which are clearly R0 resectable even without preoperative chemotherapy This group is different from Group 1, where upfront resection has a high likelihood for a R ≥ 1 resection REFERENCE: Schmoll HJ, Van Cutsem E, Stein A, et al. ESMO Consensus Guidelines for management of patients with colon and rectal cancer. A personalized approach to clinical decision making. Ann Oncol 2012;23: Schmoll HJ, et al. Ann Oncol 2012; 23: R0, resection with microscopically negative margins.

45
initially resectable LLD
EORTC intergroup study [EPOC] Surgery ± FOLFOX4 for resectable liver metastases from colorectal cancer Open label, phase 3 study FOLFOX4 6 cycles S U R G E Y FOLFOX4 6 cycles mCRC with initially resectable LLD (n = 364) R 1:1 None None Study objectives: To compare the progression-free and overall survival of patients with resectable colorectal liver metastases treated with surgery with or without neoadjuvant and adjuvant oxaliplatin, fluorouracil, and leucovorin calcium. To compare the percentage of patients with total resection with these two treatments. Selected inclusion criteria: WHO ≤ 2 1-4 resectable liver metastases No detectable extra-hepatic tumours Primary tumour either already (R0) resected or judged to be resectable (in case of synchronous metastases). No previous chemotherapy with oxaliplatin. REFERENCE: Nordlinger B, Sorbye H, Glimelius B, et al. Perioperative chemotherapy with FOLFOX4 and surgery versus surgery alone for resectable liver metastases from colorectal cancer (EORTC Intergroup trial 40983): a randomised controlled trial. Lancet 2008;371: Study endpoints: PFS (1°), OS, resectability, tumour response, safety ClinicalTrials.gov identifier: NCT Nordlinger B, et al. Lancet 2008; 371: ; Nordlinger B, et al. Lancet 2013; 14: mCRC metastatic colorectal cancer; LLD, liver limited disease; OS, overall survival; PFS, progression free survival.
 R. 1:1. None. None. Study objectives: To compare the progression-free and overall survival of patients with resectable colorectal liver metastases treated with surgery with or without neoadjuvant and adjuvant oxaliplatin, fluorouracil, and leucovorin calcium. To compare the percentage of patients with total resection with these two treatments. Selected inclusion criteria: WHO ≤ resectable liver metastases. No detectable extra-hepatic tumours. Primary tumour either already (R0) resected or judged to be resectable (in case of synchronous metastases). No previous chemotherapy with oxaliplatin. REFERENCE: Nordlinger B, Sorbye H, Glimelius B, et al. Perioperative chemotherapy with FOLFOX4 and surgery versus surgery alone for resectable liver metastases from colorectal cancer (EORTC Intergroup trial 40983): a randomised controlled trial. Lancet 2008;371: Study endpoints: PFS (1°), OS, resectability, tumour response, safety. ClinicalTrials.gov identifier: NCT Nordlinger B, et al. Lancet 2008; 371: ; Nordlinger B, et al. Lancet 2013; 14: mCRC metastatic colorectal cancer; LLD, liver limited disease; OS, overall survival; PFS, progression free survival.")
46
EORTC intergroup study 40983 [EPOC] Progression free survival
All eligible patients All resected patients 100 100 HR (96% CI) = 0.77 (0.60, 1.00) P = 0.041 HR (96% CI) = 0.73 (0.55, 0.97) P = 0.025 80 80 60 60 Proportion event-free (%) Proportion event-free (%) 40 40 20 20 1 2 3 4 5 6 1 2 3 4 5 6 3-year PFS, % Surgery + FOLFOX4 (n = 171) 36.2 Surgery (n = 171) 28.1 3-year PFS, % Surgery + FOLFOX4 (n = 151) 42.4 Surgery (n = 152) 33.2 Years Years This slide represents the trial’s final data for PFS, which were published1 while overall survival was still being monitored.2 The combination of perioperative chemotherapy with FOLFOX4 (folinic acid, fluorouracil, and oxaliplatin) and surgery increased progression-free survival (PFS) compared with surgery alone for patients with liver-only metastases from colorectal cancer deemed resectable on preoperative imaging. For all patients eligible for analysis (ie, those who were assessed by the study coordinator to fulfil eligibility criteria as defined in the protocol) the absolute difference in 3-year PFS was 8·1% (28·1% [95·66% CI 21·2 – 36·6] in the surgery-only group vs 36·2% [28·7 – 43·8] in the perioperative chemotherapy group; HR 0·77 [0·60 – 1·00]; p=0·041). Data from a median follow-up of 8.5 years reported the estimated 3-year PFS in all eligible patients to be:2 29.9% [95% CI 23·2 – 36·9] in the surgery-only group vs. 39.0% [95% CI 31.7 – 46.3] in the perioperative chemotherapy group; HR 0·78 [0·61 – 0·99]; p=0·035). REFERENCES: 1. Nordlinger B, Sorbye H, Glimelius B, et al. Perioperative chemotherapy with FOLFOX4 and surgery versus surgery alone for resectable liver metastases from colorectal cancer (EORTC Intergroup trial 40983): a randomised controlled trial. Lancet 2008;371: 2. Nordlinger B, et al. Perioperative FOLFOX4 chemotherapy and surgery versus surgery alone for resectable liver metastases from colorectal cancer (EORTC 40983): long-term results of a randomised, controlled, phase 3 trial. Lancet 2013; 14: Perioperative FOLFOX4 reduced the risk of PFS events by ~25% Nordlinger B, et al. Lancet 2008; 371: PFS, progression free survival.
