Download presentation
Presentation is loading. Please wait.

2
What is Patient- and Family-Centered Care?
Patient- and family-centered care is an approach to the planning, delivery and evaluation of health care that is grounded in mutually beneficial partnerships among patients, families, and health care practitioners. It is founded on the understanding that the family plays a vital role in ensuring the health and well being of patients of all ages. The ultimate goal of patient- and family-centered care is to create partnerships among health care practitioners, patients and families that will lead to the best outcomes and enhance the quality and safety of health care.

3
Four Core Concepts D I G N I T Y A N D R E S P E C T
Health care practitioners listen to and honor patient and family perspectives and choices. Patient and family knowledge, values, beliefs and cultural backgrounds are incorporated into the planning and delivery of care. I N F O R M AT I O N S H A R I N G Health care practitioners communicate and share complete and unbiased information with patients and families in ways that are affirming and useful. Patients and families receive timely, complete and accurate information in order to effectively participate in care and decision-making. PA R T I C I PAT I O N Patients and families are encouraged and supported in participating in care and decision-making at the level they choose. CO L L A B O R AT I O N Patients, families, health care practitioners, and hospital leaders collaborate in policy and program development, implementation and evaluation; in health care facility design; and in professional education, as well as in the delivery of care.

4
Patient- and Family-Centered Care: Why Is It Needed?
“ Care must be delivered by systems that are carefully and consciously designed to provide care that is safe, effective, patient-centered, timely, efficient, and equitable. Such systems must be designed to serve the needs of patients, and to ensure that they are fully informed, retain control and participate in care delivery whenever possible, and receive care that is respectful of their values and preferences. “ Institute of Medicine, Crossing the Quality Chasm (2001)
")
5
Crossing the Quality Chasm
1. Safe – avoiding injuries to patients from care that is intended to help them. 2. Effective – providing services based on scientific knowledge to all who could benefit and refraining from providing services to those not likely to benefit. 3. Patient-centered – providing care that is respectful of and responsive to individual patient preferences, needs and values, and ensuring that patient values guide all clinical decisions. 4. Timely – reducing waits and sometimes harmful delays for both those who receive and those who give care. 5. Efficient – avoiding waste, in particular waste of equipment, supplies, ideas, and energy. 6. Equitable – providing care that does not vary in quality because of personal characteristics such as gender, ethnicity, geographical location, and socioeconomic status.

6
Patient Centeredness The real business of health care is about preventing illness, healing those who are ill, meeting the needs of people who must live their lives with disabilities or chronic disease, and helping people in our communities achieve better health. Patient-centered care includes: respect for patients’ values, preferences, and expressed needs; coordination and integration of care; information, communication, and education; physical comfort; emotional support; and the involvement of family and friends.

7
R U L E S TO R E D E S I G N A N D I M P R O V E C A R E
1. Care based on continuous healing relationships. Patients should receive care whenever they need it and in many forms, not just face-to-face visits. 2. Customization based on patient needs and values. The system of care should be designed to meet the most common types of needs, but have the capability to respond to individual patient choices and preferences. 3. The patient should be the source of control. Patients should be given the necessary information and the opportunity to choice over their health care decisions.

8
4. Shared knowledge and the free flow of information
4. Shared knowledge and the free flow of information. Patients should have unfettered access to their own medical information and to clinical knowledge. Clinicians and patients should communicate effectively and share information. 5. Evidence-based decision making. Patients should receive care based on the best available scientific knowledge. 6. Safety as a system property Patients should be safe from injury caused by their care system.

9
7. The need for transparency
7.The need for transparency. The health care system should make information available to the pts and family that allows them to make informed decisions when selecting a health plan, hospital or clinical practice, or choosing among alternative treatments. 8. Anticipation of needs. The health system should anticipate patient needs, rather than simply reacting to events. 9. Continuous decrease in waste. The health system should not waste resources or patient time.

10
10. Cooperation among clinicians.
Clinicians and institutions should actively collaborate and communicate to ensure an appropriate exchange of information and coordination of care. Adapted from Crossing the Quality Chasm: A New Health Care System for the 21st Century, 2001.

