Download presentation
Presentation is loading. Please wait.

1
Jette R Hogenmiller, PhD, MN, FNPc, APRN, CDE, TNCCc
Preventing Orthopedic Surgical Site Infections (SSI) through a Best Practice Bundle Presenter Jette R Hogenmiller, PhD, MN, FNPc, APRN, CDE, TNCCc Current Position: Chief Nursing Officer, Haxtun Hospital District; Haxtun, Colorado Background: Infection Preventionist , Family Nurse Practitioner & Oncology Clinical Nurse Specialist Disclosures: Health, Innovation & Research, LLC 3M sponsored speaker
 through a Best Practice Bundle. Presenter. Jette R Hogenmiller, PhD, MN, FNPc, APRN, CDE, TNCCc. Current Position: Chief Nursing Officer, Haxtun Hospital District; Haxtun, Colorado. Background: Infection Preventionist , Family Nurse Practitioner & Oncology Clinical Nurse Specialist. Disclosures: Health, Innovation & Research, LLC. 3M sponsored speaker.")
2
Objectives, identify: The impact of surgical site infection (SSI) on Orthopedic joint surgery outcomes (e.g. patient, financial) Potential sources of Orthopedic joint surgery SSI’s Scientifically based SSI prevention strategies & application to Orthopedic joint surgery Strategies that might be implemented in your setting to further reduce Orthopedic joint surgery SSI’s

3
Presentation Outline Significance of SSI in Orthopedic joint surgeries
Is it time for a “SSI Prevention Bundle” in Orthopedics? How does the APIC “Guide to the Elimination of Orthopedic Surgical Site Infections” provide us direction as Infection Preventionist’s? = What is the evidence that guides us in SSI prevention? Review of a bundle used to reduce Orthopedic surgeries & evidence for impact on outcomes Next steps, what are they… on our journey to zero for SSI’s?

4
This is the face of our patients… health care consumer.
This is why we have a passion about being an Infection Preventionist….we want to protect those who enter our doors… they are innocent, no matter their age. They & their families entrust their lives in our care.

5
Surgical Site Infections (SSI)
SSI account for ~ 15% of healthcare associated infections (HAI’s) ~ 500K SSI annually among 44M inpatient surgical procedures Mortality of infected vs. uninfected cases (7.8% vs. 3.5%) ICHE 1999; 20:725 Risk factors: age, gender, nutritional status, diabetes, & obesity ICHE 1999; 20:250 Skin preparation of patient/surgical team CDC category IB Am J Inf Dis 2007; 3:51 From Guide to the Elimination of Orthopedic Surgical Site Infections. (2010), APIC
 ~ 500K SSI annually among 44M inpatient surgical procedures. Mortality of infected vs. uninfected cases. (7.8% vs. 3.5%) ICHE 1999; 20:725. Risk factors: age, gender, nutritional status, diabetes, & obesity. ICHE 1999; 20:250. Skin preparation of patient/surgical team. CDC category IB. Am J Inf Dis 2007; 3:51. From Guide to the Elimination of Orthopedic Surgical Site Infections. (2010), APIC.")
6
Significance of SSI’s in Orthopedic Joint Surgeries
What does having an SSI mean to a person & society?

7
SSI Financial Costs Guide to the Elimination of Orthopedic Surgical Site Infections. (2010), APIC
$38,000 vs. $11,255 –> infected vs. non-infected fixation or hemi- arthroplasty (Pollard, et. al, 2006) $50,000 to tx SSI (Lentino, 2003) MRSA infections more costly than non-MRSA. (Pollard et al.) $250 million total knee & hip replacement SSIs, annual US cost of total joint replacement infections (Kuper, 2008) 2.8 time higher costs for revision of a total joint due to infection than cost of revision for aseptic loosening & 4.8 times higher than costs associated with primary total hip arthroplasty (Kuper, 2008)
 $50,000 to tx SSI (Lentino, 2003) MRSA infections more costly than non-MRSA. (Pollard et al.) $250 million total knee & hip replacement SSIs, annual US cost of total. joint replacement infections (Kuper, 2008) 2.8 time higher costs for revision of a total joint due to infection than cost of revision for aseptic loosening & 4.8 times higher than costs associated with primary total hip arthroplasty (Kuper, 2008)")
8
SSI Morbidity Costs Guide to the Elimination of Orthopedic Surgical Site Infections. (2010), APIC
“Total hip arthroplasty revision due to infection results in significantly more hospitalizations increased total length of stay; # of operative procedures; and outpatient visits & charges additional complications than revision due to aseptic loosening of the prosthesis“ (APIC, 2010) _____________________________________________________________ “… increased median initial length of stay - total # of hospitalizations # of surgical procedures, - total length of stay, & cost - substantial reduction in quality of life 1 yr later Whitehouse, et. al (2002) [orthopedic procedures, incl. open reduction of fracture, fusion, laminectomy & joint replacement; pairwise matched (1:1) case-control study within a cohort (n=59 cases, 11/19% had joint replacement surgery)
 _____________________________________________________________. … increased median initial length of stay. - total # of hospitalizations - # of surgical procedures, - total length of stay, & - cost. - substantial reduction in quality of life 1 yr later. Whitehouse, et. al (2002) [orthopedic procedures, incl. open reduction of fracture, fusion, laminectomy & joint replacement; pairwise matched (1:1) case-control study within a cohort (n=59 cases, 11/19% had joint replacement surgery)")
9
SSI Morbidity & Mortality Costs Guide to the Elimination of Orthopedic Surgical Site Infections. (2010), APIC increased length of stay, including readmission within 90 days of surgery (13 vs 4 days) mean of 9.31 days of hospitalization attributable to infection higher 1-year postoperative mortality (17% vs 4%) for infected vs non-infected Lee et al. (2006) [Sample > 64 years of age, nested-case control; 15,218 -> hip & knee replacement, open reduction of fracture, other joint replacement, spinal fusion & laminectomy]
 mean of 9.31 days of hospitalization attributable to infection. higher 1-year postoperative mortality (17% vs 4%) for infected vs non-infected. Lee et al. (2006) [Sample > 64 years of age, nested-case control; 15,218 -> hip & knee replacement, open reduction of fracture, other joint replacement, spinal fusion & laminectomy]")
10
Orthopedic Surgical Site Infection Rates

11
Incidence SSI Pooled means of SSI rates by operative inpatient procedure & risk index categories, 2006 through 2008 Procedure Index Category # Procedures # of SSI’s Pooled Mean Hip prosthesis 49,576 334 0.67 1 65,046 938 1.44 2,3 15,769 379 2.4 Knee prosthesis 70,675 409 0.58 79,653 786 0.99 20,855 333 1.60 “…NHSN report, a large U.S. database for HAI aggregation & comparison report titled: “Data Summary for through 2008,” issued December 2009, SSI rates for hip replacement & knee replacement” APIC, 2010 Guide to the Elimination of Orthopedic Surgical Site Infections

12
Basic SSI Risk Index The index used in NHSN assigns surgical patients into categories based on the presence of three major risk factors: “Operation lasting more than the duration cut point hours, where the duration cut point is the approximate 75th percentile of the duration of surgery in minutes for the operative procedure, rounded to the nearest whole number of hours. Contaminated (Class 3) or Dirty/infected (Class 4) wound class. ASA classification of 3, 4, or 5. The patient’s SSI risk category is simply the number of these factors present at the time of the operation.”
 or Dirty/infected (Class 4) wound class. ASA classification of 3, 4, or 5. The patient’s SSI risk category is simply the number of these factors present at the time of the operation.")
13
Surgical Wound Classification (APIC, 2010)
")
15
Significant “pain” provides for ability to take bold action!
What was “Our” Hip & Knee SSI rate? Actions taken: stopped surgery, performed comprehensive assessment, and multi-disciplinary team convened to develop a focused bundle & intervention plan. Discuss our Hip & Knee SSI rate…. Publically reported. Significant “pain” provides for ability to take bold action!

16
Is there a SSI Ortho prevention bundle/path to get us to zero?
Getting to Zero Is there a SSI Ortho prevention bundle/path to get us to zero? YES

18
Surgical Site Infection
Allan Morrison, Jr, MD, MSC, FACP, FIDSA, FSHEA [Animated slide—mouse click to bring up pictures] Enturia102407 18

20
What do we know about the cause of
Surgery/Orthopedic SSI’s?

21
SSI: Primary Risk Factors
Endogenous microorganisms Skin-dwelling microorganisms Most common source S aureus most common isolate Exogenous microorganisms Surgical personnel OR environment All tools, instruments, and materials Most surgical site infections (SSIs) are caused by skin-dwelling microorganisms from the patient. Staphylococcus aureus is the most common isolate associated with the development of surgical site infections. Exogenous sources of pathogens that contribute to surgical site infection include surgical personnel, particularly surgical team members, who carry microorganisms on their person. The operating room environment, including the air itself, may be contaminated with microorganism that are transferred to the patient. All tools, instruments, and materials brought into the sterile field may harbor pathogens if they are not adequately sterilized. Reference Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR. The hospital infection control practices advisory committee. Guidelines for prevention of surgical site infection, Hospital Infection Control Practices Advisory Committee. Infect Control Hosp Epidemiol. 1999;20(4): Mangram AJ, et al. The hospital infection control practices advisory committee. Guidelines for prevention of surgical site infection. Infect Control Hosp Epidemiol. 1999;20(4): Enturia102407 21
 are caused by skin-dwelling microorganisms from the patient. Staphylococcus aureus is the most common isolate associated with the development of surgical site infections. Exogenous sources of pathogens that contribute to surgical site infection include surgical personnel, particularly surgical team members, who carry microorganisms on their person. The operating room environment, including the air itself, may be contaminated with microorganism that are transferred to the patient. All tools, instruments, and materials brought into the sterile field may harbor pathogens if they are not adequately sterilized. Reference. Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR. The hospital infection control practices advisory committee. Guidelines for prevention of surgical site infection, Hospital Infection Control Practices Advisory Committee. Infect Control Hosp Epidemiol. 1999;20(4): Mangram AJ, et al. The hospital infection control practices advisory committee. Guidelines for prevention of surgical site infection. Infect Control Hosp Epidemiol. 1999;20(4): Enturia")
22
SSI: Modifiable Risks Glucose control Preoperative CHG shower
Appropriate hair removal Hand hygiene Skin antisepsis [[animated slide—mouse click for each text box]] The Guidelines for Prevention of Surgical Site Infection developed by the Hospital Infection Control Practices Advisory Committee of the CDC underscores the risk to patients of morbidity and mortality associated with surgical site infections (SSI). Specific guidelines for prevention of SSIs include:1,2 Ensuring glucose control in diabetic patients Having the patient shower with an antiseptic prior to surgery. Chlorhexidine is associated with a nine-fold decrease in bacterial colony counts, compared to less than two-fold decrease using povidone-iodine. Leaving hair intact. Shaving causes microabrasions that may provide access for microorganisms. The risk of SSI is lower with clipping hair or the use of depilatories, but each produces greater risk of infection than keeping hair intact. Proper hand and forearm antisepsis by the surgical team and exclusion of members who may be ill or infected to prevent exogenous contamination Preoperative skin antisepsis Prophylactic treatment with an antimicrobial initiated immediately prior to surgery to reduce microbial burden Ensuring normal body temperature; intraoperative hypothermia has been associated with higher SSI risk References Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR. Guideline for prevention of surgical site infection, Hospital Infection Control Practices Advisory Committee. Infect Control Hosp Epidemiol. 1999;20(4): 5 Million lives. Institute for Healthcare Improvement. Available at: Accessed on February 8, 2007. Antimicrobial prophylaxis Normothermia Mangram AJ, et al. The hospital infection control practices advisory committee. Guidelines for prevention of surgical site infection. Infect Control Hosp Epidemiol. 1999;20(4): 5 Million lives. Institute for Healthcare Improvement. Available at: Accessed on February 8, 2007. Enturia102407 22
. Specific guidelines for prevention of SSIs include:1,2. Ensuring glucose control in diabetic patients. Having the patient shower with an antiseptic prior to surgery. Chlorhexidine is associated with a nine-fold decrease in bacterial colony counts, compared to less than two-fold decrease using povidone-iodine. Leaving hair intact. Shaving causes microabrasions that may provide access for microorganisms. The risk of SSI is lower with clipping hair or the use of depilatories, but each produces greater risk of infection than keeping hair intact. Proper hand and forearm antisepsis by the surgical team and exclusion of members who may be ill or infected to prevent exogenous contamination. Preoperative skin antisepsis. Prophylactic treatment with an antimicrobial initiated immediately prior to surgery to reduce microbial burden. Ensuring normal body temperature; intraoperative hypothermia has been associated with higher SSI risk. References. Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR. Guideline for prevention of surgical site infection, Hospital Infection Control Practices Advisory Committee. Infect Control Hosp Epidemiol. 1999;20(4): Million lives. Institute for Healthcare Improvement. Available at: Accessed on February 8, Antimicrobial prophylaxis. Normothermia. Mangram AJ, et al. The hospital infection control practices advisory committee. Guidelines for prevention of surgical site infection. Infect Control Hosp Epidemiol. 1999;20(4): Million lives. Institute for Healthcare Improvement. Available at: Accessed on February 8, Enturia")
27
Comprehensive Assessment
System Processes - Antibiotic usage & timing - Air system/HVAC Blood glucose control - Cleaning of OR Instrument/case opening - MRSA colonization OR apparel - Patient temperature, pre, intra & postoperative - Skin preparation Sterilization -Team work Other Client history/behaviors Diabetes Demographics Preop preparation/education - Smoking - Other

