Download presentation
Presentation is loading. Please wait.

1
Date of Birth : Jakarta/19 November 1944QUALIFICATIONS: 1971Dokter, Fakultas Kedokteran Indonesia, Jakarta 1977Spesialis Bedah FKUI 1980Spesialis Urologi FKUI MEMBERSHIP: 1. Anggota Ikatan Dokter Indonesia 2. Anggota Ahli Bedah Indonesia 3. Anggota Ikatan Ahli Urologi Indonesia Rohani Sumardi

2
Current Management of Lower Urinary Track Symptom (LUTS) - BPH Rochani Sumardi
 - BPH Rochani Sumardi")
3
INTRODUCTION Lower urinary tract symptoms (LUTS) include storage and/or voiding disturbances which are very common in aging men.
 include storage and/or voiding disturbances which are very common in aging men.")
4
INTRODUCTION StorageVoiding Frequency Urgency Nocturia Incontinence Slow stream Incomplete emptying Intermitency Hesitancy Straining Terminal dribble

5
INTRODUCTION

6
Benign Prostatic Hyperplasia (BPH) is reserved for the histologic pattern the phrase describes. Benign Prostatic Enlargement (BPE) is used when there is gland enlargement. It is usually a presumptive diagnosis based on the size of the prostate.
 is used when there is gland enlargement. It is usually a presumptive diagnosis based on the size of the prostate..")
7
INTRODUCTION Benign Prostatic Obstruction (BPO) is used when obstruction has been proven by pressure flow studies or is highly suspected from flow rates, and if the gland is enlarged. Bladder Outlet Obstruction (BOO) is the generatic term for all forms of obstruction to the bladder outlet (eg urethral stricture), including BPO.
 is the generatic term for all forms of obstruction to the bladder outlet (eg urethral stricture), including BPO..")
8
INTRODUCTION

10
The standard (usual) patient is a man over the age of 50 years consulting a qualified health care provider. He has lower urinary tract symptoms (LUTS) suggestive of BPO and does not have any of the specified exclusion criteria
 suggestive of BPO and does not have any of the specified exclusion criteria.")
11
DIAGNOSIS History An adequate medical history should be obtained on the : -Nature abd duration of genito-urinary tract symptoms -Previous surgical procedures (in particular as they affect the genitourinary tract)
")
12
DIAGNOSIS -General health issues, sexual function history -Medications currently taken by the patient, and -The patient’s fitness for possibel surgical procedures

13
DIAGNOSIS Quantification of Symptoms : International Prostate Symptom Score (I-PSS) and Qualitu of life Assessment (QoL) When patients present with LUTS suggesting underlying BPO, the use of a short, self- administered questionnaire in the appropirate language for the objective documentation of symptom frequency from the patient’s perspective is highly recommended.
 and Qualitu of life Assessment (QoL) When patients present with LUTS suggesting underlying BPO, the use of a short, self- administered questionnaire in the appropirate language for the objective documentation of symptom frequency from the patient’s perspective is highly recommended.")
14
DIAGNOSIS a)IPSS The I-PSS questionnaire is designed for patient self-administration. The answers are assigned

17
DIAGNOSIS points from 0 - 5. Each question allows the patient to choose one out of six answers indi cating the frequency of a particular symptom. The total score can therefore range from 0 to 35 points (asymptomatic to very symptomatic).
..")
18
DIAGNOSIS The symbol for Symptom Score is I-PSS [0-35] Patients can be classified as follows: 0 - 7= mildly symptomatic 8 - 19= moderately symptomatic 20 - 35 = severely symptomatic
![DIAGNOSIS The symbol for Symptom Score is I-PSS [0-35] Patients can be classified as follows: 0 - 7= mildly symptomatic = moderately symptomatic = severely symptomatic](http://images.slideplayer.com/10/2813185/slides/slide_18.jpg "DIAGNOSIS The symbol for Symptom Score is I-PSS [0-35] Patients can be classified as follows: 0 - 7= mildly symptomatic = moderately symptomatic = severely symptomatic")
19
DIAGNOSIS The Quality of Life Assessment (QoL) used in conjunction with the I-PSS is a single question asking the patient how he would feel about tolerating his current level of symptoms for the rest of his life. The answers to this question range from delighted to terrible, or 0 to 6 points. Although this single question cannot capture the global impact of LUTS on quality of life, it may serve as a valuable starting point for a doctor- patient conversation concerning this important issue.