12
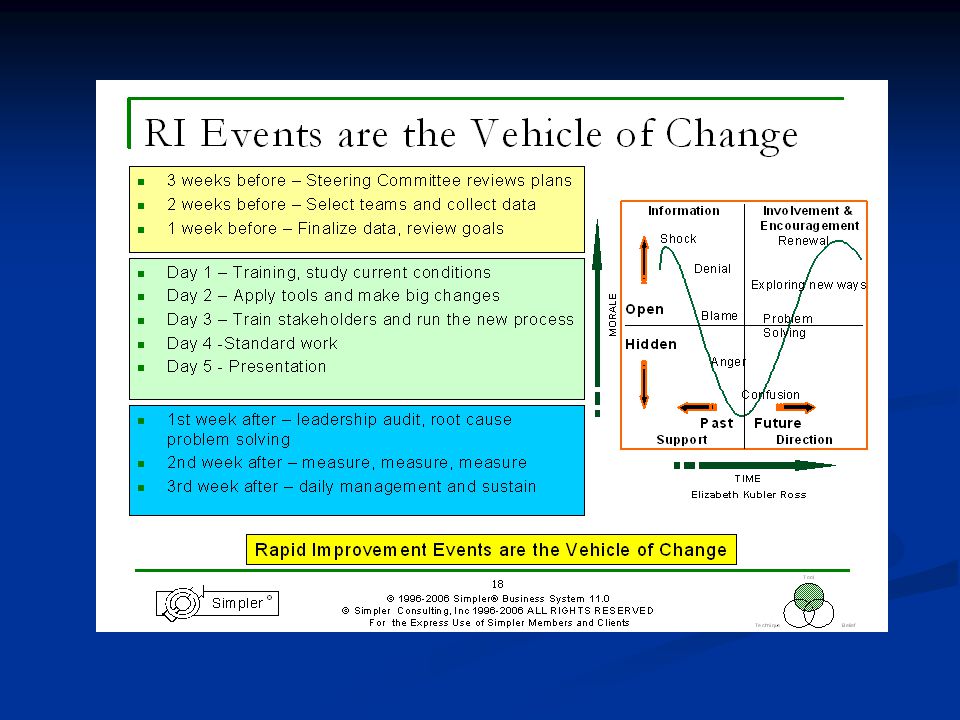
LEAN=Quality Improvement

19
PATIENT-FAMILY CENTERED CARE TEAM
Team Leader: June Sharkey Debbie Kaszycki Minnie Frazier Julie Siggelkow Judy Downey Kate Martin Krista Garner Ray Quintero

20
CHARTER SUMMARY Project Date: November 13-16, 06 Champion: Susan Grant
Opening 2D ICU-Patient Family Centered Care Project Date: November 13-16, 06 Champion: Susan Grant Objectives: To coordinate the flow for the family in 2D ICU Identify relationship between family, staff and physician (Rounding, Dr. 99 presence, MD discussion w/ families) Develop a plan for tools to facilitate communication for families including scripting and pt./family literature Develop standards of care utilizing best practices (EB) for patient family centered care(Pastoral care, social services, Public safety) Developing protocols for family room utilization (Facility management) Sponsor: Ray Quintero Sensei: Sonia Bergmann Team Leader: June Sharkey Team Members Debbie Kaszycki Minnie Frazier Julie Siggelkow Judy Downey Kate Martin Krista Garner Scope: 2D ICU-from initial contact with family and patient to D/C from ICU.
 Develop a plan for tools to facilitate communication for families including scripting and pt./family literature. Develop standards of care utilizing best practices (EB) for patient family centered care(Pastoral care, social services, Public safety) Developing protocols for family room utilization (Facility management) Sponsor: Ray Quintero. Sensei: Sonia Bergmann. Team Leader: June Sharkey. Team Members. Debbie Kaszycki. Minnie Frazier. Julie Siggelkow. Judy Downey. Kate Martin. Krista Garner. Scope: 2D ICU-from initial contact with family and patient to D/C from ICU.")
21
Current Family Waiting Area

22
Current Model vs. Family-Centered Approach
Historical models of patient care have been organized around the needs of healthcare professionals. Traditional methods of patient care delivery rarely involved family in medical management. A family-centered approach has been referenced to achieve high levels of quality care and increased patient satisfaction. Family-centered care encourages a collaborative team approach. Many aspects of patient and family centered care are cost-efficient and simply require a paradigm shift. Implementing a family centered approach to care is an ongoing commitment.

23
New Family Waiting Area

24
Accomplishments Lean exercises: Value streams, spaghetti charts, NVA / VA identification. Met with various individuals / ancillary staff: Pastoral services, Rollins DD, nutrition, day surgery advocate, ER patient administrative liason, patients’ family members. Family Process: Quick Sheet for admission and guidebook. Staff Education for new culture of family centered care.