28
Seeking the Evidence Clinical Experience
-For-profit, joint venture Orthopedic hospital (~5500+ cases annually & ~30 surgeons -Multi-state, multiple hospital system -Inner-city, safety-net, level I trauma center, multi-hospital system Conferences – local, state, national & international APIC – IDSA – SHEA & others E Patchen Dellinger, MD. University of Washington - Laura Prokuski, MD, University of Wisconsin -Others Research Review/Professional Society Guidelines

29
APIC “Guide to the Elimination of Orthopedic SSI’s”
Providing guidance for Infection Preventionists.

30
SHEA Practice Recommendations
“Strategies to prevent surgical site infections in acute care hospital” ICHE October 2008, vol. 29, supplement 1

31
Review of variety of well-known & less well-known evidence
Hair removal Surgical Instrument Table Anesthesia work space Equipment (e.g. Tourniquets)
")
33
SSI: Skin Preparations
Agent Gram Gram- Mtb Fungi Virus positive negative bacteria bacteria Chlorhexidine E G P F G Alcohol E E G G G Iodine/iodophors E G G G G PCMX G F F F F Triclosan G G G P U E = excellent; F = fair; G = good; P = poor; U = unknown Am J Infect Dis 2007; 3(1):51-61
:")
35
Sterilization wrap inspections do not adequately evaluate instrument sterility. Clin Orthop Relat Res Sep;462: Waked WR, Simpson AK, Miller CP, Magit DP, Grauer JN. See references for full abstract. Orthopaedic procedures rely on strict sterilization techniques to prevent SSI Surgical instrument trays are wrapped for sterilization & these wraps routinely are inspected by OR personnel to evaluate for breaches before use Method: 90 sterilization wraps divided into groups with no defect & with 6 sizes of defects ranging from 1.1 to 10.0 mm in diameter. Puncture-type defects were created using nails of known diameter. All wraps were evaluated by medical personnel for evidence of a breach. Detection rates ranged from 6.7% to 96.7% from the smallest to largest defects, respectively. The potential for bacterial transmission thru wrap defects also was evaluated & contaminated nails of the smallest size transmitted bacterial contaminants thru the wrap during the creation of puncture defects. Thus, substantial perforations in sterilization wraps frequently are missed when evaluated with commonly used techniques. Defects with a diameter approximately that of a pencil (6.7 mm) were missed 18% of the time, although contamination can be transmitted by a nail with the diameter of a pin (1.1 mm). These results raise questions about a common screening method.
 were missed 18% of the time, although contamination can be transmitted by a nail with the diameter of a pin (1.1 mm). These results raise questions about a common screening method.")
36
Study of surgical instruments contamination by bacteria from air during the operation Zhonghua Hu Li Za Zhi Dec;31(12): [Article in Chinese] Yin SH, Xu SH, Bo YC. See reference for full abstract Routinely sterilized surgical instruments were divided into two groups and put on the same instrument table, one group was covered with dressing and the other was exposed to the air. The samples were collected at 30 min, 60 min, and 90 min respectively after operation began and bacterium culture was done. The results showed that the general air contamination rate of the exposed group was times higher than that of the covered one
![Study of surgical instruments contamination by bacteria from air during the operation Zhonghua Hu Li Za Zhi Dec;31(12): [Article in Chinese] Yin SH, Xu SH, Bo YC. See reference for full abstract](http://slideplayer.com/slide/2803829/10/images/36/Study+of+surgical+instruments+contamination+by+bacteria+from+air+during+the+operation+Zhonghua+Hu+Li+Za+Zhi+Dec%3B31%2812%29%3A+%5BArticle+in+Chinese%5D+Yin+SH%2C+Xu+SH%2C+Bo+YC.+See+reference+for+full+abstract.jpg "Routinely sterilized surgical instruments were divided into two groups and put on the same instrument table, one group was covered with dressing and the other was exposed to the air. The samples were collected at 30 min, 60 min, and 90 min respectively after operation began and bacterium culture was done. The results showed that the general air contamination rate of the exposed group was 1.18 times higher than that of the covered one.")
37
Blood contamination of anesthesia equipment & monitoring equipment
Blood contamination of anesthesia equipment & monitoring equipment. Anesth Analg Jun;78(6): Hall JR. - See full abstracts 19 definable surfaces were sampled in 22 operating rooms. 33% of surfaces were contaminated with blood. Contaminated equipment included surfaces that are in continuous contact with patients, e.g., blood pressure cuffs and pulse oximeter probes. Visual inspection was not a reliable means of detecting blood contamination.
: Hall JR. - See full abstracts. 19 definable surfaces were sampled in 22 operating rooms. 33% of surfaces were contaminated with blood. Contaminated equipment included surfaces that are in continuous contact with patients, e.g., blood pressure cuffs and pulse oximeter probes. Visual inspection was not a reliable means of detecting blood contamination.")
38
Transmission of pathogenic bacterial organisms in the anesthesia work area. Loftus RW, Koff MD, Burchman CC, Schwartzman JD, Thorum V, Read ME, Wood TA, Beach ML. Anesthesiology Sep;109(3): See Reference section for full abstract RESULTS: Bacterial contamination of the anesthesia work area increased significantly at the case conclusion, with a mean difference of 115 colonies per surface area sampled (95% CI: ; P < 0.001). Transmission of bacterial organisms, including VRE to IV stopcock sets occurred in 32% (95% CI, %) of cases. CONCLUSION: Potentially pathogenic, multidrug-resistant bacterial organisms are transmitted during the practice of general anesthesia to both the anesthesia work area and intravenous stopcock sets.
. Transmission of bacterial organisms, including VRE to IV stopcock sets occurred in 32% (95% CI, %) of cases. CONCLUSION: Potentially pathogenic, multidrug-resistant bacterial organisms are transmitted during the practice of general anesthesia to both the anesthesia work area and intravenous stopcock sets.")
39
Microbial growth on the anesthesia machine
Microbial growth on the anesthesia machine. Maslyk PA, Nafziger DA, Burns SM, Bowers PR. AANA J Feb;70(1):53-6. Purpose: Determine amount of microbial growth that develops on the anesthesia machine after a full day's use in OR. Descriptive bacteriology study relevant to anesthesia practice given proximity of the oropharynx & multiple body fluids to anesthesia equipment & potential for cross-contamination to patients & staff. P value of 0.12 indicated that the observed CFU increase was not statistically significant at the .05 level. Organisms found on anesthesia machine tabletop: coagulase- negative Staphylococcus, Bacillus, alpha Streptococcus, Acinetobacter, Staphylococcus aureus, and gram-negative rods. Several were expected to be found; however, alpha Streptococcus, Acinetobacter, S aureus, & gram-negative rods are pathogenic organisms causing respiratory infections & bacteremia, especially in patients with compromised conditions.
:53-6. Purpose: Determine amount of microbial growth that develops on the anesthesia machine after a full day s use in OR. Descriptive bacteriology study relevant to anesthesia practice given proximity of the oropharynx & multiple body fluids to anesthesia equipment & potential for cross-contamination to patients & staff. P value of 0.12 indicated that the observed CFU increase was not statistically significant at the .05 level. Organisms found on anesthesia machine tabletop: coagulase- negative Staphylococcus, Bacillus, alpha Streptococcus, Acinetobacter, Staphylococcus aureus, and gram-negative rods. Several were expected to be found; however, alpha Streptococcus, Acinetobacter, S aureus, & gram-negative rods are pathogenic organisms causing respiratory infections & bacteremia, especially in patients with compromised conditions.")
40
Microbial colonization of tourniquets used in orthopedic surgery
Microbial colonization of tourniquets used in orthopedic surgery. Orthopedics Aug;29(8): Walsh EF, Ben-David D, Ritter M, Mechrefe A, Mermel LA, DiGiovanni C. See full abstract in references Study analyzed tourniquets used for orthopedic surgery Group A tourniquets main OR Group B tourniquets ambulatory surgicenter, Group C tourniquets unused, prepackaged, sterile tourniquets from main OR & Group D tourniquets were sterilely packed tourniquets from ambulatory surgicenter. Tourniquets from Groups A, B, C, and D had 100%, 40%, 0%, and 0% microbial growth, respectively. Group A tourniquets, coagulase-negative staphylococci, Bacillus & Staphylococcus aureus were present in 100%, 60%, and 20% of tourniquets, respectively. 20% contaminated either with Streptococcus sanguis, Aerococcus viridans, or Cornyebacterium species. Coagulase-negative staphylococci & Bacillus were present in 40% and 30% of Group B tourniquets, respectively. Tourniquet contamination may be a risk factor for the development of SSI in orthopedic surgery.
: Walsh EF, Ben-David D, Ritter M, Mechrefe A, Mermel LA, DiGiovanni C. See full abstract in references. Study analyzed tourniquets used for orthopedic surgery. Group A tourniquets main OR. Group B tourniquets ambulatory surgicenter, Group C tourniquets unused, prepackaged, sterile tourniquets from main OR & Group D tourniquets were sterilely packed tourniquets from ambulatory surgicenter. Tourniquets from Groups A, B, C, and D had 100%, 40%, 0%, and 0% microbial growth, respectively. Group A tourniquets, coagulase-negative staphylococci, Bacillus & Staphylococcus aureus were present in 100%, 60%, and 20% of tourniquets, respectively. 20% contaminated either with Streptococcus sanguis, Aerococcus viridans, or Cornyebacterium species. Coagulase-negative staphylococci & Bacillus were present in 40% and 30% of Group B tourniquets, respectively. Tourniquet contamination may be a risk factor for the development of SSI in orthopedic surgery.")
41
Ultraviolet lighting during orthopaedic surgery and the rate of infection. J Bone Joint Surg Am Sep;89(9): Ritter MA, Olberding EM, Malinzak RA. See full abstract in references BACKGROUND:. The purpose of the present study was to compare the infection rates following joint replacement procedures performed by 1 orthopaedic surgeon with & without the use of ultraviolet lighting. METHODS: July 1986 to July 2005, 1 surgeon performed 5980 total joint replacements at 1 facility. In September 1991, ultraviolet lighting was installed in the operating rooms. RESULTS: The odds of infection were 3.1 times greater for procedures performed without ultraviolet lighting (& with laminar airflow) as compared with those performed with only ultraviolet lighting (p < ). The infection rate associated with total hip replacement decreased from 1.03% to 0.72% (p = ), and the infection rate associated with total knee replacement decreased from 2.20% to 0.50% (p < ).
 as compared with those performed with only ultraviolet lighting (p < ). The infection rate associated with total hip replacement decreased from 1.03% to 0.72% (p = ), and the infection rate associated with total knee replacement decreased from 2.20% to 0.50% (p < ).")
42
Surgical area contamination--comparable bacterial counts using disposable head and mask and helmet aspirator system, but dramatic increase upon omission of head-gear: an experimental study in horizontal laminar air-flow. Friberg B, Friberg S, Ostensson R, Burman LG. J Hosp Infect Feb;47(2):110-5. Effect of different head coverings on air-borne transmission of bacteria & particles in the surgical area - studied during 30 strictly standardized sham operations performed in a horizontal laminar air flow (LAF) unit. The OR team wore disposable gowns plus either a 1) non-sterile head covering consisting of a squire type disposable hood & triple laminar face mask, 2) a sterilized helmet aspirator system or 3) no head cover at all. In the wound area both types of head cover resulted in low and comparable air (means of 8 and 4cfu/m(3)) and surface contamination (means of 69 and 126cfu/m(2)/h) rates. Omission of head-gear resulted in a three- to five-fold increase (P > or = ), depending on site sampled air contamination rate (mean of 22cfu/m(3)) whereas the bacterial sedimentation rate in the wound area increased about 60-fold ( P > or = ). A proper head cover minimized the emission of apparently heavy particles that were not removed by the horizontal LAF & contained mainly streptococci, presumably of respiratory tract origin. Dust particle counts revealed no differences between the three experimental situations. No correlation between air and surface contamination rates or between air contamination and air particle counts was found From a bacteriological point of view, disposable hoods of squire type and face masks are equally as efficient as a helmet aspirator system & both will efficiently contain the substantial emission of bacteria-carrying droplets from the respiratory tract occurring when head cover is omitted. Finally, the use of bacterial air counts to assess surgical site surface contamination in horizontal LAF units must be seriously questioned.
 unit. The OR team wore disposable gowns plus either a 1) non-sterile head covering consisting of a squire type disposable hood & triple laminar face mask, 2) a sterilized helmet aspirator system or 3) no head cover at all. In the wound area both types of head cover resulted in low and comparable air (means of 8 and 4cfu/m(3)) and surface contamination (means of 69 and 126cfu/m(2)/h) rates. Omission of head-gear resulted in a three- to five-fold increase (P > or = ), depending on site sampled air contamination rate (mean of 22cfu/m(3)) whereas the bacterial sedimentation rate in the wound area increased about 60-fold ( P > or = ). A proper head cover minimized the emission of apparently heavy particles that were not removed by the horizontal LAF & contained mainly streptococci, presumably of respiratory tract origin. Dust particle counts revealed no differences between the three experimental situations. No correlation between air and surface contamination rates or between air contamination and air particle counts was found. From a bacteriological point of view, disposable hoods of squire type and face masks are equally as efficient as a helmet aspirator system & both will efficiently contain the substantial emission of bacteria-carrying droplets from the respiratory tract occurring when head cover is omitted. Finally, the use of bacterial air counts to assess surgical site surface contamination in horizontal LAF units must be seriously questioned.")
46
Hyperglycemia & SSI What is the evidence?