20
DIAGNOSIS The symbol for the response to the Quality of Life Question is Qol, [0-6] At a minimum, clinicians are encouraged to ask the single global question in the I-PSS to begin engaging their patients in a discussion about the impact of their symptoms on their lives. Clinicians may want to consider using other question sets in their practices to assess in more detail issues of continence, sexual function, and impact of symptoms on health (outlined in the report of Committee 6).
![DIAGNOSIS The symbol for the response to the Quality of Life Question is Qol, [0-6] At a minimum, clinicians are encouraged to ask the single global question in the I-PSS to begin engaging their patients in a discussion about the impact of their symptoms on their lives.](http://images.slideplayer.com/10/2813185/slides/slide_20.jpg "Clinicians may want to consider using other question sets in their practices to assess in more detail issues of continence, sexual function, and impact of symptoms on health (outlined in the report of Committee 6)..")
21
DIAGNOSIS Physical Examination and Digital Rectal Examination (DRE) A focused physical examination should be performed to assess: the suprapubic area to rule out bladder distension, overall motor and sensory function. A digital rectal examination (DRE) should be performed to evaluate the anal sphincter tone and prostate gland with regard to approximate size, consistency, shape, and abnormalities suggestive for prostate cancer.
 should be performed to evaluate the anal sphincter tone and prostate gland with regard to approximate size, consistency, shape, and abnormalities suggestive for prostate cancer..")
22
DIAGNOSIS Urinalysis The urine should be analysed using a dipstick test, with or without examination of the urina ry sediment after centrifugation, to determine if the patient has : haematuria, proteinuria, pyuria, or other pathological findings (e.g. glucose)
.")
23
DIAGNOSIS Serum Prostate Specific Antigen (PSA) Althought BPH does not lead to prostate cancer, le BPH age group are also at risk for cancer. Measurement of the serum addition to DRE clearly increases the rate of prostate cancer over DRE alone. Serum PSA measurement is recommended in the initial evaluation of patients with an anticipated life expectancy of over 10 years in whom the diagnosis of prostate cancer once established would change the treatment plan.

24
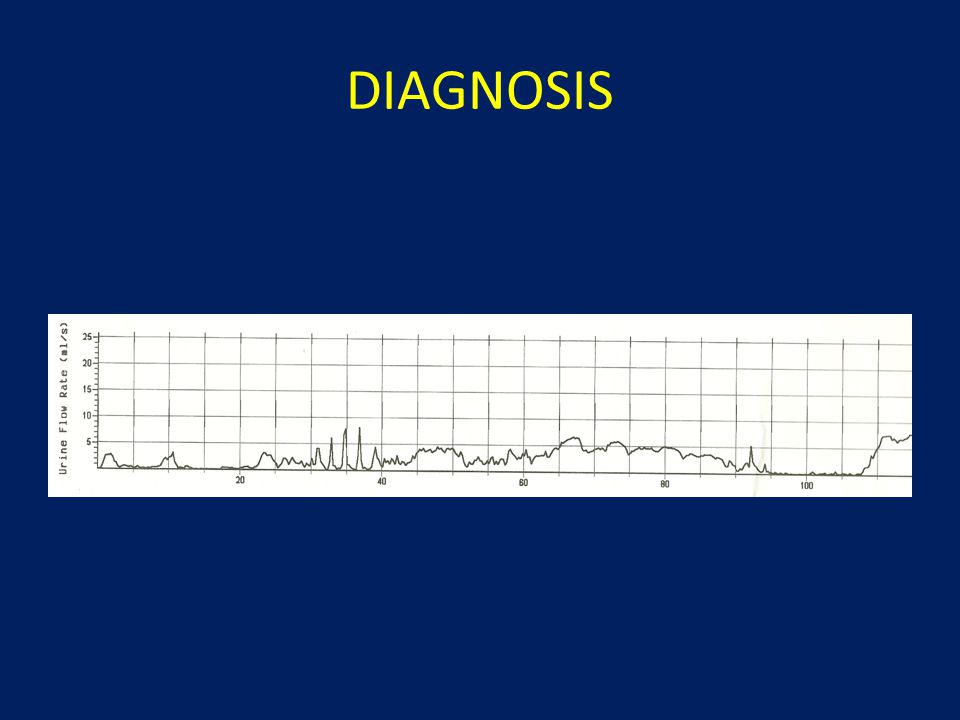
DIAGNOSIS Flow Rate Recording Urinary flow rate measurement is recommended in the initial diagnostic assessment and during or after treatment, to determine response. Because of the non- invasive nature of the test and its clinical value, it should be performed prior to embarking on any active therapy.

