Download presentation
Presentation is loading. Please wait.

1
Stroke Systems of Care V.T. Doss, D.O.
Stroke Medical Director, BMH-Memphis Assistant Professor, Neurology & Neurosurgery, UTHSC

2
Intro Neurological emergency Ischemic vs. Hemorrhagic
TOAST classification thrombosis /embolism due to atherosclerosis of a large artery cardioembolic origin occlusion of a small blood vessel other determined cause (CSVT, vasculitis, trauma) undetermined cause (two possible causes, no cause identified, or incomplete investigation) thrombosis or embolism due to atherosclerosis of a large artery, (2) embolism of cardiac origin, (3) occlusion of a small blood vessel, (4) other determined cause (5) undetermined cause (two possible causes, no cause identified, or incomplete investigation).
 undetermined cause (two possible causes, no cause identified, or incomplete investigation) thrombosis or embolism due to atherosclerosis of a large artery, (2) embolism of cardiac origin, (3) occlusion of a small blood vessel, (4) other determined cause (5) undetermined cause (two possible causes, no cause identified, or incomplete investigation).")
3
Memphis- the capitol of atherosclerosis?

4
Stroke death rates, 2000–2006: adults ≥35 years of age, by county.
Stroke death rates, 2000–2006: adults ≥35 years of age, by county. Rates are spatially smoothed to enhance the stability of rates in counties with small populations. International Classification of Diseases, 10th Revision codes for stroke: I60–I69. Data source: National Vital Statistics System and the US Census Bureau. Writing Group Members et al. Circulation 2012;125:e2-e220 Copyright © American Heart Association

5
US Stats 95% of strokes at age >45, and 2/3 of strokes occur in those >65 leading cause death/disability 10% deaths worldwide 795,000 strokes/yr, 610,000 of these are first strokes. About 185,000 people who survive a stroke go on to have another In 2010, stroke cost the US $53.9 billion Someone in the United States has a stroke every 40 seconds. Every four minutes someone dies of stroke This total includes the cost of health care services, medications, and missed days of work. Compared to whites, African Americans are at nearly twice the risk of having a first stroke. Hispanic Americans' risk falls between the two. Moreover, African Americans and Hispanics are more likely to die following a stroke than are whites. SE has highest mortality rates

6
According to the WHO, 15 million people suffer stroke worldwide each year.
Of these, 5 million die and another 5 million are permanently disabled. Stroke is the second single most common cause of death in Europe: accounting for almost 1.1 million deaths each year. Over one in seven women (15%) and one in ten men (10%) die from the disease.
 and one in ten men (10%) die from the disease.")
7
Why is Time Important? The area peripheral to a core infarct where metabolism is active but blood flow is diminished is called the ischemic penumbra This is salvageable tissue that is at risk for infarction. The penumbra lies in a 'no-man's land' between a zone of low blood flow that is < 25 ml/100 mg brain tissue/min and a zone where brain tissue is undergoing necrosis/death, flow of < 8-10 ml/100 mg/min1 Without restoration of blood flow/oxygen, the ischemic penumbra will convert to ischemic core or tissue death Core Infarct Ischemic Penumbra Brain 1-