52
Is it time for a “SSI Prevention Bundle for Orthopedic Surgery?”
Are we using the evidence we have? “Excellence is a moving target”

53
Review of a bundle used to reduce Orthopedic SSI & evidence supporting potential for positive impact on outcomes Bundle: Preoperative: 2% CHG Sage® Cloths 3MTM Skin & Nasal Antiseptic Warming with 3MTM Bair Paws Huddle - checklist

54
Preventing Orthopedic Total Joint Replacement Surgical Site Infections through a Comprehensive Best Practice Bundle/Checklist Authors: Jette R. Hogenmiller, PhD, MN, APRN, CDE, James Hamilton, MD, Todd Clayman, RN, BSN, BernaSue Casper, MBA, Kathy Sparks, RN, BSN, Akin Cil, MD, James Stanford, MD, Sarah Darby, RN, BSN, MBA, Cheryl Pilsl, RN, DN, CRNA, Kara Settles, MD, Judy Kratz, RN, Steve DeGarmo, BS, Steve Williams, BA, Tendai Zinyemba, EVS; Hospital: Truman Medical Center, Kansas City,, MO

55
Orthopedic Total Joint Surgery Checklist
TOPIC ACTION ACTION STATUS* COMMENTS Yes No Date Time Clinic Medical Has medical clearance been obtained? Dental Has dental clearance been obtained? Education Preoperative education provided 2% CHG Preoperative shower CHG pack & instructions given PAT PAT Visit 7-10 day prior to surgery Laboratory Complete laboratory tests, assure results support surgery OK Preoperative Call Reinforce & importance of preop 2% CHG showers Remind patient to be NPO after midnight, NO gum or mints, Meds with a sip of water. Ask about recent illness Surgery Day - Preoperative Area Terminal Clean Verify OR room terminally cleaned prior to Ortho implant surgery Labs drawn by 7AM & verify standards met to proceed with surgery Verify showers completed (#1soap/H20; #2 PM; #3pre-op area); Y=all done Circle which done Nares Apply 3M product to nares, if pt not allergic to iodine. Use protocol. Warming Warming 30 min in advance of surgery; time Bear Paws applied Dose of Antibx Verify dosing based on current protocol Antibiotic Antibiotic infusion begun for 8 AM surgery infused by time of incision done 10 min. before incision Ancef done 10 min before incision Instruments Coordinate time start for table/instrument prep - doc open time Team Team huddle - SCOAP/WHO Intraoperative Incision Surgery incision time Temp Patient temperature maintained at 36.0 Orthopedic Total Joint Surgery Checklist PATIENT STICKER (NOT for explants or spacer revision) Surgery Date: ____/____/______ *Place initials of the individual verifying completion of the action in the appropriate "yes" or "no" location, and place the date and time the action occurred, where appropriate, in respective locations & include AM or PM.
; Y=all done. Circle which done. Nares. Apply 3M product to nares, if pt not allergic to iodine. Use protocol. Warming. Warming 30 min in advance of surgery; time Bear Paws applied. Dose of Antibx. Verify dosing based on current protocol. Antibiotic. Antibiotic infusion begun for 8 AM surgery. - infused by time of incision. - done 10 min. before incision. Ancef - done 10 min before incision. Instruments. Coordinate time start for table/instrument prep - doc open time. Team. Team huddle - SCOAP/WHO. Intraoperative. Incision. Surgery incision time. Temp. Patient temperature maintained at Orthopedic Total Joint Surgery Checklist. PATIENT STICKER. (NOT for explants or spacer revision) Surgery Date: ____/____/______. *Place initials of the individual verifying completion of the action in the appropriate yes or no location, and place the date and time the action occurred, where appropriate, in respective locations & include AM or PM.")
56
Preoperative Skin Preparation

57
Preoperative shower revisited: Can high topical antiseptic levels be achieved on the skin surface before surgical admission? Edmiston CE Jr, Krepel CJ, Seabrook GR, Lewis BD, Brown KR, Towne JB. J Am Coll Surg. 2008 Aug; 207(2): Epub 2008 May 23. BACKGROUND: Chlorhexidine gluconate (CHG) skin concentrations were determined after preoperative showering/skin cleansing using 4% CHG soap or 2% CHG-impregnated polyester cloth. STUDY DESIGN: Subjects were randomized to 1 of 3 shower (4% soap)/skin cleansing (2% cloth) groups (n = 20 per group): Group 1 A/B evening, Group 2 A/B morning, or Group 3 A/B evening & morning. After showering or skin cleansing, volunteers returned to the investigator's laboratory where CHG skin surface concentrations were determined at five separate skin sites. CHG concentrations were compared with CHG minimal inhibitory concentration that inhibits 90% (MIC(90)) of staphylococcal skin isolates. RESULTS:CHG MIC(90) for 61 skin isolates was 4.8 parts per million (ppm). Evening only 17.2 – 31.6 ppm Group 1A, 4% CHG skin concentrations & 361.5 to ppm Group 1B, 2% CHG. (p < ) Morning only 51.6 to ppm Group 2A, 4% CHG 848.1 to 1,049.6 ppm in group 2B, 2% CHG (p < ). Evening & morning 101.4 to ppm Group 3A, 4% CHG 1,484.6 to 2,031.3 ppm Group 3B 2% CHG cloth (p < ). Effective CHG levels were not detected in the 4% CHG group in selected sites in seven (35%) subjects in group 1A, three (15%) in group 2A, and five (25%) in group 3A.
 skin concentrations were determined after preoperative. showering/skin cleansing using 4% CHG soap or 2% CHG-impregnated polyester cloth. STUDY DESIGN: Subjects were randomized to 1 of 3 shower (4% soap)/skin cleansing (2% cloth) groups (n = 20 per group): Group 1 A/B evening, Group 2 A/B morning, or. Group 3 A/B evening & morning. After showering or skin cleansing, volunteers returned to the investigator s laboratory where CHG skin surface concentrations. were determined at five separate skin sites. CHG concentrations were compared with CHG minimal inhibitory concentration. that inhibits 90% (MIC(90)) of staphylococcal skin isolates. RESULTS:CHG MIC(90) for 61 skin isolates was 4.8 parts per million (ppm). Evening only – 31.6 ppm Group 1A, 4% CHG skin concentrations & to ppm Group 1B, 2% CHG. (p < ) Morning only to ppm Group 2A, 4% CHG to 1,049.6 ppm in group 2B, 2% CHG (p < ). Evening & morning to ppm Group 3A, 4% CHG. 1,484.6 to 2,031.3 ppm Group 3B 2% CHG cloth (p < ). Effective CHG levels were not detected in the 4% CHG group in selected sites in seven (35%) subjects in group 1A, three (15%) in group 2A, and five (25%) in group 3A.")
59
a

60
Page #1 Night before instructions on use of 2% Sage cloths.
Tested in inner-city sample after revised by ambulatory care nurses Clean bed linens & pajamas also required.

61
Page # 2 1 & 2 packages night before 1 package AM of surgery

62
Evidence & interventions used to address these as sources of SSI
NASAL FLORA & SSI Evidence & interventions used to address these as sources of SSI

66
MRSA colonization studies
Population Location Year % Staph %MRSA IHS clinics 1 WA State 2004 27.3 1.9 Hosp admit 2 Atlanta 2003 21.0 2.7 Homeless 3 San Francisco 2002 22.8 2.8 Peds clinic 3 Chicago 2000 22.4 0.6 Adult*/Peds 3 New York 28*/34 0*/0.4 Students 3 Minneapolis 36.2 7.4 Peds ER 3 26.4 2.2 Hosp admit 3 Charlottesville 1999 NA 0.98 Boston 1998 24.8 2.6 Peds clinic4 Nashville 36.4 9.2 Rates of carriage of MRSA in the community so far has been low. 1) Leman R. Infect Control Hosp Epidemiol; ) Jernigan JA. Infect Control Hosp Epidemiol; ) Salgado CD. Clin Infect Dis; ) Creech CB. Peds ID 2005
 Leman R. Infect Control Hosp Epidemiol; ) Jernigan JA. Infect Control Hosp Epidemiol; ) Salgado CD. Clin Infect Dis; ) Creech CB. Peds ID")
67
Consecutive series of patients undergoing orthopaedic surgery for either insertion of metal prostheses or internal fracture fixation. Wilcox MH, Hall J, Pike H, et al: Use of perioperative mupirocin to prevent methicillin-resistant staphylococcus aureus (MRSA) orthopaedic surgical site infections. J Hosp Infect 2003;54: Of the 11 MRSA SSIs that occurred in the mupirocin/triclosan group, only one patient received the intervention correctly. The number of SSIs caused by other pathogens was not affected by the intervention. The relative contributions of mupirocin & triclosan could not be determined. Nevertheless, the authors stated that their results justify empirical, as opposed to targeted, usage of mupirocin prophylaxis because current health care practice makes it almost impossible to preoperatively assess for MRSA carriage and subsequently treat all patients undergoing orthopaedic surgery.[this is an inappropriate conclusion] Treatment: Pts received perioperative prophylaxis with: nasal mupirocin for 5 days & a bath or shower with 2% triclosan the day before surgery. The control group consisted of patients undergoing similar procedures in the 6 months before the mupirocin/triclosan regimen was started. Both groups received intravenous cephradine for 24 hours perioperatively. There was a marked decrease in the incidence of MRSA nasal carriage in the group treated with mupirocin & triclosan. After introduction of the mupirocin/triclosan protocol, MRSA SSIs decreased from 23 per 1,000 to 3.3 to 4 per 1,000

68
Mupirocin data continued
Rotger M, Trampuz A, Piper KE, Steckelberg JM, Patel R. Phenotypic & genotypic mupirocin resistance among staphylococci causing prosthetic joint infection. J Clin Microbiol 2005; 43: It is of concern that Rotger found that 27% of MRSA isolates causing hip or knee prosthetic joint infection were resistant to mupirocin.

