Download presentation
Presentation is loading. Please wait.

1
Phase II Study of Temozolomide and Thalidomide in Patients With Metastatic Neuroendocrine Tumors J Clin Oncol. 2006 Jan 20;24(3):401-6. Vs 劉俊煌 CR 周益聖 財團法人台灣癌症臨床研究發展基金會
: Vs 劉俊煌 CR 周益聖 財團法人台灣癌症臨床研究發展基金會.")
2
Outline Classification and grading of NET Introduction to temozolomide Inclusion and exclusion criteria Regimen dosage and adjustment Response assessment Result Disscusion Conclusion

5
Endocr Relat Cancer. 2004 Mar;11(1):1-18.
:1-18.")
7
Outline Classification and grading of NET Introduction to temozolomide Inclusion and exclusion criteria Regimen dosage and adjustment Response assessment Result Disscusion Conclusion

8
Cancer Chemother Pharmacol (2009) 64:647–655
 64:647–655")
10
J Clin Oncol 25:4127-4136

11
Temozolomide dosing regimens for malignant gliomas J Clin Oncol 25:4127-4136

12
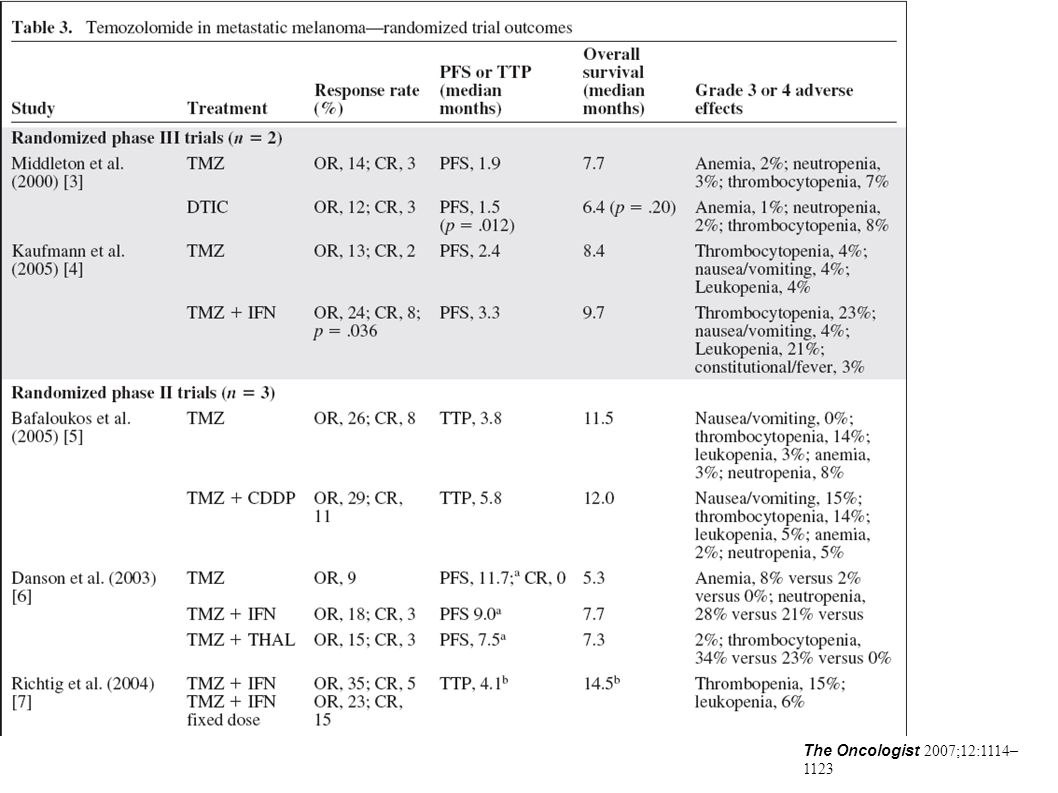
The Oncologist 2007;12:1114– 1123

14
Outline Classification and grading of NET Introduction to temozolomide Inclusion and exclusion criteria Regimen dosage and adjustment Response assessment Result Disscusion Conclusion