25
Examples of Accomplishments
Rough drafts of admission quick sheet for individual family members as well as for laminated guidebooks to remain in family waiting areas. Generated ideas for the job description of the “family coordinator” Developed plan for staff education to promote a smooth transition into family-centered care. Listed ideas for “signage” throughout the “mothership/2DICU”

26
Team Responsibilities

27
Key Metrics for the Unit
Patient & Family Satisfaction ICU Survey Baseline 11/20 through December - Ray & Aaron Employee Satisfaction Gallup Poll Survey Baseline next week and then in Feb & Apr ’07 – Ray & Marilyn Stress Study Georgia Tech. TBD MD Satisfaction – ICU Admitting Surgeons & Neurologists Obtain a validated survey – Marilyn Family Member time spent with patient Family sign in/out Baseline units 2&3 11/20 thru Dec ‘07; Future collection Feb-Apr ‘07 Julie will create a form Lindsay

28
Lessons Learned Family-centered care relies upon COMMUNICATION amongst all members involved in the care of the patient. Family-centered care is a multidisciplinary group endeavor We can change the schematics of an ICU and upgrade with all the fancy stuff in the world but if we don’t upgrade the way we practice, change will never occur for the good of the patient. The LEAN project has encouraged us to network ideas with ancillary staff throughout EUH to successfully merge and create an innovative approach to patient care in the neuroscience ICUs. FONT STYLE AND SIZE Helvetica (Postscript)/Arial (Non-postscript) is the standard font for all slides. All headline and body text is recommended Bold. The headline text is set at black 30 point in UPPERCASE or UPPER lower case. Body copy is black UPPER lower case. The first and second level body copy text is 24 point. The third and fourth level is 20 point. Text should not drop below 18 point for readability. Create more than one slide if necessary to drop below 18 point. BULLETS The standard shape for first level bullets is a square from the Monotype Sorts drop down box under Format, Bullet. It is located in the third row, the sixth symbol from the right. It should be 60% of the size of the text. The second level bullet is a dash selected from the normal menu. It is located in the fifth row, eighth from the left. For second level text, this dash is used at 70% of the size of the text, all other levels are set at 60% of the size of the text. All are the same red as the title bar and ROCKWELL.
/Arial (Non-postscript) is the standard font for all slides. All headline and body text is recommended Bold. The headline text is set at black 30 point in UPPERCASE or UPPER lower case. Body copy is black UPPER lower case. The first and second level body copy text is 24 point. The third and fourth level is 20 point. Text should not drop below 18 point for readability. Create more than one slide if necessary to drop below 18 point. BULLETS. The standard shape for first level bullets is a square from the Monotype Sorts drop down box under Format, Bullet. It is located in the third row, the sixth symbol from the right. It should be 60% of the size of the text. The second level bullet is a dash selected from the normal menu. It is located in the fifth row, eighth from the left. For second level text, this dash is used at 70% of the size of the text, all other levels are set at 60% of the size of the text. All are the same red as the title bar and ROCKWELL.")
29
Expectations The current model of patient care will be transitioned to a family-incorporated approach. May be difficult at first In-services and continued staff education should assist with integration of family-centered values into the unit’s standards and policies Family-Centered care is an ongoing journey. FONT STYLE AND SIZE Helvetica (Postscript)/Arial (Non-postscript) is the standard font for all slides. All headline and body text is recommended Bold. The headline text is set at black 30 point in UPPERCASE or UPPER lower case. Body copy is black UPPER lower case. The first and second level body copy text is 24 point. The third and fourth level is 20 point. Text should not drop below 18 point for readability. Create more than one slide if necessary to drop below 18 point. BULLETS The standard shape for first level bullets is a square from the Monotype Sorts drop down box under Format, Bullet. It is located in the third row, the sixth symbol from the right. It should be 60% of the size of the text. The second level bullet is a dash selected from the normal menu. It is located in the fifth row, eighth from the left. For second level text, this dash is used at 70% of the size of the text, all other levels are set at 60% of the size of the text. All are the same red as the title bar and ROCKWELL.
/Arial (Non-postscript) is the standard font for all slides. All headline and body text is recommended Bold. The headline text is set at black 30 point in UPPERCASE or UPPER lower case. Body copy is black UPPER lower case. The first and second level body copy text is 24 point. The third and fourth level is 20 point. Text should not drop below 18 point for readability. Create more than one slide if necessary to drop below 18 point. BULLETS. The standard shape for first level bullets is a square from the Monotype Sorts drop down box under Format, Bullet. It is located in the third row, the sixth symbol from the right. It should be 60% of the size of the text. The second level bullet is a dash selected from the normal menu. It is located in the fifth row, eighth from the left. For second level text, this dash is used at 70% of the size of the text, all other levels are set at 60% of the size of the text. All are the same red as the title bar and ROCKWELL.")
Similar presentations