69
3M Skin & Nasal Antiseptic
solutions/home/products/?PC_7_RJH9U52308DUB0IIL8TMGN _nid=5612BP15 V7be1ZB8J079ZXgl&WT.mc_id=

76
Pre, Intra & Post-operative Warming
Why is it important? & What method did we chose & Why? CMS Core Measures – postoperative measure

81
SSI & Normothermia N = 200 randomized “normothermia” vs. hypothermia
SSI developed in 6% vs. 19% (p = 0.009) Length of Stay (LOS) 2.6 days for hypothermia group (p = 0.001) Intra-operative normo-thermia can be maintained by blankets, warmed IV fluids NEJM 1996;334:1209
 Length of Stay (LOS) 2.6 days for hypothermia group (p = 0.001) Intra-operative normo-thermia can be maintained by blankets, warmed IV fluids. NEJM 1996;334:1209.")
82
Temperature & Surgical Site Infections
Hypothermia reduces tissue oxygen tension by vasoconstriction Hypothermia reduces leukocyte superoxide production Hypothermia increases bleeding & transfusion requirement Hypothermia increases duration of hospital stay even in uninfected patients Melling. Lancet 2001;358:876 Kurz. NEJM 1996;334:1209 Rabkin. Arch Surg 1987;122:221

84
The Bair Hugger patient warming system in prolonged vascular surgery: An infection risk? Huang JK, Shah EF, Vinodkumar N, Hegarty MA, Greatorex RA. Crit Care Jun;7(3):R13-6. Epub 2003 Mar 4. INTRODUCTION: Use of the Bair Hugger forced-air patient warming system during prolonged abdominal vascular surgery may lead to increased bacterial contamination of the surgical field by mobilization of the patient's skin flora. METHODS: Bacterial content analyzed in air & wound specimens collected during surgery in 16 patients undergoing abdominal vascular prosthetic graft insertion procedure, using the Bair Hugger patient warming system. Bacterial colony counts from the beginning & the end of surgery were compared. RESULTS: No increase in bacterial counts at the study sites, but also that there was a decrease (P < 0.01) in air bacterial content around the patient & in the operating theatre after prolonged use of the patient warmer. No wound or graft infections occurred.
 in air bacterial content around the patient & in the operating theatre after prolonged use of the patient warmer. No wound or graft infections occurred.")
85
Antibiotics & SSI Prevention
Medication Dosing Timing

86
Antibiotics & Orthopedic SSI
Are there opportunities beyond the accepted timing?

87
J Am Acad Orthop Surg 2008; 16:283-293

91
Team Huddle Surgical Checklist
Variety of Surgical Checklist exist: SCOAP WHO Others

93
WHO Surgical Checklist http://www. who

94
Implementing a pre-operative checklist to increase patient safety: a 1-year follow-up of personnel attitudes. Nilsson L, Lindberget O, Gupta A, Vegfors M. Acta Anaesthesiol Scand Feb;54(2): Epub 2009 Aug 31. BACKGROUND: The OR is a complex work environment with a high potential for adverse events. We assessed personnel attitudes to a pre-operative checklist ('time out') immediately before start of the operative procedure. METHODS: 'Time out' was implemented in December 2007 as an additional safety barrier in two Swedish hospitals. One year later, in order to assess how the checklist was perceived, a questionnaire was sent by to 704 persons in the operating departments, including surgeons, anesthesiologists, operation and anesthetic nurses and nurse assistants. RESULTS: The questionnaire was answered by 331 (47%) persons 93% responded that 'time out' contributes to increased patient safety. 83% thought that 'time out' gave an opportunity to identify and solve problems. Confirmation of patient identity, correct procedure, correct side and checking of allergies or contagious diseases were considered 'very important' by 78-84% of the responders. Attitudes to checking of patient positioning, allergies and review of potential critical moments were positive but differed significantly between the professions. Attitudes to a similar checklist at the end of surgery were positive and 72-99% agreed to the different elements. CONCLUSION: Staff attitudes toward a surgical checklist were mostly positive 1 year after their introduction in two large hospitals in central Sweden.
 immediately before start of the operative procedure. METHODS: Time out was implemented in December 2007 as an additional safety barrier in two Swedish hospitals. One year later, in order to assess how the checklist was perceived, a questionnaire was sent by to 704 persons in the operating departments, including surgeons, anesthesiologists, operation and anesthetic nurses and nurse assistants. RESULTS: The questionnaire was answered by 331 (47%) persons. 93% responded that time out contributes to increased patient safety. 83% thought that time out gave an opportunity to identify and solve problems. Confirmation of patient identity, correct procedure, correct side and checking of allergies or contagious diseases were considered very important by 78-84% of the responders. Attitudes to checking of patient positioning, allergies and review of potential critical moments were positive but differed significantly between the professions. Attitudes to a similar checklist at the end of surgery were positive and 72-99% agreed to the different elements. CONCLUSION: Staff attitudes toward a surgical checklist were mostly positive 1 year after their introduction in two large hospitals in central Sweden.")
96
Chuckanut Drive Washington State

97
Next steps, what are they… on our journey to zero for SSI’s?
Ortho SSI Prevention Next steps, what are they… on our journey to zero for SSI’s?

98
References APIC (2010) . Guide to the Elimination of Orthopedic Surgical Site Infections. APIC. Kuper M, Rosenstein A. (2008) Infection prevention in total knee and total hip arthroplasties. Am J Orthop, 37(1):E2–E5. Lee J, Singletary R, Schmader K, Anderson DJ, Bolognesi M, Kaye KS. (2006) Surgical site infection in the elderly following orthopaedic surgery. Risk Factors and Outcomes. J Bone Joint Surg, 88(8):1705–1712. Lentino JR. (2003) Prosthetic joint infections: bane of orthopedists, challenge for infectious disease specialists. Clin Infect Dis, 36:
 Infection prevention in total knee and total hip arthroplasties. Am J Orthop, 37(1):E2–E5. Lee J, Singletary R, Schmader K, Anderson DJ, Bolognesi M, Kaye KS. (2006) Surgical site infection in the elderly following orthopaedic surgery. Risk Factors and Outcomes. J Bone Joint Surg, 88(8):1705–1712. Lentino JR. (2003) Prosthetic joint infections: bane of orthopedists, challenge for infectious disease specialists. Clin Infect Dis, 36:")
99
References - continued
Partanen J, Syrjala H, Vahanikkila H, Jalovaara P. (2006) Impact of deep infection after hip fracture surgery on function and mortality. J Hosp Infect, 62(1): Pollard TC, Newman JE, Barlow NJ, Price JD, Willett KM. (2006) Deep wound infection after proximal femoral fracture: consequences and costs. J Hosp Infect, 63: Rabkin. Arch Surg 1987;122:221 Whitehouse JD, Friedman ND, Kirkland KB, Richardson WJ, Sexton DJ. (2002). The impact of surgical site infections following Orthopedic surgery at a community hospital and a university hospital: Adverse quality of life, excess length of stay, and extra cost. Infect Control Hosp Epidemiol, 23: Wilson J, Charlett A, Leong G, McDougall C, Duckworth G. (2008) Rates of surgical site infection after hip replacement as a hospital performance indicator: Analysis of data from the English mandatory surveillance system. Infect Control Hosp Epidemiol Mar;29(3):
 Impact of deep infection after hip fracture surgery on function and mortality. J Hosp Infect, 62(1): Pollard TC, Newman JE, Barlow NJ, Price JD, Willett KM. (2006) Deep wound infection after proximal femoral fracture: consequences and costs. J Hosp Infect, 63: Rabkin. Arch Surg 1987;122:221. Whitehouse JD, Friedman ND, Kirkland KB, Richardson WJ, Sexton DJ. (2002). The impact of surgical site infections following Orthopedic surgery at a community hospital and a university hospital: Adverse quality of life, excess length of stay, and extra cost. Infect Control Hosp Epidemiol, 23: Wilson J, Charlett A, Leong G, McDougall C, Duckworth G. (2008) Rates of surgical site infection after hip replacement as a hospital performance indicator: Analysis of data from the English mandatory surveillance system. Infect Control Hosp Epidemiol Mar;29(3):")
100
Supplementary Resources
SSI related – additional slides & abstracts for ‘abbreviated’ evidence slides