8
Time is Brain !! Neurology Dec 12;55(11):
:")
9
IV TPA APPROVED by FDA in 1996
NOW THE ACCEPTED STANDARD OF CARE THROUGHOUT US, EUROPE AND ASIA RPCT – TPA v. Placebo < 3 hours (Dose .9mg/kg IV) Inclusion Criteria: Stroke with clear time of onset, CT without ICH, & measurable deficit on NIHSS Exclusion Criteria: Recent GI or GU Bleed w/in 21 days, Ischemic stroke within 3 months,hx of ICH, recent arterial puncture at a noncompressible site w/in 7 days, SBP > 185 or DBP > 110 that can’t be controlled, INR > 1.5, platelets < 100K, glucose > 400 or < 50 Seizure at onset Phase I (N=291): TPA clinical 24 hours NIHSS improvement of >/= 4 47% TPA vs. 39% placebo, p= 0.21 Phase II (N=333): Primary Outcomes (MRS < 2) at 90 days, ARR 12%, NNT = 8 SICH 6.4 % vs % (P < 0.001)
 Inclusion Criteria: Stroke with clear time of onset, CT without ICH, & measurable deficit on NIHSS. Exclusion Criteria: Recent GI or GU Bleed w/in 21 days, Ischemic stroke within 3 months,hx of ICH, recent arterial puncture at a noncompressible site w/in 7 days, SBP > 185 or DBP > 110 that can’t be controlled, INR > 1.5, platelets < 100K, glucose > 400 or < 50 Seizure at onset. Phase I (N=291): TPA clinical 24 hours NIHSS improvement of >/= 4. 47% TPA vs. 39% placebo, p= Phase II (N=333): Primary Outcomes (MRS < 2) at 90 days, ARR 12%, NNT = 8. SICH 6.4 % vs. 0.6 % (P < 0.001)")
10
Number Needed to Treat = 14
Expanded time window for milder strokes, NIHHS < 25 with less than 1/3 of MCA territory on CT N=821 Primary endpoint: MRS < 90 days. 52.4% vs. 45.2, P = 0.04 Number Needed to Treat = 14

11
Modified Rankin Scale 0 - No symptoms.
1 - No significant disability. Able to carry out all usual activities, despite some symptoms. 2 - Slight disability. Able to look after own affairs without assistance, but unable to carry out all previous activities. 3 - Moderate disability. Requires some help, but able to walk unassisted. 4 - Moderately severe disability. Unable to attend to own bodily needs without assistance, and unable to walk unassisted. 5 - Severe disability. Requires constant nursing care and attention, bedridden, incontinent. 6 - Dead.

12
NINDS NINDS randomized 624 subjects within 3 hours of stroke onset to receive 0.9 mg/kg of intravenous tPA or placebo found that patients treated with tPA within 3 hours of onset had a substantially better chance of functional independence with minimal or no disability 3 months after treatment The proportion of patients with minimal or no disability increased from 38% with placebo to 50% with tPA, a 12% absolute improvement The NNT for 1 more patient to have a normal or near normal outcome was 8 NNT for 1 more patient to have an improved outcome was 3.1 Brain hemorrhages related to tPA caused severe worsened final outcome in 1% of patients Overall, for every 100 patients treated within the first 3 hours, 32 had a better outcome as a result and 3 had a worse outcome.

13
ECASS III 821 pts, hr no difference in mortality between the two groups (approximately 8%) sICH higher in tpa group (2.4%) odds for a favorable outcome (MRS 0-1) after stroke were 28% higher with alteplase than with placebo Time is tissue
 odds for a favorable outcome (MRS 0-1) after stroke were 28% higher with alteplase than with placebo. Time is tissue.")
14
NINDS and ACLS Recommended Benchmarks for Potential Thrombolysis Candidate
Interval Target Door to doctor 10 min Access to neuro expertise 15 min Door to CT completion 25 min Door to CT interpretation 45 min Door to IV-rTPA 60 min Admission to stroke unit or ICU 3 hours

15
Casting a wider net Expanding time window
Stroke centers- primary, comprehensive Tele-stroke Multi-modal imaging New agents/devices Less is more? Neuroprotection