15
Inclusion (1) Histologically confirmed, locally unresectable or metastatic neuroendocrine tumors Prior treatment with chemotherapy, other than DTIC, temozolomide, or thalidomide, was permitted ECOG performance status of 0, 1, or 2 Life expectancy > 12 weeks Adequate renal function (serum creatinine < 1.5 * the upper limit of normal [ULN])
![Inclusion (1) Histologically confirmed, locally unresectable or metastatic neuroendocrine tumors Prior treatment with chemotherapy, other than DTIC, temozolomide, or thalidomide, was permitted ECOG performance status of 0, 1, or 2 Life expectancy > 12 weeks Adequate renal function (serum creatinine < 1.5 * the upper limit of normal [ULN])](http://images.slideplayer.com/10/2804001/slides/slide_15.jpg "Inclusion (1) Histologically confirmed, locally unresectable or metastatic neuroendocrine tumors Prior treatment with chemotherapy, other than DTIC, temozolomide, or thalidomide, was permitted ECOG performance status of 0, 1, or 2 Life expectancy > 12 weeks Adequate renal function (serum creatinine < 1.5 * the upper limit of normal [ULN])")
16
Inclusion (2) Adequate hepatic function (total and direct bilirubin < 2 * the ULN) ALT and AST < 5 * the ULN, and alkaline phosphatase < 2 * the ULN or < 5 * the ULN in the setting of liver metastases Adequate bone marrow function (absolute neutrophil count >1,500/mm3, platelets > 100,000/mm3, hemoglobin >9 g/dL)
 Adequate hepatic function (total and direct bilirubin < 2 * the ULN) ALT and AST < 5 * the ULN, and alkaline phosphatase < 2 * the ULN or < 5 * the ULN in the setting of liver metastases Adequate bone marrow function (absolute neutrophil count >1,500/mm3, platelets > 100,000/mm3, hemoglobin >9 g/dL)")
17
Exclusion Clinically apparent CNS metastases or carcinomatous meningitis History of myocardial infarction 6 months before protocol treatment History of major surgery within 2 weeks before treatment initiation HIV infection or AIDS-related illness Other serious medical or psychiatric illness Insufficient recovery from toxicities of prior therapies Pregnant or lactating.

18
Outline Classification and grading of NET Introduction to temozolomide Inclusion and exclusion criteria Regimen dosage and adjustment Response assessment Result Disscusion Conclusion

19
Treatment Program Temozolomide 150 mg/m2 days 1 to 7 and days 15 to 21 Thalidomide daily starting dose of 200 mg Every 28 days

20
Temozolomide adjustment Hold if ANC less than 1,000/mm3 Plt less than 50,000/mm3 all nonhematologic toxicities with National Cancer Institute Common Toxicity Criteria grade 2 or higher Not resumed until full hematologic recovery On recovery, dose reduction of 50 mg/m2 Discontineud if Unable to resume therapy within 3 weeks Unacceptable toxicity levels

21
Thalidomide adjustment Increased weekly by 100 mg until a maximum dose of 400 mg Before escalation Toxicity >> reduced by 100 mg/d No improvement within 7days >> further reduced by 50 mg Not tolerate 50 mg/d >> removed from study After escalation Toxicity >> decreased by 100 mg not resolved to grade 1 within 7 days >> further reduced by 100 mg P't at a dose of 100 mg >> reduction to 50 mg daily

22
Outline Classification and grading of NET Introduction to temozolomide Inclusion and exclusion criteria Regimen dosage and adjustment Response assessment Result Disscusion Conclusion

23
Response assessment Every 8 weeks after initiation of treatment Computed tomography scan P't with complete [CR] or partial response [PR] or stable disease remained on treatment until progression CR disappearance of all target lesions at least 4 weeks
![Response assessment Every 8 weeks after initiation of treatment Computed tomography scan P t with complete [CR] or partial response [PR] or stable disease remained on treatment until progression CR disappearance of all target lesions at least 4 weeks](http://images.slideplayer.com/10/2804001/slides/slide_23.jpg "Response assessment Every 8 weeks after initiation of treatment Computed tomography scan P t with complete [CR] or partial response [PR] or stable disease remained on treatment until progression CR disappearance of all target lesions at least 4 weeks")
24
Response assessment PR decrease of more than 30% in the sum of the largest perpendicular diameters of all measurable lesions at least 4 weeks without progression of any nonmeasurable sites Without new lesions. Progressive disease increase of 20% or more in the sum of longest diameters of target lesions one or more new lesions

25
Response assessment Stable disease: Neither PR, nor progressive disease Biochemical response secondary end point PR:decrease in chromogranin A by 50% or more Stable: <50 % decrease or <25% increase

26
Outline Classification and grading of NET Introduction to temozolomide Inclusion and exclusion criteria Regimen dosage and adjustment Response assessment Result Disscusion Conclusion