25
DIAGNOSIS

26
Maximum urinary flow rate (Qmax) is the best single measure ; but a low Q max does not distinguish between obstruction and decreased bladder contractility.
 is the best single measure ; but a low Q max does not distinguish between obstruction and decreased bladder contractility.")
27
DIAGNOSIS Because of the great intra individual variability and the volume dependency of the Qmax, at least two flow rates, both with a volume ideally of > 150 ml voided urine, should be obtained. If such a voiding volume cannot he obtained by the patient despite repeated recordings, the Qmax results at available voiding volumes should be considered

28
DIAGNOSIS The Qmax should be read manually as many automatic flow rate recording devices tend to overestimate Qmax due to tchnical artifacts

29
DIAGNOSIS

31
Residual Urine The determination of post-void residual urine is recommended in the initial diagnostic assessment of the patient and during subsequent monitoring as a safety parameter. The determination is best performed by noninvasive transabdominal ultrasonography. Because of the marked intra-individual variability of residual urine volume, the test should be repeated to improve precision, if the first residual urine volume is significant and suggests a change in the treatment plan.

32
DIAGNOSIS

36
Diagnostic Tests OPTIONAL TESTS 1. Pressure-Flow Studies 2. Imaging of the Prostate by Transabdominal or Transrectal Ultrasound (TRUS) 3. Imaging of the Upper Urinary Tract by Ultrasonography or Intravenous Urography (IVU) 4. Endoscopy of the Lower Urinary Tract
 3. Imaging of the Upper Urinary Tract by Ultrasonography or Intravenous Urography (IVU) 4. Endoscopy of the Lower Urinary Tract.")
37
INDICATION FOR SURGICAL TREATMENT 1.urinary retention (inability to urinate after at least one attempt at catheter removal) 2.recurrent gross haematuria due to BPE 3.renal failure due to BPO 4.bladder stones due to BPO 5.recurrent urinary tract infections due to BPO, or 6.large bladder diverticula, TREATMENT
 2.recurrent gross haematuria due to BPE 3.renal failure due to BPO 4.bladder stones due to BPO 5.recurrent urinary tract infections due to BPO, or 6.large bladder diverticula, TREATMENT")
38
Treatment options Watchful waiting Medication Alpha Blocker: tamsulosin, terazosin, alfuzosin,doxazosin 5 ARI: finasteride, dutasteride min 6 mo treatment Surgical approaches – Minimal invasive (TURP, TUIP, Laser, TUMT, TUNA) – Invasive “ open ” procedures : Retropubic, Trans vesical
 – Invasive open procedures : Retropubic, Trans vesical")
39
Treatment Options for BPH - Drug therapy Class of DrugGeneric NameBrand name Alpha Blocker drug AlfuzosinXatral TerazosinHytrin DoxazosinCardura PrazosinMinipress TamsulosinHarnal Anti androgen drug ( 5-ARI) FinasterideProscar DutasteridAvodart Phytofarmaka Serenoa repens Pygeum africanum
 FinasterideProscar DutasteridAvodart Phytofarmaka Serenoa repens Pygeum africanum")
40
Alpha Blockers