16
Direction/Innovations
EMS Advances Telemedicine Spoke and Hub Models

18
Tele-Stroke 24hr access to neuro specialist Avoids stroke mimickers
Allows smaller hospitals to keep these patients

19
CSC Physicians Vascular Neurology Vascular Neurosurgery
Infrastructure Stroke Unit Intensive Care Unit Operating room staffed 24/7 Interventional staff available 24/7 Stroke registry Diagnostic techniques MRI with diffusion MRA and MRV Computed Tomography Angiogram (CTA) Digital cerebral angiography Transcranial dopplers Carotid duplex ultrasound TTE and TEE Rehabilitation (PT/OT/ST) Advanced Practice Nursing /Staff stroke nurses Respiratory Therapists Educational/research programs Clinical research Community education/prevention Professional education Physicians Vascular Neurology Vascular Neurosurgery Vascular Surgery Diagnostic radiology and neuroradiology Interventional/endovascular physicians Critical care medicine Physiatrists Surgical and interventional therapies CEA Intracranial aneurysm clipping Surgical removal or draining of blood from the brain Placement of EVD and intracranial pressure monitors Endovascular treatment of aneurysms and arteriovenous malformations Intra-arterial reperfusion therapy Endovascular treatment of vasospasm PSCs certified within the past 2 years, 72.7% of eligible patients received tPA. The longer a PSC was in the certification program, the higher its tPA participation rate. Hospitals in their second certification cycle achieved a 78.6% IV tPA participation rate, and those certified for a third 2-year cycle achieved 94.4% participation. Among teaching hospitals in their first certification cycle, the rate of IV tPA use for eligible patients was 81% compared with 70% of nonteaching hospitals. Most studies have found Tx at PSC you’re more likely to have a better outcome and lower mortality.
 Digital cerebral angiography. Transcranial dopplers. Carotid duplex ultrasound. TTE and TEE. Rehabilitation (PT/OT/ST) Advanced Practice Nursing /Staff stroke nurses. Respiratory Therapists. Educational/research programs. Clinical research. Community education/prevention. Professional education. Physicians. Vascular Neurology. Vascular Neurosurgery. Vascular Surgery. Diagnostic radiology and neuroradiology. Interventional/endovascular physicians. Critical care medicine. Physiatrists. Surgical and interventional therapies. CEA. Intracranial aneurysm clipping. Surgical removal or draining of blood from the brain. Placement of EVD and intracranial pressure monitors. Endovascular treatment of aneurysms and arteriovenous malformations. Intra-arterial reperfusion therapy. Endovascular treatment of vasospasm. PSCs certified within the past 2 years, 72.7% of eligible patients received tPA. The longer a PSC was in the certification program, the higher its tPA participation rate. Hospitals in their second certification cycle achieved a 78.6% IV tPA participation rate, and those certified for a third 2-year cycle achieved 94.4% participation. Among teaching hospitals in their first certification cycle, the rate of IV tPA use for eligible patients was 81% compared with 70% of nonteaching hospitals. Most studies have found Tx at PSC you’re more likely to have a better outcome and lower mortality.")
20
Mobile Stroke Unit Point-of-Care-based laboratory
compact CT scan results, reviewed remotely by hospital physicians results in early pre-hospital IV-thrombolysis and subsequent bridging therapy later with IA recanalization in the hospital A hospital system in Hamburg Germany developed a mobile stroke (treatment) ambulance to address the issue of suburban and rural stroke patient management and shorten time to treatment - bring the stroke care to the patient They have been able to dramatically reduce Call-to-Lab time, Call to CT time and, most importantly, Call-to-Therapy Decision-Advanced Treatment time, reduced from 120 minutes (two hours), to just minutes.
 ambulance to address the issue of suburban and rural stroke patient management and shorten time to treatment - bring the stroke care to the patient. They have been able to dramatically reduce Call-to-Lab time, Call to CT time and, most importantly, Call-to-Therapy Decision-Advanced Treatment time, reduced from 120 minutes (two hours), to just minutes.")
21
Options for Patients Experiencing an Ischemic Stroke
IV tPA Gold-standard in ischemic stroke care. Drug is designed to break apart the clot. Endovascular Clot Removal Mechanical disruption or removal of the clot using standard endovascular approaches Bridging Therapy Medical Management Monitor vitals and provide secondary stroke prevention. Patient is send to rehab or a nursing facility when stable.