101
Am J Infect Control. 1998 Apr;26(2):143-5
Am J Infect Control Apr;26(2): Levels of microbial contamination on surgical instruments. Rutala WA, Gergen MF, Jones JF, Weber DJ. Division of Infectious Diseases, University of North Carolina School of Medicine, Chapel Hill, USA. OBJECTIVE: To ascertain the microbial load and type of organisms on used surgical instruments following standard cleaning, which consisted of the use of a washer sterilizer followed by sonic cleaning. DESIGN: In this prospective experimental study, used surgical instruments were immersed in Peptamin Tween broth, the broth agitated, and then filtered through a 0.45 microm filter. Quantitative cultures were performed, and all microbes were identified by using standard techniques. SETTING: This study was conducted at a 660-bed university hospital. RESULTS: The microbial load remaining on used surgical instruments after cleaning was as follows: 36 (72%) instruments 0 to 10 colony-forming units (CFU), 7 (14%) instruments 11 to 100 CFU, and 7 (14%) instruments > 100 CFU. Organisms contaminating the instruments included coagulase-negative staphylococcus (56%) followed by Bacillus (22%) and diphtheroids (14%). No other microbes were isolated from more than 4% of the instruments. CONCLUSION: Most used nonlumen surgical instruments contain less than 100 CFU of relatively nonpathogenic microorganisms after cleaning. This suggests that new low-temperature sterilization technologies are likely to be highly effective in preventing cross-transmission of infection via nonlumen medical instruments.
: Levels of microbial contamination on surgical instruments. Rutala WA, Gergen MF, Jones JF, Weber DJ. Division of Infectious Diseases, University of North Carolina School of Medicine, Chapel Hill, USA. OBJECTIVE: To ascertain the microbial load and type of organisms on used surgical instruments following standard cleaning, which consisted of the use of a washer sterilizer followed by sonic cleaning. DESIGN: In this prospective experimental study, used surgical instruments were immersed in Peptamin Tween broth, the broth agitated, and then filtered through a 0.45 microm filter. Quantitative cultures were performed, and all microbes were identified by using standard techniques. SETTING: This study was conducted at a 660-bed university hospital. RESULTS: The microbial load remaining on used surgical instruments after cleaning was as follows: 36 (72%) instruments 0 to 10 colony-forming units (CFU), 7 (14%) instruments 11 to 100 CFU, and 7 (14%) instruments > 100 CFU. Organisms contaminating the instruments included coagulase-negative staphylococcus (56%) followed by Bacillus (22%) and diphtheroids (14%). No other microbes were isolated from more than 4% of the instruments. CONCLUSION: Most used nonlumen surgical instruments contain less than 100 CFU of relatively nonpathogenic microorganisms after cleaning. This suggests that new low-temperature sterilization technologies are likely to be highly effective in preventing cross-transmission of infection via nonlumen medical instruments.")
102
Transmission of pathogenic bacterial organisms in the anesthesia work area. Loftus RW, Koff MD, Burchman CC, Schwartzman JD, Thorum V, Read ME, Wood TA, Beach ML. Anesthesiology Sep;109(3): Department of Anesthesiology, Dartmouth-Hitchcock Medical Center, Comment in: Anesthesiology May;110(5):1191; author reply BACKGROUND: The current prevalence of hospital-acquired infections and evolving amplification of bacterial resistance are major public health concerns. A heightened awareness of intraoperative transmission of potentially pathogenic bacterial organisms may lead to implementation of effective preventative measures. METHODS: Sixty-one operative suites were randomly selected for analysis. Sterile intravenous stopcock sets and two sites on the anesthesia machine were decontaminated and cultured aseptically at baseline and at case completion. The primary outcome was the presence of a positive culture on the previously sterile patient stopcock set. Secondary outcomes were the number of colonies per surface area sampled on the anesthesia machine, species identification, and antibiotic susceptibility of isolated organisms. R RESULTS: Bacterial contamination of the anesthesia work area increased significantly at the case conclusion, with a mean difference of 115 colonies per surface area sampled (95% confidence interval [CI], ; P < 0.001). Transmission of bacterial organisms, including vancomycin-resistant enterococcus, to intravenous stopcock sets occurred in 32% (95% CI, %) of cases. Highly contaminated work areas increased the odds of stopcock contamination by 4.7 (95% CI, ; P = 0.011). Contaminated intravenous tubing was associated with a trend toward increased nosocomial infection rates (odds ratio, 3.08; 95% CI, ; P = 0.11) and with an increase in mortality (95% CI odds ratio, infinity; P = ). CONCLUSION: Potentially pathogenic, multidrug-resistant bacterial organisms are transmitted during the practice of general anesthesia to both the anesthesia work area and intravenous stopcock sets. Implementation of infection control measures in this area may help to reduce both the evolving problem of increasing bacterial resistance and the development of life-threatening infectious complications. Full abstract for prior slide – for future reference, not reviewed.
. Transmission of bacterial organisms, including vancomycin-resistant enterococcus, to intravenous stopcock sets occurred in 32% (95% CI, %) of cases. Highly contaminated work areas increased the odds of stopcock contamination by 4.7 (95% CI, ; P = 0.011). Contaminated intravenous tubing was associated with a trend toward increased nosocomial infection rates (odds ratio, 3.08; 95% CI, ; P = 0.11) and with an increase in mortality (95% CI odds ratio, infinity; P = ). CONCLUSION: Potentially pathogenic, multidrug-resistant bacterial organisms are transmitted during the practice of general anesthesia to both the anesthesia work area and intravenous stopcock sets. Implementation of infection control measures in this area may help to reduce both the evolving problem of increasing bacterial resistance and the development of life-threatening infectious complications. Full abstract for prior slide – for future reference, not reviewed.")
103
Microbial colonization of tourniquets used in orthopedic surgery
Microbial colonization of tourniquets used in orthopedic surgery. Orthopedics Aug;29(8): Walsh EF, Ben-David D, Ritter M, Mechrefe A, Mermel LA, DiGiovanni C. Department of Orthopedic Surgery Rhode Island Hospital, USA. Comment in: Orthopedics Dec;29(12):1060; author reply This study analyzed tourniquets used for orthopedic surgery in our hospital to Group A tourniquets were from our main operating room, Group B tourniquets were from our ambulatory surgicenter, Group C tourniquets were unused, prepackaged, sterile tourniquets from our main operating room, and Group D tourniquets were sterilely packed tourniquets from our ambulatory surgicenter. Tourniquets from Groups A, B, C, and D had 100%, 40%, 0%, and 0% microbial growth, respectively. For Group A tourniquets, coagulase-negative staphylococci, Bacillus, and Staphylococcus aureus were present in 100%, 60%, and 20% of tourniquets, respectively. Twenty percent were contaminated either with Streptococcus sanguis, Aerococcus viridans, or Cornyebacterium species. Coagulase-negative staphylococci and Bacillus were present in 40% and 30% of Group B tourniquets, respectively. Tourniquet contamination may be a risk factor for the development of surgical site infection in orthopedic surgery.
: Walsh EF, Ben-David D, Ritter M, Mechrefe A, Mermel LA, DiGiovanni C. Department of Orthopedic Surgery Rhode Island Hospital, USA. Comment in: Orthopedics Dec;29(12):1060; author reply This study analyzed tourniquets used for orthopedic surgery in our hospital to. Group A tourniquets were from our main operating room, Group B tourniquets were from our ambulatory surgicenter, Group C tourniquets were unused, prepackaged, sterile tourniquets from our main operating room, and. Group D tourniquets were sterilely packed tourniquets from our ambulatory surgicenter. Tourniquets from Groups A, B, C, and D had 100%, 40%, 0%, and 0% microbial growth, respectively. For Group A tourniquets, coagulase-negative staphylococci, Bacillus, and Staphylococcus aureus were present in 100%, 60%, and 20% of tourniquets, respectively. Twenty percent were contaminated either with Streptococcus sanguis, Aerococcus viridans, or Cornyebacterium species. Coagulase-negative staphylococci and Bacillus were present in 40% and 30% of Group B tourniquets, respectively. Tourniquet contamination may be a risk factor for the development of surgical site infection in orthopedic surgery.")
104
Zhonghua Hu Li Za Zhi. 1996 Dec;31(12):690-1
Zhonghua Hu Li Za Zhi Dec;31(12): [Study of surgical instruments contamination by bacteria from air during the operation] [Article in Chinese] Yin SH, Xu SH, Bo YC. Anhui Provincicial Hospital, Hefei, P.R. China. Routinely sterilized surgical instruments were divided into two groups and put on the same instrument table, one group was covered with dressing and the other was exposed to the air. The samples were collected at 30 min, 60 min, and 90 min respectively after operation began and bacterium culture was done. The results showed that the general air contamination rate of the exposed group was 1.18 times higher than that of the covered one. The exposure time had a positive correlation with bacterium contamination rate. This study gave the laboratory evidence for controlling the infection in the operation room. Full abstract for prior slide – for future reference, not reviewed.
: [Study of surgical instruments contamination by bacteria from air during the operation] [Article in Chinese] Yin SH, Xu SH, Bo YC. Anhui Provincicial Hospital, Hefei, P.R. China. Routinely sterilized surgical instruments were divided into two groups and put on the same instrument table, one group was covered with dressing and the other was exposed to the air. The samples were collected at 30 min, 60 min, and 90 min respectively after operation began and bacterium culture was done. The results showed that the general air contamination rate of the exposed group was 1.18 times higher than that of the covered one. The exposure time had a positive correlation with bacterium contamination rate. This study gave the laboratory evidence for controlling the infection in the operation room. Full abstract for prior slide – for future reference, not reviewed.")
105
Environmental and body contamination through aerosols produced by high-speed cutters in lumbar spine surgery. Nogler M, Lass-Flörl C, Ogon M, Mayr E, Bach C, Wimmer C. Spine (Phila Pa 1976) Oct 1;26(19): Department of Orthopaedic Surgery, University of Innsbruck, Austria. STUDY DESIGN: A cadaver study to evaluate contamination in the operating room through the use of a high-speed bone cutter. OBJECTIVES: To determine the grade of contamination of animate and inanimate objects through an aerosol intraoperatively, produced by a high-speed cutter during lumbar laminectomy. SUMMARY OF BACKGROUND: In spinal surgery, high-speed cutters are used that produce an aerosol consisting of a mixture of irrigation solution, blood, and tissue debris. Such aerosols can be contaminated with potential pathogens. The surgical personnel and the environment are therefore exposed to a contamination risk. METHODS: Laminectomies at three points (L2-L4) were performed on a human cadaver using a high-speed cutting device. The aerosol produced by the irrigation solution was contaminated with Staphylococcus aureus ATCC To detect the contamination of the environment and of the surgical team, surveillance cultures were used. RESULTS: By air sampling, staphylococci were detected in the operating room at an extension of 5 by 7 m. The surgical team showed extensive face and body contamination with S. aureus. Despite protection by a barrier drape, similar contamination was observed on both the cadaver's head and the anesthesiologist. CONCLUSIONS: The use of high-speed cutters in spinal surgery produces an aerosol that can be contaminated with blood-borne pathogens from infected patients. This aerosol is spread over the whole surgical room and contaminates the room and all personnel present. It is therefore critical to ensure that effective infection control measures are performed, not only by the surgeons but by everyone present in the operating room. The room itself must be sufficiently disinfected after such procedures.
 were performed on a human cadaver using a high-speed cutting device. The aerosol produced by the irrigation solution was contaminated with Staphylococcus aureus ATCC To detect the contamination of the environment and of the surgical team, surveillance cultures were used. RESULTS: By air sampling, staphylococci were detected in the operating room at an extension of 5 by 7 m. The surgical team showed extensive face and body contamination with S. aureus. Despite protection by a barrier drape, similar contamination was observed on both the cadaver s head and the anesthesiologist. CONCLUSIONS: The use of high-speed cutters in spinal surgery produces an aerosol that can be contaminated with blood-borne pathogens from infected patients. This aerosol is spread over the whole surgical room and contaminates the room and all personnel present. It is therefore critical to ensure that effective infection control measures are performed, not only by the surgeons but by everyone present in the operating room. The room itself must be sufficiently disinfected after such procedures.")
106
Microbial growth on the anesthesia machine
Microbial growth on the anesthesia machine. Maslyk PA, Nafziger DA, Burns SM, Bowers PR. AANA J Feb;70(1):53-6. Genesys Regional Medial Center, Grand Blanc, Mich., USA. The purpose of this study was to determine the amount of microbial growth that develops on the anesthesia machine after a full day's use in the operating room. This descriptive bacteriology study is relevant to anesthesia practice because of the proximity of the oropharynx and multiple body fluids to anesthesia equipment and the potential for cross- contamination to patients and staff. The Wilcoxon signed rank test was used to evaluate the change in colony-forming units (CFUs) before and after use of equipment. The resulting P value of 0.12 indicated that the observed CFU increase was not statistically significant at the .05 level. The study identified many organisms that survive on the anesthesia machine tabletop, namely, coagulase-negative Staphylococcus, Bacillus, alpha Streptococcus, Acinetobacter, Staphylococcus aureus, and gram-negative rods. Several were expected to be found; however, alpha Streptococcus, Acinetobacter, S aureus, and gram-negative rods are pathogenic organisms causing respiratory infections and bacteremia, especially in patients with compromised conditions. Terminal cleaning methods may have changed during the course of the study, thereby contributing to the volume of microbes present before use and distorting the change in the number of CFUs before and after use.
:53-6. Genesys Regional Medial Center, Grand Blanc, Mich., USA. The purpose of this study was to determine the amount of microbial growth that develops on the anesthesia machine after a full day s use in the operating room. This descriptive bacteriology study is relevant to anesthesia practice because of the proximity of the oropharynx and multiple body fluids to anesthesia equipment and the potential for cross- contamination to patients and staff. The Wilcoxon signed rank test was used to evaluate the change in colony-forming units (CFUs) before and after use of equipment. The resulting P value of 0.12 indicated that the observed CFU increase was not statistically significant at the .05 level. The study identified many organisms that survive on the anesthesia machine tabletop, namely, coagulase-negative Staphylococcus, Bacillus, alpha Streptococcus, Acinetobacter, Staphylococcus aureus, and gram-negative rods. Several were expected to be found; however, alpha Streptococcus, Acinetobacter, S aureus, and gram-negative rods are pathogenic organisms causing respiratory infections and bacteremia, especially in patients with compromised conditions. Terminal cleaning methods may have changed during the course of the study, thereby contributing to the volume of microbes present before use and distorting the change in the number of CFUs before and after use.")
107
Anesth Analg Jun;78(6): Blood contamination of anesthesia equipment and monitoring equipment. Hall JR. Department of Anesthesiology, Emory University School of Medicine, Atlanta, Georgia. This study was conducted to determine the extent of blood contamination of anesthesia equipment and monitoring equipment in clinical use in operating rooms. The study employed a catalytic-test method, which is used in forensic medicine, to detect blood contamination of anesthesia equipment and monitoring equipment. Nineteen definable surfaces were sampled in 22 operating rooms. Thirty-three percent of surfaces were contaminated with blood. Contaminated equipment included surfaces that are in continuous contact with patients, e.g., blood pressure cuffs and pulse oximeter probes. Visual inspection was not a reliable means of detecting blood contamination. Whether this blood contamination represents an infection risk was not determined. Nevertheless, improved cleaning and disinfection procedures are probably needed. Equipment design needs to focus on reducing the potential for blood contamination and enhancing capability for cleaning and disinfection.

