Download presentation
Presentation is loading. Please wait.

1
Enterobacteriaceae and 3 rd generation cephalosporin breakpoints - European and US (CLSI) current and pending breakpoints Gunnar Kahlmeter EUCAST
 current and pending breakpoints Gunnar Kahlmeter EUCAST")
2
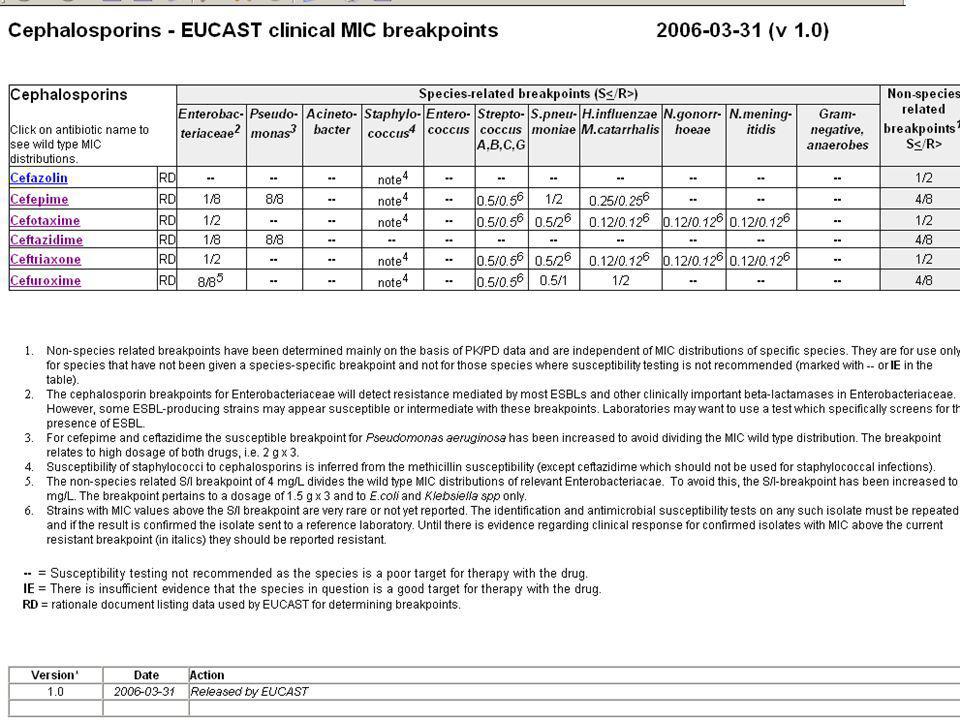
This presentation will deal with Cefuroxime Cefotaxime Ceftriaxone Ceftazidime Cefepime European and US (CLSI) breakpoints for: …it will not deal with ESBL detection or characterisation.
 breakpoints for: …it will not deal with ESBL detection or characterisation.")
3
Breakpoint committees CommitteeCountryAST system BSACUnited KingdomYes CA-SFMFranceYes CLSIUSAYes CRGThe NetherlandsNo DINGermanyNo NWGANorwayNo SRGASwedenYes

4
S/I-breakpoints I/R-breakpoints ESBL

5
S/I-breakpoints I/R-breakpoints ESBL

6
To determine breakpoints has always been part science and part art! ….the science is growing stronger…. …but so far we have had difficulties agreeing:

7
Cefotaxime CommitteeS BSAC1 / 1 CA-SFM4 / 32 CLSI8 / 32 CRG4 / 16 DIN2 / 8 NWGA1 / 4 SRGA0.5 / 1

8
Breakpoint committees must have procedures for re-evaluating and revising breakpoints of existing drugs. Initial breakpoints often overly optimistic, - with few exceptions, revised breakpoints have been lowered New resistance mechanisms need to be assessed, Doses and indications may change, New drugs within the class provoke a need for re- evaluation of breakpoints of existing drugs, The tools available for determining breakpoints have improved and the older breakpoints need to be ”overhauled” with new tools!