22
Endovascular Therapy Anterior 12 hours Posterior <24h NIHSS >7
Evidence of Large vessel occlusion, hemodynamically unstable Large penumbra or clinical mismatch

23
25% vs 42.9%## MCA Occlusion Basilar Occlusion
Recanalization rate IV TPA: M1: 22%, M2:44%‡ Mortality: 25% vs 42.9%## Recanalization rate with IV TPA: <10% Mortality: 90% (persistent occlusion)** Internal Carotid Occlusion Recanalization rate with IV TPA: <10% Mortality: 73% (persistent occlusion)^^ ‡Alexandrov et al. Stroke ## Proact II: Jama 1999 **Meta analysis Furlan et al ^^ Flint et al. MERCI Registry Stroke 2008
** Internal Carotid Occlusion. Recanalization rate with IV TPA: <10% Mortality: 73% (persistent occlusion)^^ ‡Alexandrov et al. Stroke. ## Proact II: Jama **Meta analysis Furlan et al. ^^ Flint et al. MERCI Registry Stroke")
24
The Importance of Recanalization
Recanalization is strongly associated with improved function outcomes and reduced mortality.

25
Meta-analysis shows a strong correlation between opening the blood vessel and patient good outcomes
Rha JH, Saver JL. The impact of recanalization on ischemic stroke outcome: a meta-analysis. Stroke Mar;38(3):
:")
26
Clinical Trials Most recent published EVT (endovascular therapy) trial results Lessons learned Current trial design

27
New EVT Stroke Trials IMS III MR RESCUE SYNTHESIS - EXPANSION
NEJM February 7, 2013

28
IMS III

29
IMS III: Interventional Management of Stroke 3
Patients who had received intravenous rt-PA within 3 hours after symptom onset were randomized 2:1 to: IV tPA + IA therapy IV t-PA alone Primary outcome measure: 90-day mRS ≤ 2 Broderick JP. NEJM 2013;368:

30
Primary outcome: IMS III
mRS < 2 95% CI: -6.1% to +9.1% 40.8% with endovascular + IV rt-PA 38.7% with IV rt-PA alone Broderick JP. NEJM 368: , 2013

31
MR RESCUE

32
MR RESCUE: Methods ≤ 8 hours of onset Anterior circulation LVO
Randomized to either EVT or Medical Mgmt “penumbral” pattern by CT or MRI Penumbra : “Small core” (<90 cc), large penumbra Non-Penumbral: Large core and small/absent penumbra IV tPA treated patients without recan were eligible if MRA or CTA showed persistent occlusion Kidwell CS. NEJM 2013 Mar 7;368(10):914-23 32
, large penumbra. Non-Penumbral: Large core and small/absent penumbra. IV tPA treated patients without recan were eligible if MRA or CTA showed persistent occlusion. Kidwell CS. NEJM 2013 Mar 7;368(10):")
33
MR RESCUE: 90-day mRS NO DIFFERENCE IN OUTCOMES
Endovascular vs. medical therapy Penumbra vs. no penumbra p=0.23 p=0.32 Kidwell CS. NEJM 368: , 2013

34
Synthesis Expansion

35
Synthesis Expansion: Outcomes
Primary Outcome (mRS < 1) 30.4% EVT 34.8% IV tPA Death Rates EVT: 14 (8%) IV tPA: 11 (6%) Italian Medicines Agency (AIFA) “EVT is not superior to standard treatment with IV tPA” Ciccone A. NEJM 368: , 2013
 30.4% EVT. 34.8% IV tPA. Death Rates. EVT: 14 (8%) IV tPA: 11 (6%) Italian Medicines Agency (AIFA) EVT is not superior to standard treatment with IV tPA Ciccone A. NEJM 368: ,")
36
IMS III Protocol Versus Contemporary Practice
The majority of patients included in the study Were not imaged using modern approaches Were not triaged using modern approaches Were not treated using modern approaches

37
Imaging Assessment Basic Head CT only in most patients
More than 40% of IMS III patients had baseline CT with ASPECTS < 7