28
Duration of Treatment 29 patients received treatment for a median of 7.3 months (range, 1 to 23 months) 1 patient required dose reduction of temozolomide due to thrombocytopenia 16 patients required dose reductions for thalidomide- related toxicities 14 required dose reduction to 100 mg 2 required dose reductions to 50 mg daily 9 patients continued thalidomide at their starting dose of 200 mg 4 patients able to undergo dose escalation to 400 mg Median thalidomide dose 100 mg/d
 1 patient required dose reduction of temozolomide due to thrombocytopenia 16 patients required dose reductions for thalidomide- related toxicities 14 required dose reduction to 100 mg 2 required dose reductions to 50 mg daily 9 patients continued thalidomide at their starting dose of 200 mg 4 patients able to undergo dose escalation to 400 mg Median thalidomide dose 100 mg/d")
29
Treatment-related toxicities resulting in discontinuation: neuropathy (11 patients,38%, 6 pt's persist > 3 wks), infection (four patients), thrombocytopenia (four patients), neutropenia (one patient), rash (one patient). Infections included: Pneumocystis carinii pneumonia (one patient), disseminated varicella zoster virus (one patient), staphylococcal sepsis (one patient), cutaneous herpes zoster (one patient)
, disseminated varicella zoster virus (one patient), staphylococcal sepsis (one patient), cutaneous herpes zoster (one patient).")
30
Median time to treatment discontinuation for toxicity :8.4 months (range, 1.5 to 7.5 months)
")
32
Median duration of response was 13.5 months (range, 2 to 31 months)
")
33
Progression-free survival Overall survival 1-year survival rate: 79% 2-year survival rate: 61%

34
Outline Classification and grading of NET Introduction to temozolomide Inclusion and exclusion criteria Regimen dosage and adjustment Response assessment Result Disscusion Conclusion

35
Discussion Overall objective radiologic response rate of 25%(CR+PR) Biochemical response rate of 40% 2-year survival rate of 61% Unique toxicities:neuropathy(38%) and selective lymphopenia(69%)
 Biochemical response rate of 40% 2-year survival rate of 61% Unique toxicities:neuropathy(38%) and selective lymphopenia(69%)")
36
Carcinoid tumor Objective response rates of streptozocin-based regimens: 16% to 33% J Clin Oncol 2:1255-1259, 1984 Cancer Clin Trials2:327-334, 1979 J Clin Oncol 23:4897-4904, 2005 Pancreatic endocrine tumors Combined biochemical and radiologic response rate of. Streptozocin and doxorubicin : 69% N Engl J Med 326:519-523, 1992 Overall response rate of retrospective study of streptozocin, fluorouracil, and doxorubicin:39% J Clin Oncol 22:4762-4771, 2004 Cancer 86:944-948, 1999 Am JClin Oncol 27:485-488, 2004

37
CR+PR Carcinoid tumor 1/15 (7%) Pancreatic endocrine tumors 5/11(45%) Pheochromocytoma 1/3 (33%)
 Pancreatic endocrine tumors 5/11(45%) Pheochromocytoma 1/3 (33%)")
38
high proportion (55%) removed for toxicity Median time to treatment discontinuation for treatment- related toxicity:8.4 months 4 patients experienced progressive disease while receiving study therapy Prophylaxis against P carinii pneumonia and herpes simplex virus should be utilized
 removed for toxicity Median time to treatment discontinuation for treatment- related toxicity:8.4 months 4 patients experienced progressive disease while receiving study therapy Prophylaxis against P carinii pneumonia and herpes simplex virus should be utilized")
39
Outline Classification and grading of NET Introduction to temozolomide Inclusion and exclusion criteria Regimen dosage and adjustment Response assessment Result Disscusion Conclusion

40
Combination of temozolomide and thalidomide seems to be an active oral regimen for the treatment of metastatic neuroendocrine tumors and alternative to intravenous regimens More active in pancreatic endocrine tumors than in carcinoid tumors. Further studies to more precisely assess the relative efficacy of this regimen in pancreatic endocrine and carcinoid tumors Also to assess the relative contributions of temozolomide and thalidomide to the antitumor activity

Similar presentations











,as adjuvant therapy following resection of AJCC stage IIB.>")



 46, 475–484 Best Practice & Research Clinical haematology (2007). 295- 310 Current Opinion.>")





 M.P. SUNYACH, D. PEROL, N. PENEL, P.>")

 vs Lenalidomide and Dexamethasone (Rd) in Subjects.>")

: A Trial of the Eastern Cooperative Oncology Group: Berlin J 1, Powell.>")