9
EUCAST and CLSI EUCAST - in concert with EMEA and the pharmaceutical companies, EUCAST has devised procedures for setting breakpoints for new drugs. - has devised procedures for re-evaluating breakpoints for existing drugs (can be initiated by the company, EMEA or EUCAST). CLSI - and FDA currently do not agree on the mandate of CLSI to determine breakpoints for new drugs or to revise breakpoints for existing drugs.
. CLSI - and FDA currently do not agree on the mandate of CLSI to determine breakpoints for new drugs or to revise breakpoints for existing drugs..")
10
Why revise Enterobacteriaceae 3rd generation cephalosporine breakpoints? And why now?

11
1.The multiflora of cephalosporine breakpoints in itself calls for revision and hopefully harmonisation. 2.Many of our current cephalosporine breakpoints are - too high – do not in themselves correlate well with clinical outcome - do not detect those enzymes that need to be identified for successful therapy - are out of sync with modern pK/pD-concepts 3.There is evidence that the clinical correlate is to the MIC rather than to the presence of the enzyme. 4.New techniques in breakpoint setting can improve on the breakpoints determined 25 years ago. Why?

12
5.It is becoming increasingly important to assure that the breakpoints themselves correlate to clinical outcome - - the rapidly increasing multiflora of resistance mechanisms and species with ESBLs makes screening more complicated and increasingly unreliable, - the screening for and identification of ESBLs often delay the report (of an R) to the clinician, - many laboratories do not employ adequate ESBL screening across the board - they may screen isolates from septicemia cases but not from UTI.
 to the clinician, - many laboratories do not employ adequate ESBL screening across the board - they may screen isolates from septicemia cases but not from UTI.")
13
Both EUCAST and CLSI emphasise that the new breakpoints are clinical breakpoints - not breakpoints designed to detect every ESBL. However, the clinical breakpoints will detect the absolute majority of ESBLs ……and for anyone who wants to catch every ESBL, irrespective of clinical significance, the current detection methods (see next slide) have not changed or EUCAST has made available species specific epidemiological cut-off values (see the slide after next and www.eucast.org).
 have not changed or EUCAST has made available species specific epidemiological cut-off values (see the slide after next and")
14
ESBL detection tests Cefpodoxime + single substance which will detect all (?) ESBLs. + high sensitivity - low specificity - will screen for ESBL but when negative there is ”nothing to report” - and, because of the low specificity, when positive you need to put in more work (confirm and characterize) before you report to the clinician Cefotaxime AND ceftazidime - both needed to find all (?) ESBLs (many microbiologists hesitate to ”waste” space on two 3rd generation cephs) + high sensitivity + high specificity + will screen for ESBLs and give a plausible profile + cefotaxime and ceftazidime susceptibility to include in report - these cephalosporines are not relevant for less serious infections
 before you report to the clinician Cefotaxime AND ceftazidime - both needed to find all ( ) ESBLs (many microbiologists hesitate to waste space on two 3rd generation cephs) + high sensitivity + high specificity + will screen for ESBLs and give a plausible profile + cefotaxime and ceftazidime susceptibility to include in report - these cephalosporines are not relevant for less serious infections.")
15
Comparison of EUCAST clinical breakpoints and epidemiological cut-off values EUCASTEpidemiological cut-off values S≤S≤R>E.coliK.pneK.oxyP.mir Cefuroxime8 Adj 88884 Cefotaxime120.250.12 0.06 Ceftriaxone180.250.12 0.06 Ceftazidime180.5 0.12 Cefepime180.12 Adj Adjusted from 4 to 8 to avoid dividing wild type Enterobacteriaceae

16
Should ESBL-detection and characterization be abandoned? Yes – the new breakpoints shall predict clinical outcome. No – ESBLs have implications for infection control and the epidemiology of antimicrobial resistance in hospitals.

