Download presentation
Presentation is loading. Please wait.

1
Documentation Issues with Electronic Medical Records
Suzanne McMurtry Baird, DNP, RN Clinical Nurse Specialist The Woodlands, Texas

3
Objectives Discuss current issues with electronic health record documentation Discuss documentation strategies to best utilize electronic technology Illustrate documentation concepts in case studies

4
Documentation No documentation Poor documentation
Confusing documentation Conflicting documentation Missing documentation

5
Documentation LEGAL ISSUE
Inadequately documented medical record can be your worst liability! A well-documented medical record can be your greatest legal asset! LEGAL ISSUE

6
Documentation Essentials
Assessment – What did you see or not see? Frequency Interventions – What did you do? Who did you tell? Response to interventions Plan of care

7
Documentation Data from external sources flow into EMR
EFM Vital signs Hemodynamics Validation of data Is the information accurate?

8
Documentation Myth “If it wasn’t documented…… it wasn’t done”

9
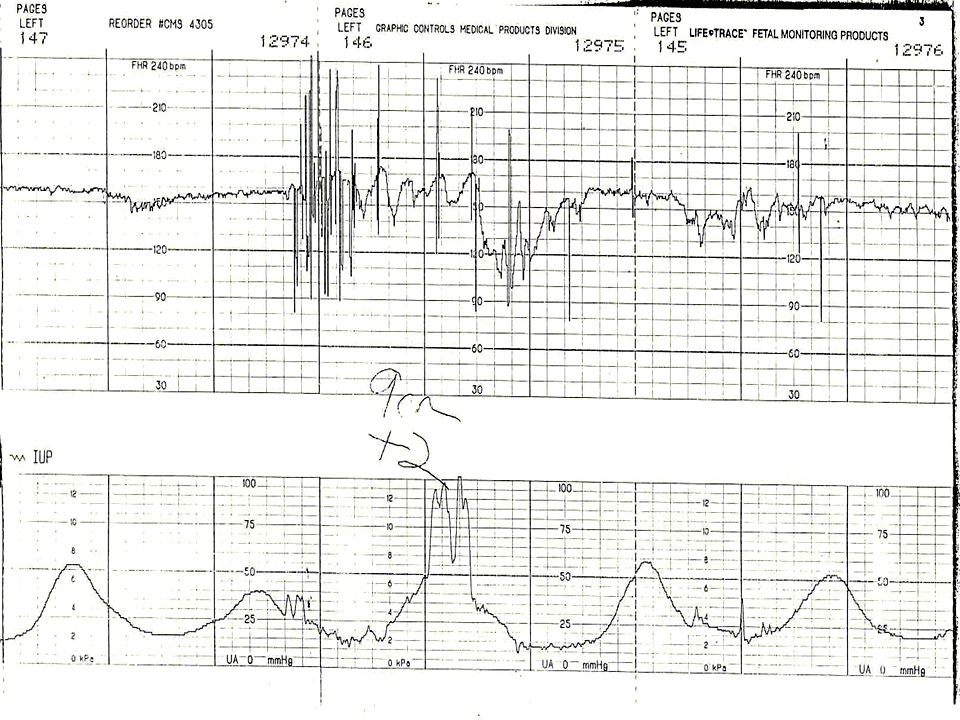
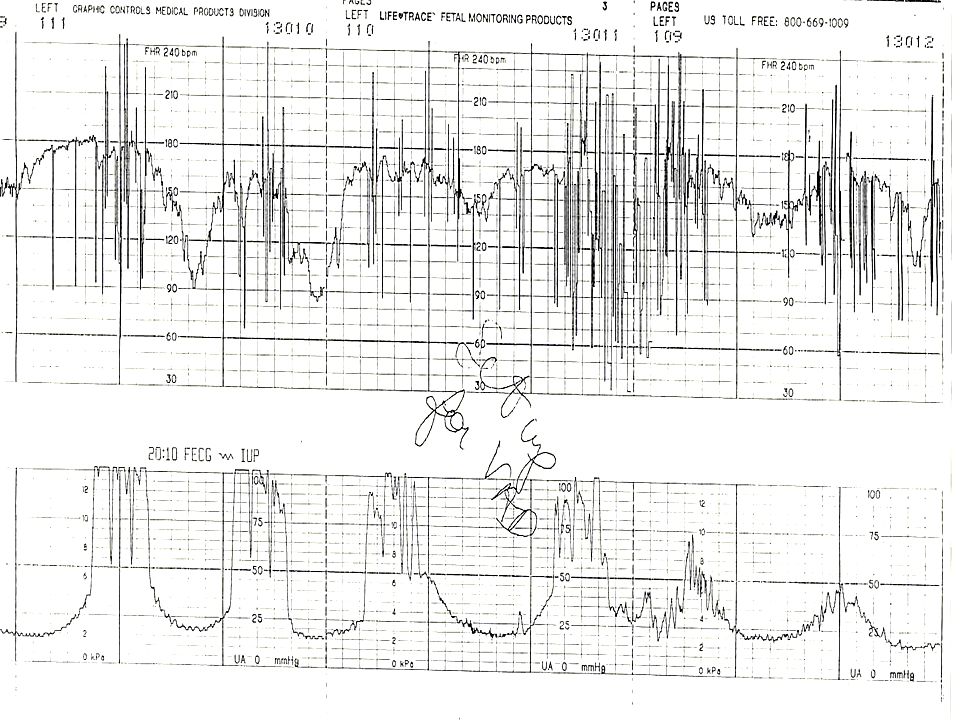
Documentation – Example
What are the components of documentation that need to be included in regards to the EFM strip?