41
P< 0.001 Narayan.P, et al. vol 5. The J of App Res. No.2, 2005 Reduction in BPH symptom severity was significantly greater after 4 weeks of treatment with tamsulosin than with terazosin

42
Reduction in BPH symptom severity was significantly greater after 6 weeks of treatment with tamsulosin than with doxazosin Djoko Rahardjo, Doddy M Soebadi, Suwandi Sugandi, Ponco Birowo, Wahjoedjati, Irfan Wahyudi, International Journal of Urology (2006) 13, 1405–1409
 13, 1405–1409")
43
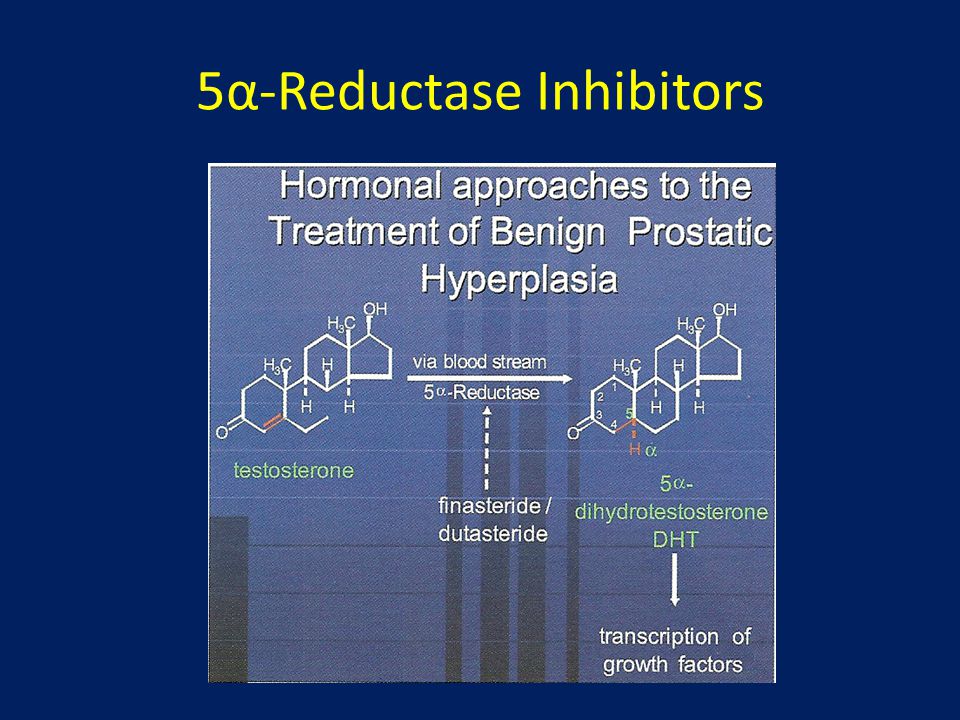
5α-Reductase Inhibitors AdvantagesDisadvantages Reduce prostate size by 20–30% Improve I-PSS by ~15% Moderately improve urinary flow rates Reduce risk of developing urinary retention Reduce requirement for surgery Long-term efficacy Not recommended for patients with prostate size <40ml Side effects of reduced sexual function affect up to 12% of patients Reduce serum levels of PSA, which may mask detection of prostate cancer Take 6 months to achieve maximum efficacy No effect on smooth muscle component of BPH de la Rosette J, et al, 2002. EAU guidelines on benign prostatic hyperplasia.

44
5α-Reductase Inhibitors

46
CONCLUSION 1.Prevalance LUTS-BPH increas with age 2.Diagnostic test include - highly recommended test : history, I-PSS, QoL, DRE and Urinalysis -recommended test : renal function test, PSA, Flow Rate and Residual Urine 3. Treatment option : -Watchful waiting -Medication : alpha blockers, 5 alpha reductation inhibitor - Surgical treatment

47
THANK YOU

Similar presentations







 Bob White, AIM-IRS ABMTS Milwaukee, WI.>")















 in elderly males>")

