Download presentation
Presentation is loading. Please wait.

1
Falls – an over view for GPs
Julie Brache Consultant Geriatrician and Falls Lead October, 2014

2
Overview Why older people fall Multifactorial risk assessment
Normal changes with ageing Dizziness and syncope Medication review Multifactorial interventions Where to get advice

3
Definition when an individual comes to rest unintentionally on the ground or another lower level, with or without loss of consciousness

4
Background 35% >65 living at home fall each year
£2.3 billion per year 10% injury After a fall 50% have reduced mobility Leading cause of injury related death in older adults

5
Preventable Evidence based national and international guidelines N

6
Fall is a symptom, not a diagnosis

7
‘Old age starts with the first fall and death comes with the second’
Gabriel Garcia Marquez “Love in the time of cholera”

8
Frailty Reduced ability to withstand illness without loss of function
Muscle weakness, reduced walking speed, reduced physical activity, weight loss, self reported exhaustion Would you be surprised if this person died in the next year?

9
Falls are multifactorial

10
Why do older people fall?
Muscle weakness Poor balance Gait deficit Polypharmacy Sensory loss – vision, hearing, peripheral Medical illness Nutrition Dizziness Osteoarthritis Frailty Environment Depression Cognitive impairment Incontinence Alcohol Previous falls CV problems Neurological

12
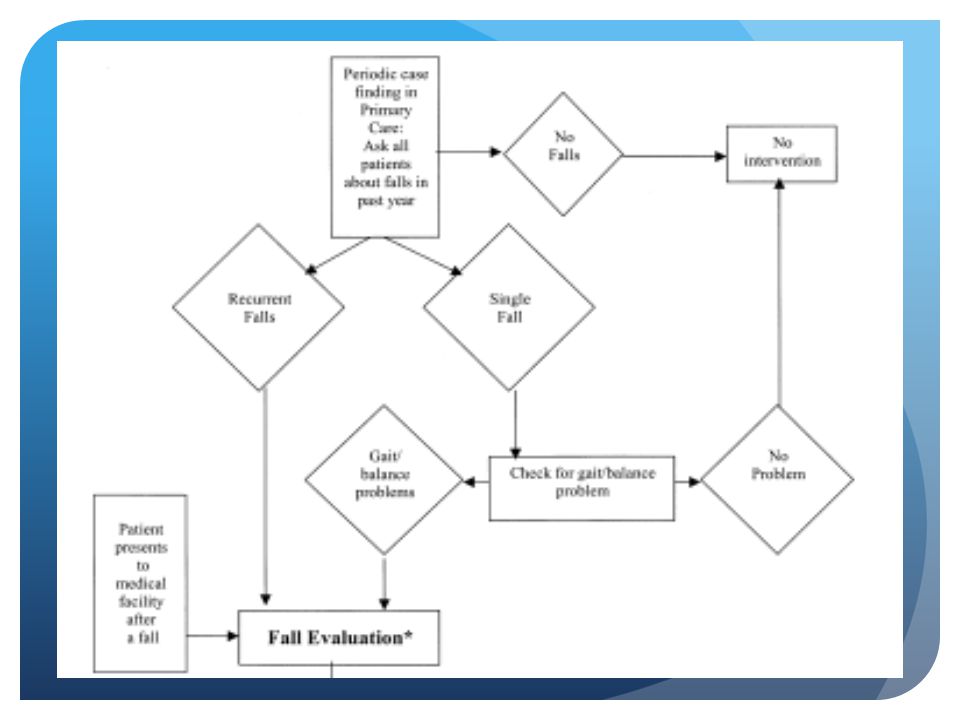
History Circumstances of falls How many falls in the last year?
Activity at the time Where and when Lightheaded, dizzy, LoC, chest pain, palpitations, visual disturbance? Seizure markers? How many falls in the last year?