10
Documentation Example
“Doctor aware. No orders received”

11
Documentation - Example
Prolonged deceleration noted at 2217, lasting x 5 minutes. BP 122/74, Uterine activity WNL, Maternal position change left side, right side, knee chest, O2 started at 10L fm, 500 mL IVF bolus, Cervical exam = C, + 3 station (rapid change), No cord felt, physician notified at 2219 – coming to room, Charge RN notified and requested additional assistance. Preparing patient for vacuum assisted delivery. NICU notified for presence at birth. Plan to assess FHR q 5 minutes. OR team and anesthesia notified – on standby.
, No cord felt, physician notified at 2219 – coming to room, Charge RN notified and requested additional assistance. Preparing patient for vacuum assisted delivery. NICU notified for presence at birth. Plan to assess FHR q 5 minutes. OR team and anesthesia notified – on standby.")
12
Case Study – Communication & Documentation
RN assigned to patient from 7am until time of birth at 12:58pm Physician examines patient at 8:35 am, leaves hospital for office Patient begins to show slow or no progress; oxytocin increased with resulting tachysystole and prolonged deceleration; fetal tachycardia and minimal-absent variability followed the deceleration At 10:25 am RN reports to physician that the patient is complete, pushing effectively with no mention of oxytocin dose, abnormal FHR parameters. Neither RN or physician remembers who initiated phone call.

13
Case Study At some point, the Charge RN becomes involved in patient care, but no documentation is made as to whom, if anybody, contacted her or if she just happened to be there. Patient allowed to “labor down” and oxytocin is stopped around 11:00 am with the RN contacting the physician. Charge RN did not contact physician Physician arrives at 12:30 pm expecting to see normal EFM strip

14
Case Study – Physician Deposition
Q: And it’s the nurse’s job to tell you when you should come to the bedside? A: It’s the nurse’s job to inform you of what the status of the patient is, the fetus and the mother, in which you decide if you want to come to the bedside. Q: Did you rely on Nurse ______ to perform that function? A: Yes

15
Case Study RN documentation did not reflect correct EFM assessment
In the 8 hours that the patient was in labor, the physician only checked on the patient 2 times The child has cerebral palsy. Plaintiffs were able to use the poor communication and miscommunication regarding the strip to force a substantial settlement. This case was made on the finger pointing by one physician. Had the RNs and physician documented their actions and their plan of care, the damages may have been substantially mitigated.

16
EMR Wish List

17
Improving the Health Care System
Six Aims Safe Effective Patient-centered Timely Efficient Equitable Crossing the Quality Chasm (2001) Institute of Medicine
 Institute of Medicine.")
18
Documentation - Safe Checklists Time out Quality and safety data

20
Documentation - Safe Quality Measures
“We measure what we value and we improve what we measure” AWHONN

21
AWHONN Measure 02: Second Stage of Labor Mother-Initiated, Spontaneous Pushing
Mother-initiated, spontaneous pushing in the 2nd stage of labor begins at the time the patient feels the urge to push. Spontaneous pushing is defined as a mother’s response to a natural urge to push or bearing down effort that comes and goes several times during each contraction. It does not involve timed breath holding or counting to 10. Documentation in the medical record will reflect nursing education to the patient regarding the 2nd stage of labor; patient’s report of feeling pressure or the urge to push prior to initiation of active pushing and evidence of nursing support during the 2nd stage of labor. Mother-initiated pushing Assisting the patient into upright, gravity-neutral positions Encouraging grunting or vocalization during the push in response to contractions.

22
Documentation - Safe Order Entry Clear Concise
Match policy/care guidelines

23
Documentation - Effective
Trending of Data Vital Signs Labs Intake and Output

24
Documentation - Effective
Ability to recreate clinical picture Fragmented documentation If you were unaware of previous patient care data, would you be able to look at medical record and determine care needs?