![EORTC intergroup study [EPOC] Progression free survival](http://slideplayer.com/slide/3227633/11/images/46/EORTC+intergroup+study+%5BEPOC%5D+Progression+free+survival.jpg "All eligible patients. All resected patients HR (96% CI) = 0.77 (0.60, 1.00) P = HR (96% CI) = 0.73 (0.55, 0.97) P = Proportion event-free (%) Proportion event-free (%) year PFS, % Surgery + FOLFOX4 (n = 171) Surgery (n = 171) year PFS, % Surgery + FOLFOX4 (n = 151) Surgery (n = 152) Years. Years. This slide represents the trial’s final data for PFS, which were published1 while overall survival was still being monitored.2. The combination of perioperative chemotherapy with FOLFOX4 (folinic acid, fluorouracil, and oxaliplatin) and surgery increased progression-free survival (PFS) compared with surgery alone for patients with liver-only metastases from colorectal cancer deemed resectable on preoperative imaging. For all patients eligible for analysis (ie, those who were assessed by the study coordinator to fulfil eligibility criteria as defined in the protocol) the absolute difference in 3-year PFS was 8·1% (28·1% [95·66% CI 21·2 – 36·6] in the surgery-only group vs 36·2% [28·7 – 43·8] in the perioperative chemotherapy group; HR 0·77 [0·60 – 1·00]; p=0·041). Data from a median follow-up of 8.5 years reported the estimated 3-year PFS in all eligible patients to be: % [95% CI 23·2 – 36·9] in the surgery-only group vs. 39.0% [95% CI 31.7 – 46.3] in the perioperative chemotherapy group; HR 0·78 [0·61 – 0·99]; p=0·035). REFERENCES: 1. Nordlinger B, Sorbye H, Glimelius B, et al. Perioperative chemotherapy with FOLFOX4 and surgery versus surgery alone for resectable liver metastases from colorectal cancer (EORTC Intergroup trial 40983): a randomised controlled trial. Lancet 2008;371: Nordlinger B, et al. Perioperative FOLFOX4 chemotherapy and surgery versus surgery alone for resectable liver metastases from colorectal cancer (EORTC 40983): long-term results of a randomised, controlled, phase 3 trial. Lancet 2013; 14: Perioperative FOLFOX4 reduced the risk of PFS events by ~25% Nordlinger B, et al. Lancet 2008; 371: PFS, progression free survival.")
47
20100086 EORTC BOS-2 study Patients with resectable liver metastases
Open label, phase 2 study 6 cycles mFOLFOX6 mFOLFOX6 + bevacizumab panitumumab S U R G E Y 6 cycles mFOLFOX6 mFOLFOX6 + bevacizumab panitumumab F O L W - U P KRAS WT mCRC with resectable LLD (n = 360) CRC with ≤8 resectable metachronous or synchronous liver metastases from CRC KRAS wild-type R The addition of targeted agents to standard FOLFOX chemotherapy in the perioperative strategy for mCRC might increase the ORR and R0 resectability, without significant increase in toxicity, therefore translating to a better outcome. To test this, the European Organisation for Research and Treatment of Cancer (EORTC) has designed an open label, randomized, multi-centre, 3-arm late phase II study. Selected inclusion criteria: WHO 0 or 1 Histologically proven CRC with 1 to 8 metachronous or synchronous liver metastases considered to be completely resectable. No detectable extra-hepatic tumours. Primary tumour either already (R0) resected or judged to be resectable at the same time as the liver metastases (in case of synchronous metastases). Primary tumour (or liver metastasis) of CRC must be KRAS status "wild type". No previous chemotherapy for metastatic disease or surgical treatment for liver metastases. No exposure to EGFR or VEGF/VEGFR targeting therapy in the last 12 months. REFERENCE: ClinicalTrials.gov identifier: NCT Study endpoints: PFS (1°), pathological response rate, resection rate, OS, safety ClinicalTrials.gov identifier: NCT BOS, biologics, oxaliplatin and surgery, OS, overall survival.