13
Taking the history –some pointers
Allow them to describe everything first, then get the history you need Describe a single fall in detail Take them through it in fine detail Then ask about associated symptoms Witness account is vital

14
History - pitfalls “It was nothing” “I haven’t fallen”
“I tripped over the cat” “I must have…….” “They had a fit, doctor”

15
Assess Continence Cognition Frailty Alcohol intake
Psychological consequences of falling Fear, anxiety, depression

16
Examination Cardiovascular Pulse – rate and rhythm Heart sounds
3 min lying and standing BP Drop 20 systolic or 10 diastolic or to <90 significant Only 23% will describe dizziness ECG

18
Examination Focused neurological examination
Lower limb strength – hip and ankle flexors Peripheral sensation Evidence of stroke, Parkinson’s cerebellar signs? Gait and balance Vision

19
Ageing and gait Slower Increased sway
Slowed postural support responses Shorter stride length Increased time in double support Loss of rhythm Loss muscle bulk, reduced postural reflexes, JPS

20
Gait disorders in the elderly
Parkinsonism Cerebrovascular disease Cervical spondolytic myelopathy Sensory neuropathy Foot drop Don’t forget Normal Pressure Hydrocephalus

21
Gait and balance assessment
Not all for the Physio! Gait: Get Up and Go Balance: Proprioception – vision- vestibular function -> Romberg's -> Head Thrust

22
Ageing and vision ↓Acuity ↓Depth perception
Lens density changes- glare Decreased rod density - ↓Light adaptation - ↓ contrast sensitivity ↓ Visual processing speed

23
Vision Test acuity and fields
ARMD, glaucoma, stroke, diabetes, cataract Bifocal / varifocal glasses, change in prescription

24
SPECTACLE USE 5.7 Optometrists and dispensing opticians should consider supplying an additional pair of single vision spectacles (to wear in outdoor and unfamiliar settings) for older people who take part in regular outdoor activities
 for older people who take part in regular outdoor activities.")
25
Examination Other Cognition Foot wear and feet

26
Take the shoes off!

27
Dizziness Vertigo Pre-syncope Dysequilibrium

28
Vertigo Illusion of rotation “The room was spinning”
Nystagmus during episode Labyrinth or vestibular problem Occasionally cerebellar or CP angle Treat acute attacks with anti-histamines

29
Benign Paroxysmal Positional Vertigo
Vertigo on change in position Self limiting Disabling Hallpike- Dix test Epley manoeuvre Vestibular rehab Cawthorne- Cooksey exercises Brandt - Daroff

30
Pre-syncope Sense of feeling faint or light-headed “Legs went weak”
“Vision blurred ” Pallor, weak/slow pulse Same causes as syncope Often a sign of postural BP drop Cardiovascular assessment Treat underlying cause

31
Dysequilibrium Balance dysfunction A sense of unsteadiness
“Thought I was going to fall” Often multi-factorial Sensory impairments and/or CNS disease Multidisciplinary management

32
Syncope 23% >65s over 10 years High recurrence rate
Spontaneous LOC with complete recovery Diagnosis difficult and often wrong

33
Syncope in the Elderly Cerebral autoregulation impaired
Baroreflex sensitivity blunted Volume regulation impaired Comorbid illness and medications

34
Syncope diagnosis All in the history DETAIL Posture Prodrome
Eye movements Tongue biting/incontinence Injury Duration Confusion Hemi weakness

35
Red flags Abnormal ECG (NICE) Heart failure Syncope during exertion
FHx sudden death <40 New/unexplained SOB Murmur (NICE)
")
36
Assessment Vasovagal – 3Ps Cardiovascular – if in doubt Neurological
ECG, 24 hour tape, event recorder, implantable device, tilt table test + carotid sinus massage, cardio ref Neurological CT head, EEG (?value in elderly), neuro ref
, neuro ref.")
37
Tilt Tests Unexplained, recurrent syncope
Single syncope in high risk settings Unexplained recurrent falls