38
ASPECTS (Alberta Stroke Program Early CT Score)
")
39
ASPECTS Score - 4

40
Patient Selection Matters: Penumbra Pivotal Trial
Independent Blinded Retrospective Analysis Baseline NCCT Data Using ASPECTS mRS ≤ 2 Large Infarct 8/53 pts Small Infarct 15/30 pts Goyal M. Stroke 2010

41
IMS III - Imaging Assessment
Patients with “large clear regions of hypodensity” (darker than white matter and brighter than CSF) on CT, greater than 1/3rd of MCA territory were excluded Sulcal effacement and loss of grey-white matter differentiation were not contraindications Many patients would have likely been excluded with more conservative CT reading (ASPECTS), CTA-SI (source image) ASPECTS, MR Diffusion ASPECTS, CT Perfusion or MR Perfusion
 on CT, greater than 1/3rd of MCA territory were excluded. Sulcal effacement and loss of grey-white matter differentiation were not contraindications. Many patients would have likely been excluded with more conservative CT reading (ASPECTS), CTA-SI (source image) ASPECTS, MR Diffusion ASPECTS, CT Perfusion or MR Perfusion.")
42
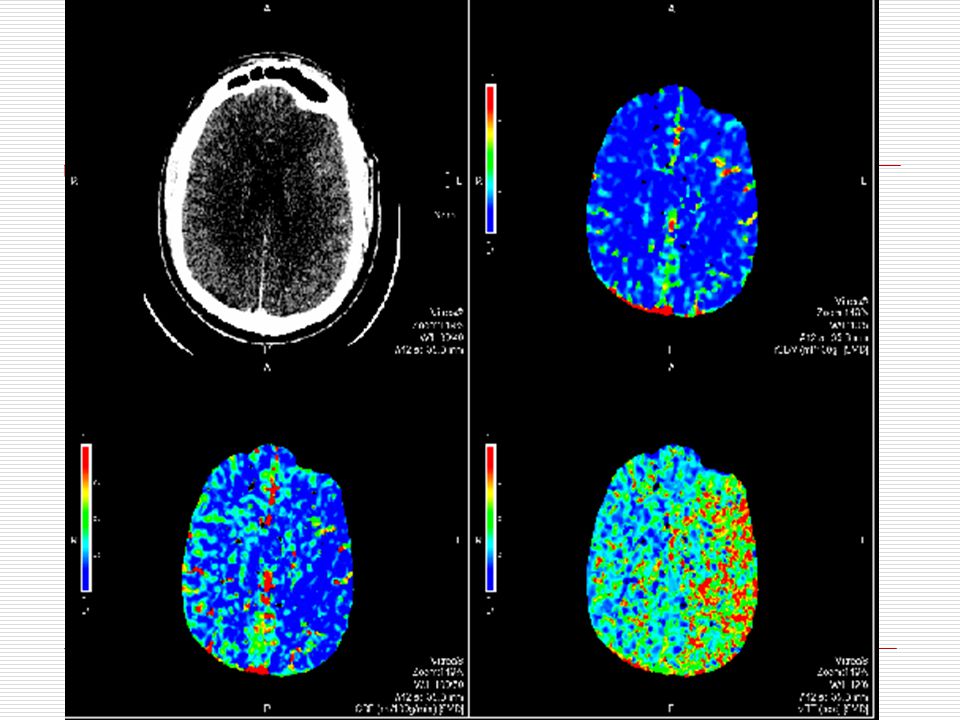
Imaging Based Selection: Perfusion Imaging

43
IMS III – EVT Arm Would ALL have been screened out with CTA
89 patients with ”no treatable or treated thrombus” 33 no thrombus seen 34 thrombus not treatable by EVT 12 with treatable thrombus but not treated No reason (1) Couldn’t safely cross occlusion (3) Recanalization during angio (2) Occlusion not responsible for clinical presentation (2) No reason (2) Would ALL have been screened out with CTA
 Couldn’t safely cross occlusion (3) Recanalization during angio (2) Occlusion not responsible for clinical presentation (2) No reason (2) Would ALL have been screened out with CTA.")
44
Clot characteristics (length)
No Clot > 8mm recanalized with IV tPA 43% of large vessel occlusions have greater than 8 mm clot lengths1 44