25
Documentation - Effective
Essential categories of assessment Legal Issue: Assessment parameters are incomplete or not available for documentation

26
Documentation - Effective
Will you remember the specifics about your care several years later? Interventions Sequence of events and interventions Communication Timing

27
Assessment parameters
Uterine contractions Fetal status Frequency Intensity Duration Resting tone Baseline rate Baseline variability Periodic patterns Accelerations Decelerations

28
Assessment parameters
Non-invasive assessment of hemodynamics and tissue perfusion Pulses Quality of pulses Skin color Skin temperature Capillary refill Mucous membranes Heart sounds Breath sounds Urine – amount and color

29
Abnormal Assessment Parameters
Are normal parameters defined? What should the RN do when assessment parameters fall outside of normal values? How are abnormal parameters documented? Example: Maternal HR 122, documentation WNL

30
Documentation – Patient Centered

31
Documentation - Timely
Late notes Time of late entry in comparison to patient care

32
Documentation - Efficient

33
“Department of Redundancy Department”
Staffing Guidelines Frequency of documentation requirements Physician/RN/Anesthesia _____________________________________________ Bottom Line We don’t have time for this!

34
Plan of Care documentation
What was the Physician/CNM/RN thinking? Weakness in most systems Liability Example: Fetal heart rate with abnormal assessment parameters, but remains in Category II with some reassuring findings Why did you continue to watch abnormal parameters? Plan of Care is not a form!

35
Narrative Discreet data
Are there limitations to the amount of narrative documentation? Ability to expand clinical assessment Abnormal assessment parameters plan of care Communication with other healthcare providers What was the specific communication? Is there ability to document communication?

36
Documentation - Equitable
Prenatal Records Ability for off service Physicians/RNs to document consultation in EMR Operative suites Antepartum Outpatient OB Clinic Intensive Care Emergency Department Medical – Surgical Unit Main OR

37
Medication Reconciliation
Outpatient Inpatient Triage Admission Change in service/unit Discharge

38
Ability To Document Emergency Situations
RRT Code Blue Operative vaginal birth Shoulder dystocia RN maneuvers Provider maneuvers Hemorrhage/MTP

39
Case Studies

40
Case Study – Patient History
G 1 EGA = 39 2/7 weeks Elective induction – severe maternal discomfort Cervix = 2 cm / 80% 0 station Plan – oxytocin; epidural for pain management

41
Note: 39 week Hard Stop

42
Checklist

43
Bishop’s Score Closed 0 – 30 -3 Firm Posterior 1 1 – 2 40 – 50 -2
Dilation Effacement Station Consistency Position of cervix Closed 0 – 30 -3 Firm Posterior 1 1 – 2 40 – 50 -2 Medium Mid-position 2 3 – 4 60 – 70 -1,0 Soft Anterior 3 > 5 > 80 +1, +2

45
Case Study RN Documentation: “Pt. pushing. Friends holding and supporting legs. Comfortable with epidural” Physician Documentation: “Pt. did not have particularly good pushing effort, nor particularly good control, and was fairly emotional and uncooperative”

46
Oxytocin In-Use Checklist

47
Case Study - 2010 Cervix – complete Vertex LOA @ -1 to -2
Maternal temp 100.1 Fetal tachycardia Plan – Vacuum extraction

56
Case Study – Second Stage Summary
Vacuum extraction Fundal pressure Nucal cord – tight – reduced McRoberts maneuver performed Suprapubic pressure Could not reach posterior arm 4th degree episiotomy Delivered posterior arm

57
Case Study – Delivery @ 2121 Pediatrics in attendance
Apgars 1 (1) and 2 (5) Physician Note: “a segment of cord was obtained for a gas, but somehow the nursing staff did not draw the gas and it clotted” EBL = 1200 cc
 and 2 (5) Physician Note: a segment of cord was obtained for a gas, but somehow the nursing staff did not draw the gas and it clotted EBL = 1200 cc.")
58
Case Study – RN Documentation
“Pt. tired, pushes well at times. Baby coming down with vacuum” No documentation Fetal station # vacuum attempts How long vacuum applied Patient cooperation Fundal pressure Shoulder dystocia Maneuvers to correct

59
Case Study – RN No interventions Anticipation Oxygen not started
Pitocin remained at 22 mu

60
Case Study – Physician Documentation
“Vacuum applied and vertex pulling to crowning position over 5-6 UCs over about a 30 minute time period. At that time, pt. became very combative and uncooperative. The pt as I said was very uncooperative and did not push with any effort. With fundal pressure and continued pushing, male infant delivered”

61
Case Study – Newborn Outcome
Birth asphyxia diagnosed Developmental delay

62
Case Study – Legal Outcome
Depositions: “During vacuum, physician placed leg on the foot of the bed and pulled until red in the face and shaking; leaned back on stool; feel off stool; delivery table fell over” RN experts x 2 – unable to defend Legal case settled

Similar presentations

















 on a pregnancy. Discuss assessments for a patient with.>")