108
Surgical area contamination--comparable bacterial counts using disposable head and mask and helmet aspirator system, but dramatic increase upon omission of head-gear: an experimental study in horizontal laminar air-flow. Friberg B, Friberg S, Ostensson R, Burman LG. J Hosp Infect Feb;47(2): Department of Nursing, Umeå University, Umeå, SE-90187, Sweden. The effect of different head coverings on air-borne transmission of bacteria and particles in the surgical area was studied during 30 strictly standardized sham operations performed in a horizontal laminar air flow (LAF) unit. The operating team members wore disposable gowns plus either a non- sterile head covering consisting of a squire type disposable hood and triple laminar face mask, a sterilized helmet aspirator system or no head cover at all. In the wound area both types of head cover resulted in low and comparable air (means of 8 and 4cfu/m(3)) and surface contamination (means of 69 and 126cfu/m(2)/h) rates. Omission of head-gear resulted in a three- to five-fold increase (P > or = ), depending on site sampled air contamination rate (mean of 22cfu/m(3)) whereas the bacterial sedimentation rate in the wound area increased about 60-fold ( P > or = ). A proper head cover minimized the emission of apparently heavy particles that were not removed by the horizontal LAF and contained mainly streptococci, presumably of respiratory tract origin. Dust particle counts revealed no differences between the three experimental situations. No correlation between air and surface contamination rates or between air contamination and air particle counts was found. We conclude that, from a bacteriological point of view, disposable hoods of squire type and face masks are equally as efficient as a helmet aspirator system and both will efficiently contain the substantial emission of bacteria-carrying droplets from the respiratory tract occurring when head cover is omitted. Finally, the use of bacterial air counts to assess surgical site surface contamination in horizontal LAF units must be seriously questioned. Copyright 2001 The Hospital Infection Society.
 unit. The operating team members wore disposable gowns plus either a non- sterile head covering consisting of a squire type disposable hood and triple laminar face mask, a sterilized helmet aspirator system or no head cover at all. In the wound area both types of head cover resulted in low and comparable air (means of 8 and 4cfu/m(3)) and surface contamination (means of 69 and 126cfu/m(2)/h) rates. Omission of head-gear resulted in a three- to five-fold increase (P > or = ), depending on site sampled air contamination rate (mean of 22cfu/m(3)) whereas the bacterial sedimentation rate in the wound area increased about 60-fold ( P > or = ). A proper head cover minimized the emission of apparently heavy particles that were not removed by the horizontal LAF and contained mainly streptococci, presumably of respiratory tract origin. Dust particle counts revealed no differences between the three experimental situations. No correlation between air and surface contamination rates or between air contamination and air particle counts was found. We conclude that, from a bacteriological point of view, disposable hoods of squire type and face masks are equally as efficient as a helmet aspirator system and both will efficiently contain the substantial emission of bacteria-carrying droplets from the respiratory tract occurring when head cover is omitted. Finally, the use of bacterial air counts to assess surgical site surface contamination in horizontal LAF units must be seriously questioned. Copyright 2001 The Hospital Infection Society.")
109
J Bone Joint Surg Am. 2007 Sep;89(9):1935-40
J Bone Joint Surg Am Sep;89(9): Ultraviolet lighting during orthopaedic surgery and the rate of infection. Ritter MA, Olberding EM, Malinzak RA. The Center for Hip and Knee Surgery, St. Francis Hospital-Mooresville, 1199 Hadley Road, Mooresville, IN 46158, USA. BACKGROUND: Ultraviolet lighting is an alternative to laminar airflow in the operating room that may be as effective for lowering the number of environmental bacteria and possibly lowering infection rates by killing the bacteria rather than simply reducing the number at the operative site. The purpose of the present study was to compare the infection rates following joint replacement procedures performed by one orthopaedic surgeon with and without the use of ultraviolet lighting. METHODS: From July 1986 to July 2005, one surgeon performed 5980 total joint replacements at one facility. In September 1991, ultraviolet lighting was installed in the operating rooms. All procedures that were performed before the installation of the ultraviolet lighting utilized horizontal laminar airflow, whereas all procedures that were performed after that date utilized ultraviolet lighting without laminar airflow. Factors associated with the rate of infection were analyzed. RESULTS: Over a nineteen-year period, forty-seven infections occurred following 5980 joint replacements. The infection rate without ultraviolet lighting (and with laminar airflow) was 1.77%, and the infection rate with ultraviolet lighting was 0.57% (p < ). The odds of infection were 3.1 times greater for procedures performed without ultraviolet lighting (and with laminar airflow) as compared with those performed with only ultraviolet lighting (p < ). The infection rate associated with total hip replacement decreased from 1.03% to 0.72% (p = ), and the infection rate associated with total knee replacement decreased from 2.20% to 0.50% (p < ). Revision surgery, previous infection, age, total body mass index, use of cement, disease, and diagnosis were not associated with an elevated infection rate. CONCLUSION: When appropriate safety precautions are taken, ultraviolet lighting appears to be an effective way to lower the risk of infection in the operating room during total joint replacement surgery.
: Ultraviolet lighting during orthopaedic surgery and the rate of infection. Ritter MA, Olberding EM, Malinzak RA. The Center for Hip and Knee Surgery, St. Francis Hospital-Mooresville, 1199 Hadley Road, Mooresville, IN 46158, USA. BACKGROUND: Ultraviolet lighting is an alternative to laminar airflow in the operating room that may be as effective for lowering the number of environmental bacteria and possibly lowering infection rates by killing the bacteria rather than simply reducing the number at the operative site. The purpose of the present study was to compare the infection rates following joint replacement procedures performed by one orthopaedic surgeon with and without the use of ultraviolet lighting. METHODS: From July 1986 to July 2005, one surgeon performed 5980 total joint replacements at one facility. In September 1991, ultraviolet lighting was installed in the operating rooms. All procedures that were performed before the installation of the ultraviolet lighting utilized horizontal laminar airflow, whereas all procedures that were performed after that date utilized ultraviolet lighting without laminar airflow. Factors associated with the rate of infection were analyzed. RESULTS: Over a nineteen-year period, forty-seven infections occurred following 5980 joint replacements. The infection rate without ultraviolet lighting (and with laminar airflow) was 1.77%, and the infection rate with ultraviolet lighting was 0.57% (p < ). The odds of infection were 3.1 times greater for procedures performed without ultraviolet lighting (and with laminar airflow) as compared with those performed with only ultraviolet lighting (p < ). The infection rate associated with total hip replacement decreased from 1.03% to 0.72% (p = ), and the infection rate associated with total knee replacement decreased from 2.20% to 0.50% (p < ). Revision surgery, previous infection, age, total body mass index, use of cement, disease, and diagnosis were not associated with an elevated infection rate. CONCLUSION: When appropriate safety precautions are taken, ultraviolet lighting appears to be an effective way to lower the risk of infection in the operating room during total joint replacement surgery.")
110
The Bair Hugger patient warming system in prolonged vascular surgery: An infection risk? Huang JK, Shah EF, Vinodkumar N, Hegarty MA, Greatorex RA. Crit Care Jun;7(3):R13-6. Epub 2003 Mar 4. Department of Surgery, Queen Elizabeth Hospital, King's Lynn, UK. INTRODUCTION: Use of the Bair Hugger forced-air patient warming system during prolonged abdominal vascular surgery may lead to increased bacterial contamination of the surgical field by mobilization of the patient's skin flora. METHODS: This possibility was studied by analyzing bacterial content in air and wound specimens collected during surgery in 16 patients undergoing abdominal vascular prosthetic graft insertion procedure, using the Bair Hugger patient warming system. The bacterial colony counts from the beginning and the end of surgery were compared, and the data analyzed using the Wilcoxon matched pairs test. RESULTS: The results showed not only that there was no increase in bacterial counts at the study sites, but also that there was a decrease (P < 0.01) in air bacterial content around the patient and in the operating theatre after prolonged use of the patient warmer. No wound or graft infections occurred. CONCLUSION: The use of this warming system does not lead to increased bacterial contamination of the operating theatre atmosphere, and it is unlikely to affect the surgical field adversely.
 in air bacterial content around the patient and in the operating theatre after prolonged use of the patient warmer. No wound or graft infections occurred. CONCLUSION: The use of this warming system does not lead to increased bacterial contamination of the operating theatre atmosphere, and it is unlikely to affect the surgical field adversely.")
111
Sterilization wrap inspections do not adequately evaluate instrument sterility. Clin Orthop Relat Res Sep;462: Waked WR, Simpson AK, Miller CP, Magit DP, Grauer JN. Department of Orthopaedics and Rehabilitation, Yale University School of Medicine, New Haven, CT , USA. Orthopaedic procedures rely on strict sterilization techniques to prevent surgical site infections. Surgical instrument trays are wrapped for sterilization, and these wraps routinely are inspected by operating room personnel to evaluate for breaches before using the contained instruments. The sensitivity of this practice for detecting wrap defects has not been established. We divided 90 sterilization wraps into groups with no defect and with six sizes of defects ranging from 1.1 to 10.0 mm in diameter. Puncture- type defects were created using nails of known diameter. All wraps were evaluated by medical personnel for evidence of a breach. Detection rates ranged from 6.7% to 96.7% from the smallest to largest defects, respectively. The potential for bacterial transmission through wrap defects also was evaluated, and contaminated nails of the smallest size transmitted bacterial contaminants through the wrap during the creation of puncture defects. Thus, substantial perforations in sterilization wraps frequently are missed when evaluated with commonly used techniques. Defects with a diameter approximately that of a pencil (6.7 mm) were missed 18% of the time, although contamination can be transmitted by a nail with the diameter of a pin (1.1 mm). These results raise questions about a common screening method.
 were missed 18% of the time, although contamination can be transmitted by a nail with the diameter of a pin (1.1 mm). These results raise questions about a common screening method.")
112
Preoperative shower revisited: can high topical antiseptic levels be achieved on the skin surface before surgical admission? Edmiston CE Jr, Krepel CJ, Seabrook GR, Lewis BD, Brown KR, Towne JB. J Am Coll Surg. 2008 Aug; 207(2): Epub 2008 May 23. Source: Division of Vascular Surgery, Medical College of Wisconsin, Milwaukee, WI 53226, BACKGROUND: Skin asepsis is a sentinel strategy for reducing risk of surgical site infections. In this study, chlorhexidine gluconate (CHG) skin concentrations were determined after preoperative showering/skin cleansing using 4% CHG soap or 2% CHG-impregnated polyester cloth. STUDY DESIGN: Subjects were randomized to one of three shower (4% soap)/skin cleansing (2% cloth) groups (n = 20 per group): Group 1 A/B evening, Group 2 A/B morning, or Group 3 A/B evening and morning. After showering or skin cleansing, volunteers returned to the investigator's laboratory where CHG skin surface concentrations were determined at five separate skin sites. CHG concentrations were compared with CHG minimal inhibitory concentration that inhibits 90% (MIC(90)) of staphylococcal skin isolates. RESULTS:CHG MIC(90) for 61 skin isolates was 4.8 parts per million (ppm). Group 1A, 4% CHG skin oncentrations ranged from 17.2 to 31.6 ppm, and CHG concentrations were to ppm (p < ) in Group 1B (2%). In group 2A (4%), CHG levels ranged from 51.6 to ppm and to 1,049.6 ppm in group 2B (2%), respectively (p < ). CHG levels ranged from to ppm in the 4% CHG group (group 3A) compared with 1,484.6 to 2,031.3 ppm in 2% CHG cloth (group 3B) group (p < ). Effective CHG levels were not detected in the 4% CHG group in selected sites in seven (35%) subjects in group 1A, three (15%) in group 2A, and five (25%) in group 3A. CONCLUSIONS: Effective CHG levels were achieved on most skin sites after using 4% CHG; gaps in antiseptic coverage were noted at selective sites even after repeated application. Use of the 2% CHG polyester cloth resulted in considerably higher skin concentrations with no gaps in antiseptic coverage. Effective decolonization of the skin before hospital admission can play an important role in reducing risk of surgical site infections.
 skin concentrations were determined after preoperative showering/skin cleansing using 4% CHG soap or 2% CHG-impregnated polyester cloth. STUDY DESIGN: Subjects were randomized to one of three shower (4% soap)/skin cleansing (2% cloth) groups (n = 20 per group): Group 1 A/B evening, Group 2 A/B morning, or. Group 3 A/B evening and morning. After showering or skin cleansing, volunteers returned to the investigator s laboratory where CHG skin surface concentrations. were determined at five separate skin sites. CHG concentrations were compared with CHG minimal inhibitory concentration. that inhibits 90% (MIC(90)) of staphylococcal skin isolates. RESULTS:CHG MIC(90) for 61 skin isolates was 4.8 parts per million (ppm). Group 1A, 4% CHG skin oncentrations ranged from 17.2 to 31.6 ppm, and CHG concentrations were to ppm (p < ) in. Group 1B (2%). In group 2A (4%), CHG levels ranged from 51.6 to ppm and to 1,049.6 ppm in group 2B (2%), respectively (p < ). CHG levels ranged from to ppm in the 4% CHG group (group 3A) compared with 1,484.6 to 2,031.3 ppm in 2% CHG cloth (group 3B) group (p < ). Effective CHG levels were not detected in the 4% CHG group in selected sites in seven (35%) subjects in group 1A, three (15%) in group 2A, and five (25%) in group 3A. CONCLUSIONS: Effective CHG levels were achieved on most skin sites after using 4% CHG; gaps in antiseptic coverage were noted at selective sites even after repeated application. Use of the 2% CHG polyester cloth resulted in considerably higher skin concentrations with no gaps in antiseptic coverage. Effective decolonization of the skin before hospital admission can play an important role in reducing risk of surgical site infections.")
113
J Bone Joint Surg Br Jan;78(1):92-4 Air contamination during skin preparation and draping in joint replacement surgery. Brown AR, Taylor GJ, Gregg PJ. Glenfield Hospital, Leicester, England. Despite the use of ultraclean air, there are still cases of infection in total joint arthroplasty. One possible route by which bacteria may enter the wound is indirectly by contamination of instruments during skin preparation and draping. We found that bacterial air counts were 4.4 times higher during preparation and draping for hip or knee arthroplasty using an unscrubbed, ungowned leg holder than during the operation itself. With the leg holder scrubbed and gowned during preparation and draping, the air counts were reduced but were still 2.4 fold greater than intraoperatively. On some occasions, the air counts during preparation and draping exceeded the standards for ultraclean air irrespective of the attire of the leg holder. We recommend that the leg is held by a scrubbed and gowned member of the team. More importantly, we consider that instrument packs should be opened only after skin preparation and draping have been completed.