45
IMS III: Baseline CTA Occlusion Present – 90 day mRS
van Elteren test p-value

46
IMS III: Baseline CTA Occlusion Present - NIHSS > 20
van Elteren test p-value

47
TICI Score Grade 0 No perfusion
Grade 1 Perfusion past the initial obstruction, but limited distal branch filling with little or slow distal perfusion Grade 2a Perfusion of less than ½ of the vascular distribution of the occluded artery (e.g., filling and perfusion through 1 M2 division) Grade 2b Perfusion of ½ or greater of the vascular distribution of the occluded artery (e.g., filling and perfusion through 2 or more M2 divisions) Grade 3 Full perfusion with filling of all distal branches
 Grade 2b Perfusion of ½ or greater of the vascular distribution of the occluded artery (e.g., filling and perfusion through 2 or more M2 divisions) Grade 3 Full perfusion with filling of all distal branches.")
48
Percentage of Patients Who Achieved a Functional Outcome in IMS III Based on Reperfusion Result (p=0.001) In IMS III, independent functional outcome (mRS 0-2) was strongly associated with TICI 2b-3 revascularization.
 was strongly associated with TICI 2b-3 revascularization.")
49
IMS III ‘modern’ devices = 13% of endovascular cohort
Total endovascular treatments = 334/434 IA tPA EKOS + tPA 22 Merci 38 Merci + tPA 57 Penumbra 16 Penumbra + tPA 38 Solitaire 2 Solitaire + tPA 3 ‘modern’ devices = 13% of endovascular cohort

50
IMS III IMS-III endovascular reperfusion rates: ≥ TICI 2a ≥ TICI 2b
ICA % % M % % M % % Overall % % TREVO2* 92% 68% SWIFT* 94% 76% *Both are high quality independent core lab adjudicated, published in Lancet

51
Systems and Process Issues in the Era of Comprehensive Stroke Center Designation
Relative to IMS I and II, the IMS III trial suffered from a dramatic delay between the initiation of iv tPA and endovascular therapy At over two hours, this lag impedes the ability of reperfusion to realize clinical benefit.

52
IMS III patients further suffered a significant lag between groin access and initiation of IAT at the lesion Fourty-four minutes is far beyond reported standards with modern guide and distal access catheter technology

53
Time to Treatment IMS III Onset to arrival: 57 min
Arrival to IV tPA: 66 min IV to groin puncture: 86 mins Groin puncture to IA: 44 mins MR RESCUE Mean time from imaging to groin puncture: 2h 4 min SYNTHESIS Time from onset to start of treatment EVT hrs IV 2.75 hrs 130 mins between IV tPA and start of IA therapy By comparison STAR registry: Groin Puncture to guide cath placement: 12 mins Guide cath to TICI 2B/3 flow: 20 mins Critical as IA group did NOT receive IV tpa

54
Lessons Learned Endovascular Therapy is safe – as safe as IV rt-PA

55
Lessons Learned from Recent Ischemic Stroke Trials
It is not IV vs EVT IV tPA is proven Class 1 – it should not be denied from patients Future trials should compare best medical management versus best medical management + EVT Only enroll patients with LVO (large vessel occlusion) Excellent recanalization is needed TICI 2B or 3 Time is Brain Better determination of salvageable brain tissue ASPECTS CT Perfusion MRI Diffusion/Perfusion Set the stage for final portion of talk – can quickly review point 1 on this slide. We have already made the argument for point 2. Will then get into greater discussion of points 3-5 55
 Excellent recanalization is needed. TICI 2B or 3. Time is Brain. Better determination of salvageable brain tissue. ASPECTS. CT Perfusion. MRI Diffusion/Perfusion. Set the stage for final portion of talk – can quickly review point 1 on this slide. We have already made the argument for point 2. Will then get into greater discussion of points")
56
Merci Retriever “Cork Screw”