17
For laboratories with other main interests than ”antimicrobial resistance”, the use of an appropriate breakpoint will simplify everyday life. A breakpoint which will guide therapy and where the SIR- categorisation is not delayed by the detection and categorisation of every ESBL, will be beneficial to patient care. The clinical rationale for the new breakpoints are: - When the breakpoint detects cephalosporine resistance you immediately report the R or the I for the drug(s) you have tested. - Then you perform ESBL confirmation and characterisation tests and contact the appropriate infection control authorities. So how to proceed?
 you have tested. - Then you perform ESBL confirmation and characterisation tests and contact the appropriate infection control authorities. So how to proceed .")
18
New cephalosporine breakpoints in Enterobacteriaceae from EUCAST and CLSI Old breakpoints in white. New breakpoints in yellow.

19
Cefuroxime

20
Cefuroxime iv CommitteeS WT BSAC8 / 16S CA-SFM8 / 32S CRG4 / 16S and I DIN4 / 8S and I NWGA1 / 16I SRGA8 / 8S CLSI8/16S CLSI pending 4/8 (8 adj /8 or 16) S EUCAST*8/8 (pKD 4/8)S *for dosage: 1.5 g x 3
 S EUCAST*8/8 (pKD 4/8)S *for dosage: 1.5 g x 3")
21
Cefotaxime

22
CommitteeS WT BSAC1 / 1S CA-SFM4 / 32S CRG4 / 16S DIN2 / 8S NWGA1 / 4S SRGA0.5 / 1S CLSI8/32S CLSI pending1/2S EUCAST*1/2 (pKD 1/2)S *for dosage: 1 g x 3 and high dose 2 g x 3.
S *for dosage: 1 g x 3 and high dose 2 g x 3.")
23
Ceftriaxone CommitteeS BSAC1 / 1 CA-SFM4 / 32 CRG4 / 16 DIN4 / 16 NWGA1 / 16 SRGA0.5 / 1 CLSI8/32 CLSI pending1/2 EUCAST*1/2 (pKD 1/2) *for dosage: 1 g x 1 and high dose 2 g x 1.
 *for dosage: 1 g x 1 and high dose 2 g x 1.")
24
Ceftazidime

25
CommitteeS WT BSAC2 / 2S CA-SFM4 / 32S CRG4 / 16S DIN4 / 16S NWGA1 / 4S SRGA2 / 4S CLSI8/16S CLSI pending4/8S EUCAST*1/8 (pKD 4/8)S *for dosage: 1 g x 3 and high dose 2 g x 3 The S/I-breakpoint was decreased from 4 to 1 to detect clinically important ESBLs.
S *for dosage: 1 g x 3 and high dose 2 g x 3 The S/I-breakpoint was decreased from 4 to 1 to detect clinically important ESBLs.")
26
Cefepime

27
CommitteeS WT BSAC1 / 1S CA-SFM4 / 32S CRGNAS DIN4 / 16S NWGANAS SRGA0.5 / 1S CLSI8/16S CLSI pending8/16S EUCAST*1/8 (pKD 4/8)S *for dosage: 2 g x 3
S *for dosage: 2 g x 3")
29
EUCAST clinical breakpoints and dosage EUCASTDosage S≤S≤R>LowHigh Cefuroxime8 Adj 8-1.5 g x 3 Cefotaxime121 g x 32 g x 3 Ceftriaxone121 g x 12 g x 1 Ceftazidime181 g x 32 g x 3 Cefepime181 g x 32 g x 3 Adj Adjusted from 4 to 8 to avoid dividing wild type Enterobacteriaceae

30
Cefotaxime Ceftazidime Cefpodoxime

31
Cefotaxime Ceftazidime Cefpodoxime

32
Cefepime Cefotaxime Ceftazidime Cefoxitin Cefpodoxime

33
Cefepime Cefotaxime Ceftazidime

34
The end

Similar presentations



 Antimicrobial susceptibility testing in Europe - the role of national breakpoint committees and EUCAST Gunnar.>")

 surveillance (2009Q1-4) **** Data as.>")
.>")

 breakpoints – the impact on the BSAC recommendations Alasdair MacGowan Southmead Hospital BRISTOL.>")







>")

 surveillance, 2009 **** Data as of 01/12/2010.>")