114
Ann R Coll Surg Engl. 2007 Sep;89(6):605-8
Ann R Coll Surg Engl Sep;89(6): Theatre shoes - a link in the common pathway of postoperative wound infection? Amirfeyz R, Tasker A, Ali S, Bowker K, Blom A. Department of Trauma and Orthopaedics, Musgrove Park Hospital, Taunton, UK. INTRODUCTION: Operating department staff are usually required to wear dedicated theatre shoes whilst in the theatre area but there is little evidence to support the beneficial use of theatre shoes. PATIENTS & METHODS: We performed a study to assess the level of bacterial contamination of theatre shoes at the beginning and end of a working day, and compared the results with outdoor footwear. RESULTS: We found the presence of pathogenic bacterial species responsible for postoperative wound infection on all shoe groups, with outdoor shoes being the most heavily contaminated. Samples taken from theatre shoes at the end of duty were less contaminated than those taken at the beginning of the day with the greatest reduction being in the number of coagulase-negative staphylococcal species grown. Studies have demonstrated that floor bacteria may contribute up to 15% of airborne bacterial colony forming units in operating rooms. The pathogenic bacteria we isolated have also been demonstrated as contaminants in water droplets spilt onto sterile gloves after surgical scrubbing. CONCLUSIONS: Theatre shoes and floors present a potential source for postoperative infection. A combination of dedicated theatre shoe use and a good floor washing protocol controls the level of shoe contamination by coagulase-negative staphylococci in particular. This finding is significant given the importance of staphylococcal species in postoperative wound infection.
: Theatre shoes - a link in the common pathway of postoperative wound infection Amirfeyz R, Tasker A, Ali S, Bowker K, Blom A. Department of Trauma and Orthopaedics, Musgrove Park Hospital, Taunton, UK. INTRODUCTION: Operating department staff are usually required to wear dedicated theatre shoes whilst in the theatre area but there is little evidence to support the beneficial use of theatre shoes. PATIENTS & METHODS: We performed a study to assess the level of bacterial contamination of theatre shoes at the beginning and end of a working day, and compared the results with outdoor footwear. RESULTS: We found the presence of pathogenic bacterial species responsible for postoperative wound infection on all shoe groups, with outdoor shoes being the most heavily contaminated. Samples taken from theatre shoes at the end of duty were less contaminated than those taken at the beginning of the day with the greatest reduction being in the number of coagulase-negative staphylococcal species grown. Studies have demonstrated that floor bacteria may contribute up to 15% of airborne bacterial colony forming units in operating rooms. The pathogenic bacteria we isolated have also been demonstrated as contaminants in water droplets spilt onto sterile gloves after surgical scrubbing. CONCLUSIONS: Theatre shoes and floors present a potential source for postoperative infection. A combination of dedicated theatre shoe use and a good floor washing protocol controls the level of shoe contamination by coagulase-negative staphylococci in particular. This finding is significant given the importance of staphylococcal species in postoperative wound infection.")
115
Implementing a pre-operative checklist to increase patient safety: a 1-year follow-up of personnel attitudes. Nilsson L, Lindberget O, Gupta A, Vegfors M. Department of Anesthesiology and Intensive Care, University Hospital, Linköping, Sweden. Acta Anaesthesiol Scand Feb;54(2): Epub 2009 Aug 31. BACKGROUND: The operating room is a complex work environment with a high potential for adverse events. Protocols for perioperative verification processes have increasingly been recommended by professional organizations during the last few years. We assessed personnel attitudes to a pre- operative checklist ('time out') immediately before start of the operative procedure. METHODS: 'Time out' was implemented in December 2007 as an additional safety barrier in two Swedish hospitals. One year later, in order to assess how the checklist was perceived, a questionnaire was sent by to 704 persons in the operating departments, including surgeons, anesthesiologists, operation and anesthetic nurses and nurse assistants. In order to identify differences in response between professions, each alternative in the questionnaire was assigned a numerical value. RESULTS: The questionnaire was answered by 331 (47%) persons and 93% responded that 'time out' contributes to increased patient safety. Eighty-six percent thought that 'time out' gave an opportunity to identify and solve problems. Confirmation of patient identity, correct procedure, correct side and checking of allergies or contagious diseases were considered 'very important' by 78-84% of the responders. Attitudes to checking of patient positioning, allergies and review of potential critical moments were positive but differed significantly between the professions. Attitudes to a similar checklist at the end of surgery were positive and 72-99% agreed to the different elements. CONCLUSION: Staff attitudes toward a surgical checklist were mostly positive 1 year after their introduction in two large hospitals in central Sweden.
 immediately before start of the operative procedure. METHODS: Time out was implemented in December 2007 as an additional safety barrier in two Swedish hospitals. One year later, in order to assess how the checklist was perceived, a questionnaire was sent by to 704 persons in the operating departments, including surgeons, anesthesiologists, operation and anesthetic nurses and nurse assistants. In order to identify differences in response between professions, each alternative in the questionnaire was assigned a numerical value. RESULTS: The questionnaire was answered by 331 (47%) persons and 93% responded that time out contributes to increased patient safety. Eighty-six percent thought that time out gave an opportunity to identify and solve problems. Confirmation of patient identity, correct procedure, correct side and checking of allergies or contagious diseases were considered very important by 78-84% of the responders. Attitudes to checking of patient positioning, allergies and review of potential critical moments were positive but differed significantly between the professions. Attitudes to a similar checklist at the end of surgery were positive and 72-99% agreed to the different elements. CONCLUSION: Staff attitudes toward a surgical checklist were mostly positive 1 year after their introduction in two large hospitals in central Sweden.")
116
3M Launches Skin and Nasal Antiseptic for Preoperative Use - Studies show antiseptic reduces 99.5% of S. aureus in nares - ST. PAUL, Minn. — Tuesday, February 9, 2010 Addressing the rising concern about surgical site infections caused by Staphylococcus aureus (S. aureus), including methicillin resistant Staphylococcus aureus (MRSA), 3M today announced the launch of the 3M™ Skin and Nasal Antiseptic (Povidone-Iodine Solution 5% w/w (0.5% available iodine) USP) Patient Preoperative Skin Preparation. This is the first product designed to reduce S. aureus in the nasal passages or nares, and is applied in the healthcare setting prior to surgery. Clinical studies show that the antiseptic kills 99.5% of S. aureus in the nares in one hour and maintains that level for at least twelve hours, an important benefit for patients undergoing surgery who may be at risk for infection.1 “Staphylococcus aureus is the leading cause of surgical site infections with approximately 80 percent of S. aureus infections caused by the patient’s own nasal flora2,” said Matt Scholz, corporate scientist, Infection Prevention Division at 3M. “As a patient preoperative skin preparation, 3M Skin and Nasal Antiseptic helps reduce the risk of S. aureus surgical site infection, including MRSA, which provides healthcare providers with confidence and control.” 6E &fn=Skin_Nasal_Launch_Release.pdf
, including methicillin resistant Staphylococcus aureus (MRSA), 3M today announced the launch of the 3M™ Skin and Nasal Antiseptic (Povidone-Iodine Solution 5% w/w (0.5% available iodine) USP) Patient. Preoperative Skin Preparation. This is the first product designed to reduce S. aureus in the nasal. passages or nares, and is applied in the healthcare setting prior to surgery. Clinical studies show. that the antiseptic kills 99.5% of S. aureus in the nares in one hour and maintains that level for at. least twelve hours, an important benefit for patients undergoing surgery who may be at risk for. infection.1. Staphylococcus aureus is the leading cause of surgical site infections with approximately 80. percent of S. aureus infections caused by the patient’s own nasal flora2, said Matt Scholz, corporate scientist, Infection Prevention Division at 3M. As a patient preoperative skin preparation, 3M Skin. and Nasal Antiseptic helps reduce the risk of S. aureus surgical site infection, including MRSA, which. provides healthcare providers with confidence and control. mwsId=66666UuZjcFSLXTtnXMVlXf_EVuQEcuZgVs6EVs 6E &fn=Skin_Nasal_Launch_Release.pdf.")
Similar presentations