38
Falls and acute illness
Fall often the presentation of an acute illness Think of falls risk when unwell diuretics, antihypertensive, steroids, anticholinergics, sedatives urinary urgency/frequency Delirium

39
Medication review

40
Drugs in the elderly UK elderly 18% pop – 45% all prescriptions
In NH in 1 year 97% will receive a prescribed drug – 71% in community Polypharmacy - >4 drugs = risk falls

41
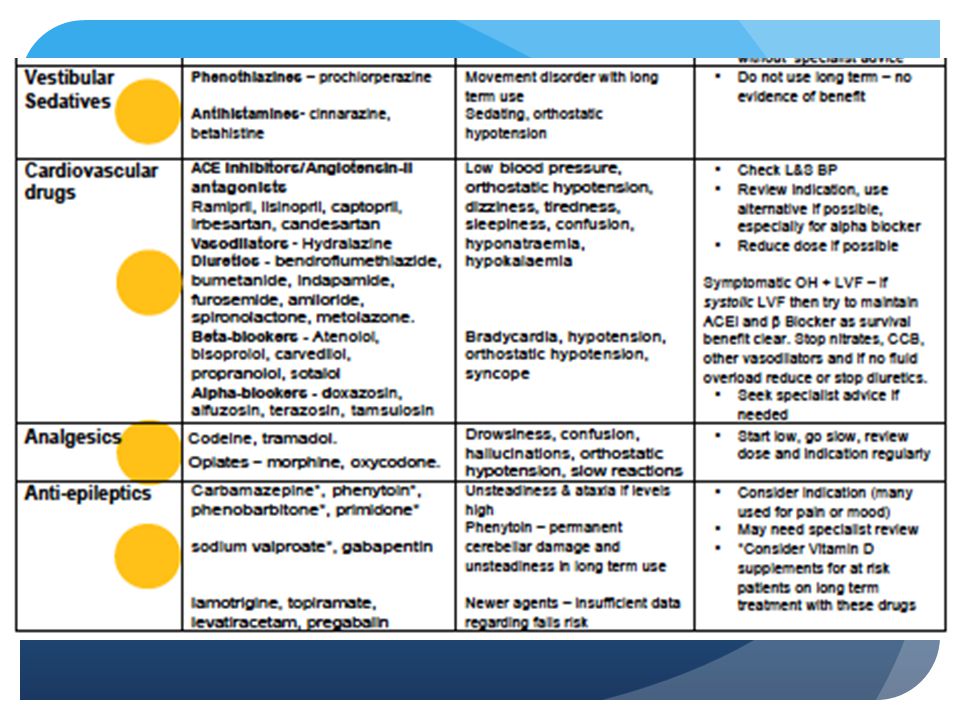
Principles of Medication review
Review indication – is there evidence? Review dose Reduce the number of medicines Avoid complex regimes Review benzodiazepines and other psychotropic drugs Check L&S BP – if drop review culprit drugs

42
Medication and Falls Risk
“Therapeutic effect” Interactions Side effects 2/52 after change in meds – high risk time Stopping – can be difficult

43
“Therapeutic effect” Meta-analysis – sedatives and hypnotics
Improve sleep duration and reduce night time wakening NNT sleep 13 NNT any adverse event 6 BMJ 2005;331:1169