 CRC with ≤8 resectable metachronous or synchronous liver metastases from CRC. KRAS wild-type. R. The addition of targeted agents to standard FOLFOX chemotherapy in the perioperative strategy for mCRC might increase the ORR and R0 resectability, without significant increase in toxicity, therefore translating to a better outcome. To test this, the European Organisation for Research and Treatment of Cancer (EORTC) has designed an open label, randomized, multi-centre, 3-arm late phase II study. Selected inclusion criteria: WHO 0 or 1. Histologically proven CRC with 1 to 8 metachronous or synchronous liver metastases considered to be completely resectable. No detectable extra-hepatic tumours. Primary tumour either already (R0) resected or judged to be resectable at the same time as the liver metastases (in case of synchronous metastases). Primary tumour (or liver metastasis) of CRC must be KRAS status wild type . No previous chemotherapy for metastatic disease or surgical treatment for liver metastases. No exposure to EGFR or VEGF/VEGFR targeting therapy in the last 12 months. REFERENCE: ClinicalTrials.gov identifier: NCT Study endpoints: PFS (1°), pathological response rate, resection rate, OS, safety. ClinicalTrials.gov identifier: NCT BOS, biologics, oxaliplatin and surgery, OS, overall survival.")
48
Conclusiones El CCRm tiene mal pronóstico si no se trata.
La cirugía hepática ofrece posibilidad de curación (15%) Hasta un 30% de los tumnores inicialmente irresecables se convierten en resecables tras QT de conversión Las combinaciones de quimioterapia con tratamientos biológicos ofrecen tasas de respuestas superiores a 50% en pacientes no seleccionados, y superiores a 70% en pacientes con enfermedad limitada al hígado. Los datos de los estudios fase III (PRIME), y los estudios de los estudios fase II con pacientes seleccionados (PLANET), permiten emular los resultados de otras combinaciones REFERENCES: 1. Van den Eynde M, Hendlisz A. Treatment of colorectal liver metastases: a review. Rev Recent Clin Trials 2009;4:56–62. 2. Nordlinger B et al. Does chemotherapy prior to liver resection increase the potential for cure in patients with metastatic colorectal cancer? A report from the European Colorectal Metastases Treatment Group. Eur J Cancer. 2007;43(14):2037–45. 3. Schmoll HJ, Van Cutsem E, Stein A, et al. ESMO Consensus Guidelines for management of patients with colon and rectal cancer. A personalized approach to clinical decision making. Ann Oncol 2012;23: 4. Peeters M, et al. Resection Rates and Survival in Patients with Wild-Type KRAS/NRAS Metastatic Colorectal Cancer and Liver Metastases: Data from the Prime Study. EJC 2013; 49 (suppl 4):abstract MC (and poster)