57
Newer Technologies = Better Recanalization
Solitaire FR Trevo Separator 3-D Penumbra Max System

60
Distal aspiration with retrievable stent assisted thrombectomy for the treatment of acute ischemic stroke William Humphries1, Daniel Hoit1, Vinodh T Doss1, Lucas Elijovich1, Adam S Arthur1 Abstract Objective Flexible large lumen aspiration catheters and stent retrievers have recently become available in the USA for the revascularization of large vessel occlusions presenting within the context of acute ischemic stroke (AIS). We describe a multicenter experience using a combined aspiration and stent retrieval technique for thrombectomy. Design A retrospective analysis to identify patients receiving combined manual aspiration and stent retrieval for treatment of AIS between August 2012 and April 2013 at six high volume stroke centers was conducted. Outcome variables, including recanalization rate, post-treatment National Institutes of Health Stroke Scale (NIHSS) score, symptomatic intracranial hemorrhage, discharge 90 day modified Rankin Scale (mRS) score, and mortality were evaluated. Results 105 patients were found that met the inclusion criteria for this retrospective study. Successful recanalization (Thrombolysis in Cerebral Infarction score 2B) was achieved in 92 (88%) of these patients. 44% of patients had favorable (mRS score 0–2) outcomes at 90 days. There were five (4.8%) symptomatic intracerebral hemorrhages and three procedure related deaths (2.9%). Conclusions Mechanical thrombectomy utilizing combined manual aspiration with a stent retriever is an effective and safe strategy for endovascular recanalization of large vessel occlusions presenting within the context of AIS. J NeuroIntervent Surg doi: /neurintsurg
. We describe a multicenter experience using a combined aspiration and stent retrieval technique for thrombectomy. Design A retrospective analysis to identify patients receiving combined manual aspiration and stent retrieval for treatment of AIS between August 2012 and April 2013 at six high volume stroke centers was conducted. Outcome variables, including recanalization rate, post-treatment National Institutes of Health Stroke Scale (NIHSS) score, symptomatic intracranial hemorrhage, discharge 90 day modified Rankin Scale (mRS) score, and mortality were evaluated. Results 105 patients were found that met the inclusion criteria for this retrospective study. Successful recanalization (Thrombolysis in Cerebral Infarction score 2B) was achieved in 92 (88%) of these patients. 44% of patients had favorable (mRS score 0–2) outcomes at 90 days. There were five (4.8%) symptomatic intracerebral hemorrhages and three procedure related deaths (2.9%). Conclusions Mechanical thrombectomy utilizing combined manual aspiration with a stent retriever is an effective and safe strategy for endovascular recanalization of large vessel occlusions presenting within the context of AIS. J NeuroIntervent Surg doi: /neurintsurg")
61
Case 1 53yo male presented with L MCA syndrome NIHSS 21 Onset 1 hour
Received iv-tpa within 60 min from door

62
Pre-treatment

64
Post-treatment

65
Case 1 Dysfluency and hemiparesis d/c to rehab with mRS of 2
1 mo f/u mRS of 1

66
Case 2 75yo male consulted for acute stroke Pseudobulbar palsy
Post. circulation strokes 3 months prior, d/c mRS 0, was on ASA/plavix

67
April 2013 30% stenosis 67

71
262 PRU

73
Case 3 35yo AA male presents with 2 hours of inability to produce speech and right sided weakness. PMH: bipolar d/o Exam: awake, not following commands, globally aphasic Right hemiplaegia NIHSS: 22

79
At Discharge: mRS- 0, NIHSS 1

80
Conclusions Stroke systems and patient selection critical to outcomes
EMS critical to triage, stabilizing and transporting to stroke center Imperative to recognize signs and symptoms of stroke especially large vessel occlusion IV-TPA standard of care Endovascular treatment can be performed quickly and safely Time is Brain!

81
Questions?

Similar presentations













 University of Helsinki Markku Kaste Department.>")












 Thrombolytic canalization of occluded arteries may reduce the degree.>")