44
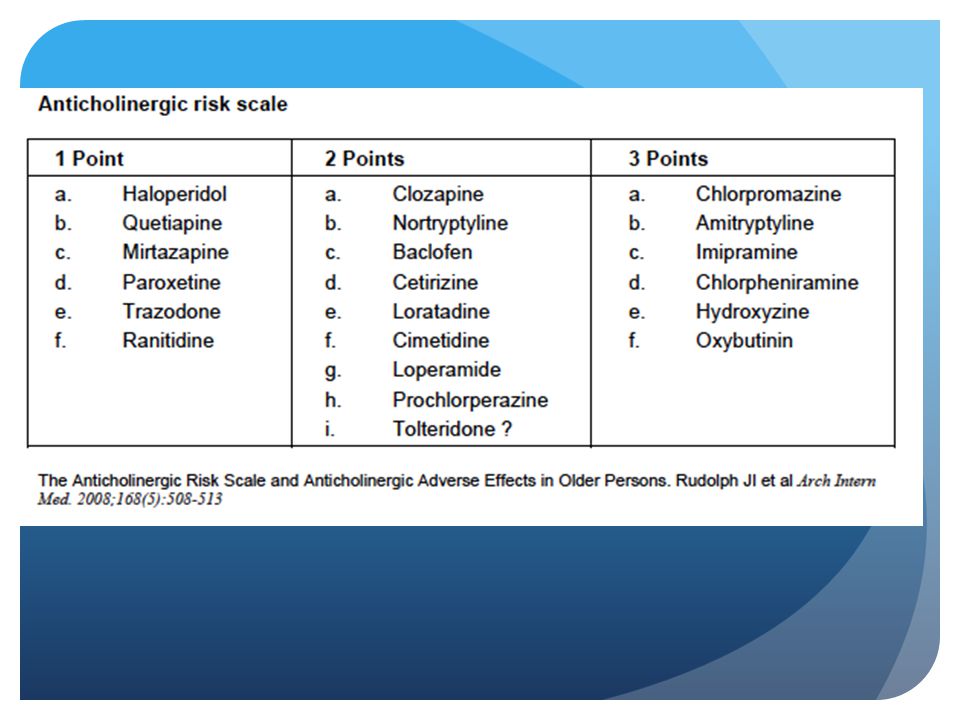
Side effects – anticholinergic activity
Antiarrhythmics - disopyramide, procainamide Antidepressants – tricyclics Antipsychotics – chlorpromazine, prochlorperazine Antiemetics – cyclizine, prochlorperazine Antiparkinson – amantadine, benzhexol Antispasmodics – oxybutynin Bronchodilators - ipatropium

46
Time to reconsider warfarin?
50% elderly in AF not on warfarin Falls is the main reason >300 falls per year for bleeding risk to outweigh stroke risk

47
Ageing and Pharmacokinetics / Pharmacodynamics
Distribution ↑blood (& tissue) conc water sol drugs ↑ vol distribution lipophilic drugs Hepatic metabolism Metabolism by C P-450 reduced Reduced 1st pass metabolism – some drugs Renal elimination Reduced GFR with age Changes in drug-receptor interactions
 conc water sol drugs. ↑ vol distribution lipophilic drugs. Hepatic metabolism. Metabolism by C P-450 reduced. Reduced 1st pass metabolism – some drugs. Renal elimination. Reduced GFR with age. Changes in drug-receptor interactions.")
48
April 2014

51
Osteoporosis assessment
FRAX – but beware over 80s Calcium and vitamin D Reduce falls All housebound fallers, and RH/NH residents 800iu daily vit D Long term anticonvulsants – check vit D level

53
Hip protectors Controversial area! At home – ineffective Institutions?
Current advice: May be useful in confused elderly in institutional care

54
Multifactorial interventions
Treat any problems found Evidence based recommendations: Strength and balance training Home hazards assessment & intervention Vision assessment and referral Medication review and modification/withdrawal of psychotropics Education

55
How to get advice

56
Geriatric Advice Line

57
Clinics Geriatric clinic Falls clinic Doctor, 45 min appointment
Nurse, therapist and doctor, 2 hour appointment, on-going therapy via referral to community teams Geriatric clinic Doctor, 45 min appointment If you just want therapy – refer to community teams If already seeing community team – refer to geriatric clinic PLEASE send as much information as possible

58
Take home messages Some falls are preventable
Requires time consuming multifactorial assessment, identification and intervention Can’t do it alone Always review medication Don’t forget bones A friendly geriatrician is always on the end of the phone

59
Questions?

Similar presentations










>")