 Hasta un 30% de los tumnores inicialmente irresecables se convierten en resecables tras QT de conversión. Las combinaciones de quimioterapia con tratamientos biológicos ofrecen tasas de respuestas superiores a 50% en pacientes no seleccionados, y superiores a 70% en pacientes con enfermedad limitada al hígado. Los datos de los estudios fase III (PRIME), y los estudios de los estudios fase II con pacientes seleccionados (PLANET), permiten emular los resultados de otras combinaciones. REFERENCES: 1. Van den Eynde M, Hendlisz A. Treatment of colorectal liver metastases: a review. Rev Recent Clin Trials 2009;4:56– Nordlinger B et al. Does chemotherapy prior to liver resection increase the potential for cure in patients with metastatic colorectal cancer A report from the European Colorectal Metastases Treatment Group. Eur J Cancer. 2007;43(14):2037– Schmoll HJ, Van Cutsem E, Stein A, et al. ESMO Consensus Guidelines for management of patients with colon and rectal cancer. A personalized approach to clinical decision making. Ann Oncol 2012;23: Peeters M, et al. Resection Rates and Survival in Patients with Wild-Type KRAS/NRAS Metastatic Colorectal Cancer and Liver Metastases: Data from the Prime Study. EJC 2013; 49 (suppl 4):abstract MC (and poster)")
49
Conclusiones Cuando hablemos del tratamiento de conversión en pacientes afectos de CCRm potencialmente resecables, las combinaciones con panitumumab han demostrado ser igualmente eficaces que otras combinaciones de tratamiento estudiadas con anterioridad. REFERENCES: 1. Van den Eynde M, Hendlisz A. Treatment of colorectal liver metastases: a review. Rev Recent Clin Trials 2009;4:56–62. 2. Nordlinger B et al. Does chemotherapy prior to liver resection increase the potential for cure in patients with metastatic colorectal cancer? A report from the European Colorectal Metastases Treatment Group. Eur J Cancer. 2007;43(14):2037–45. 3. Schmoll HJ, Van Cutsem E, Stein A, et al. ESMO Consensus Guidelines for management of patients with colon and rectal cancer. A personalized approach to clinical decision making. Ann Oncol 2012;23: 4. Peeters M, et al. Resection Rates and Survival in Patients with Wild-Type KRAS/NRAS Metastatic Colorectal Cancer and Liver Metastases: Data from the Prime Study. EJC 2013; 49 (suppl 4):abstract MC (and poster)
:2037– Schmoll HJ, Van Cutsem E, Stein A, et al. ESMO Consensus Guidelines for management of patients with colon and rectal cancer. A personalized approach to clinical decision making. Ann Oncol 2012;23: Peeters M, et al. Resection Rates and Survival in Patients with Wild-Type KRAS/NRAS Metastatic Colorectal Cancer and Liver Metastases: Data from the Prime Study. EJC 2013; 49 (suppl 4):abstract MC (and poster)")
Similar presentations
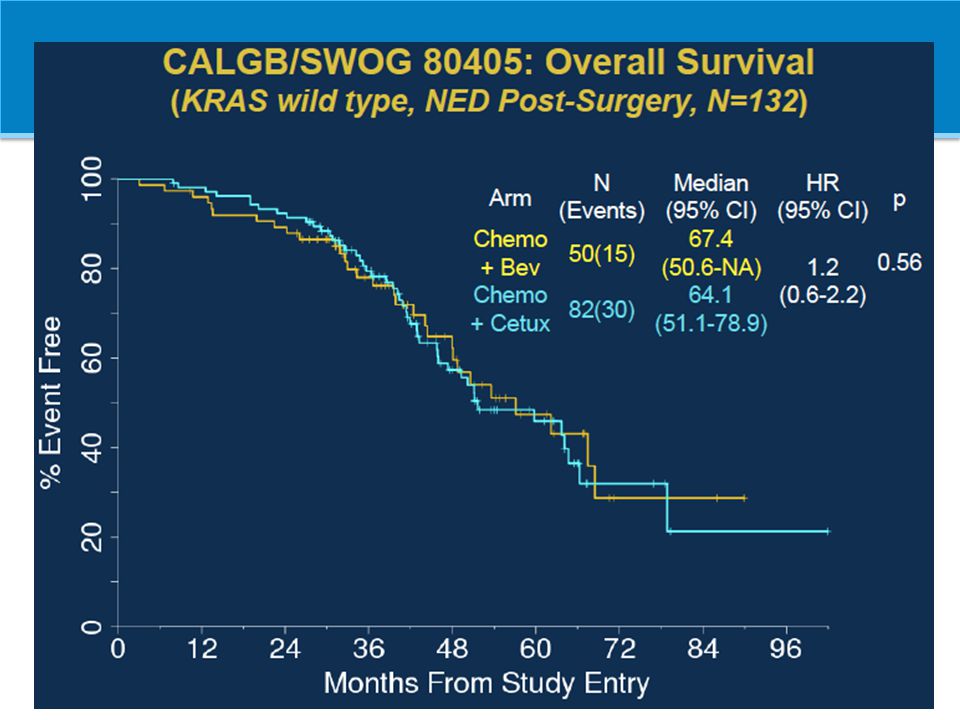













 patients Policy.>")