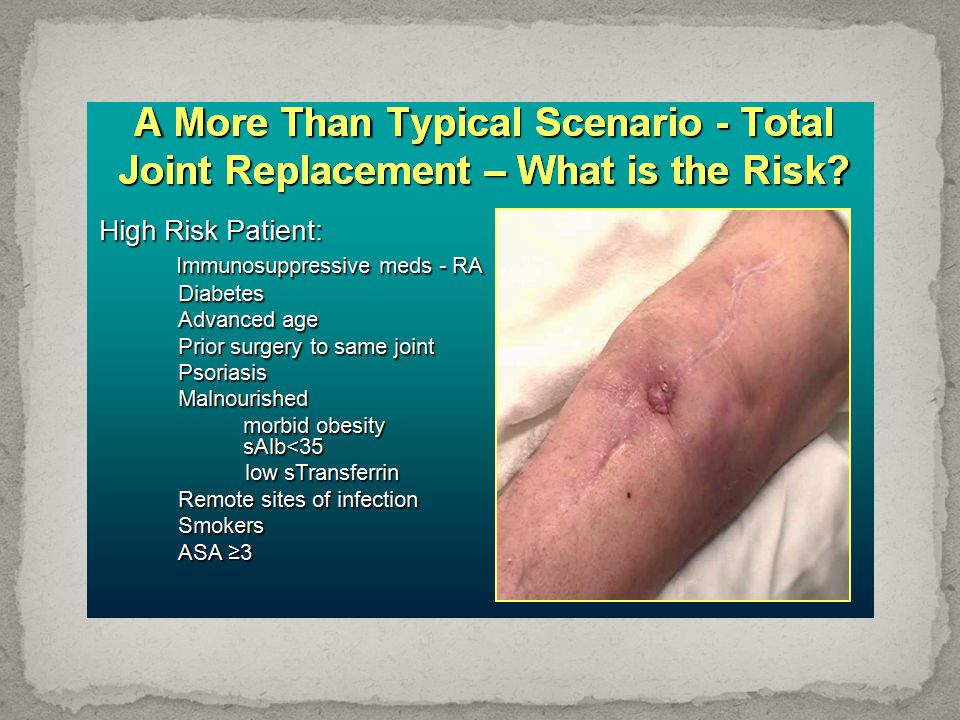
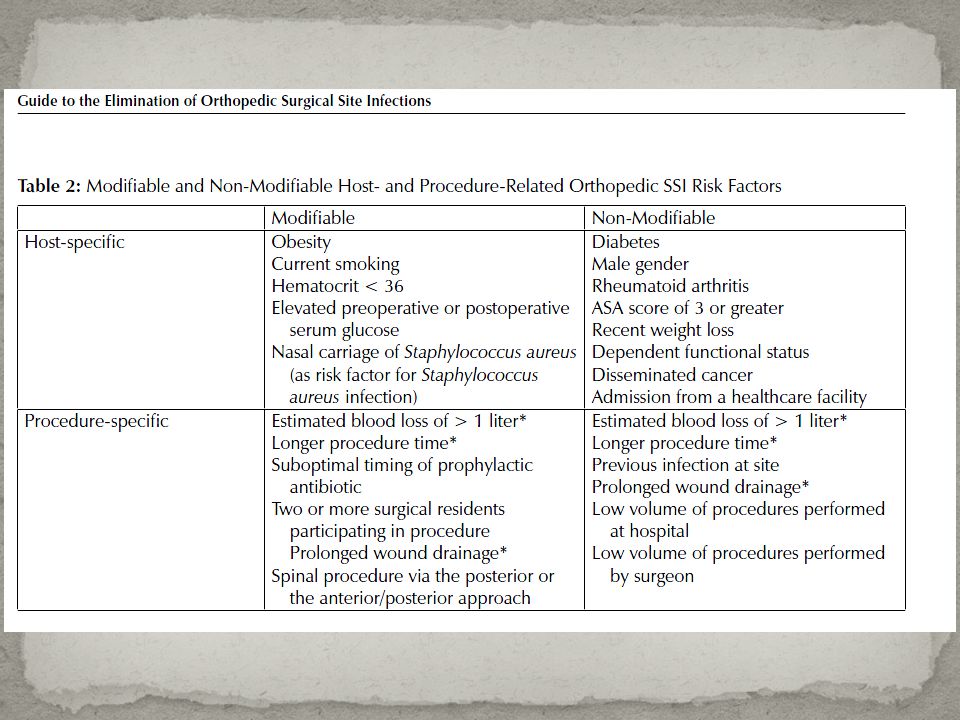

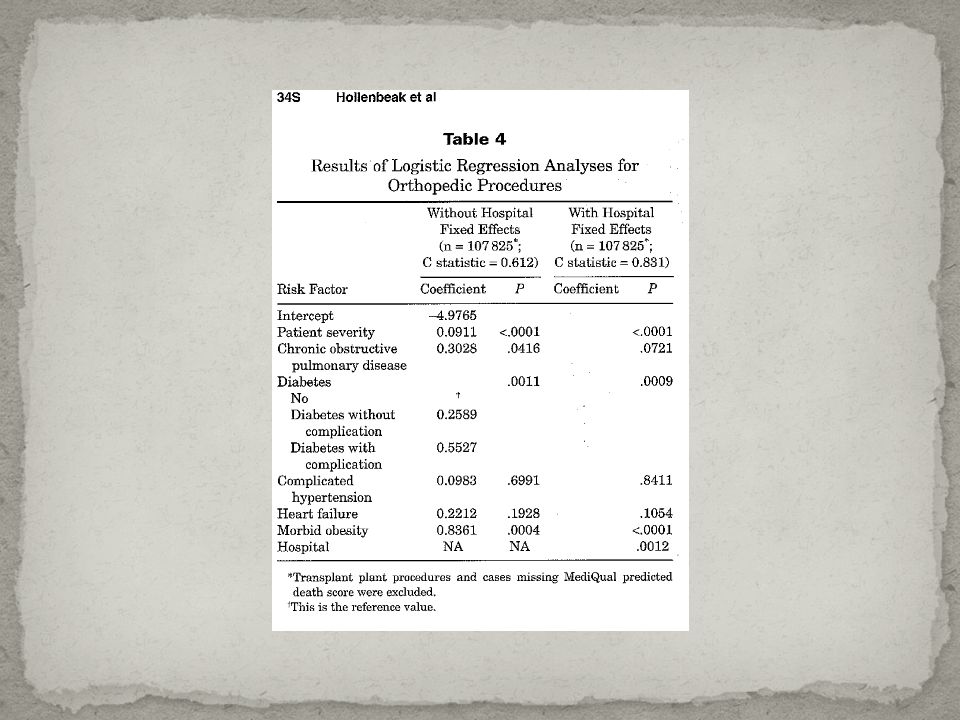

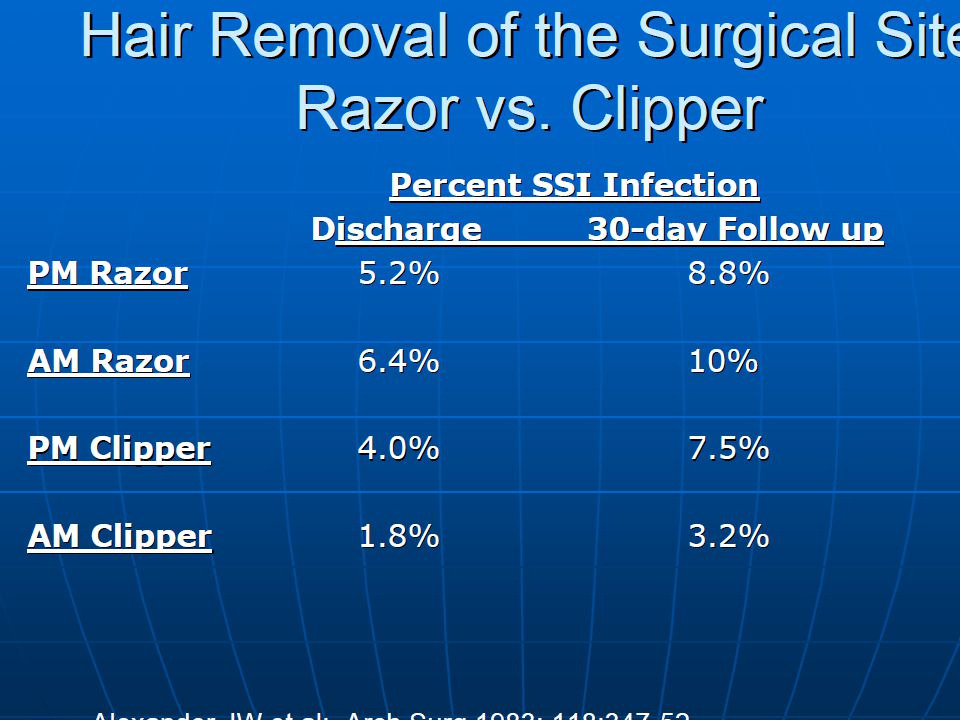









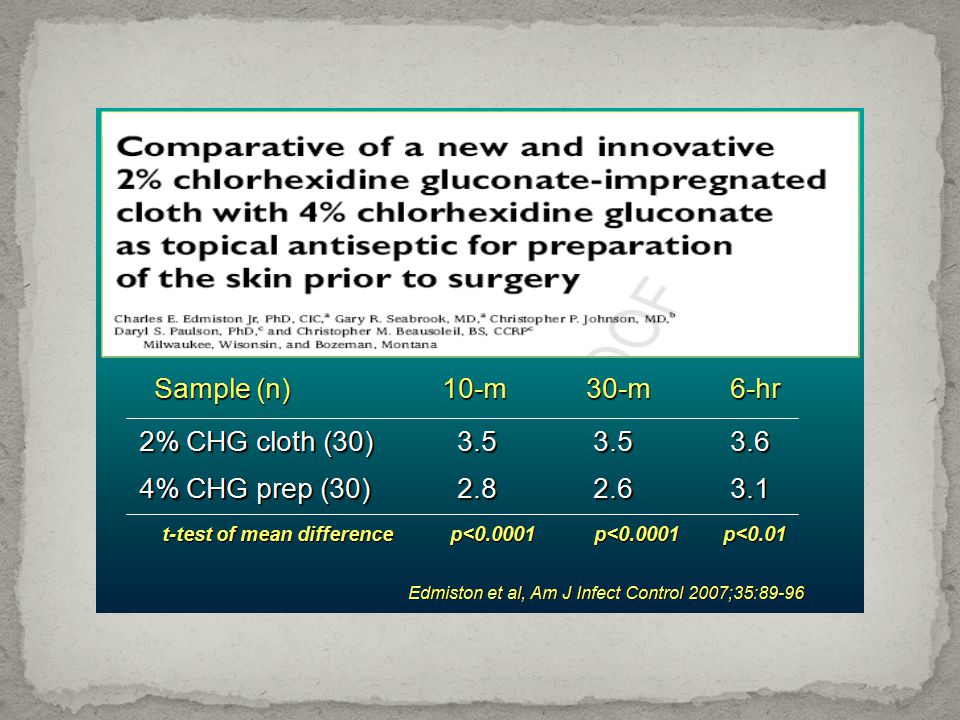
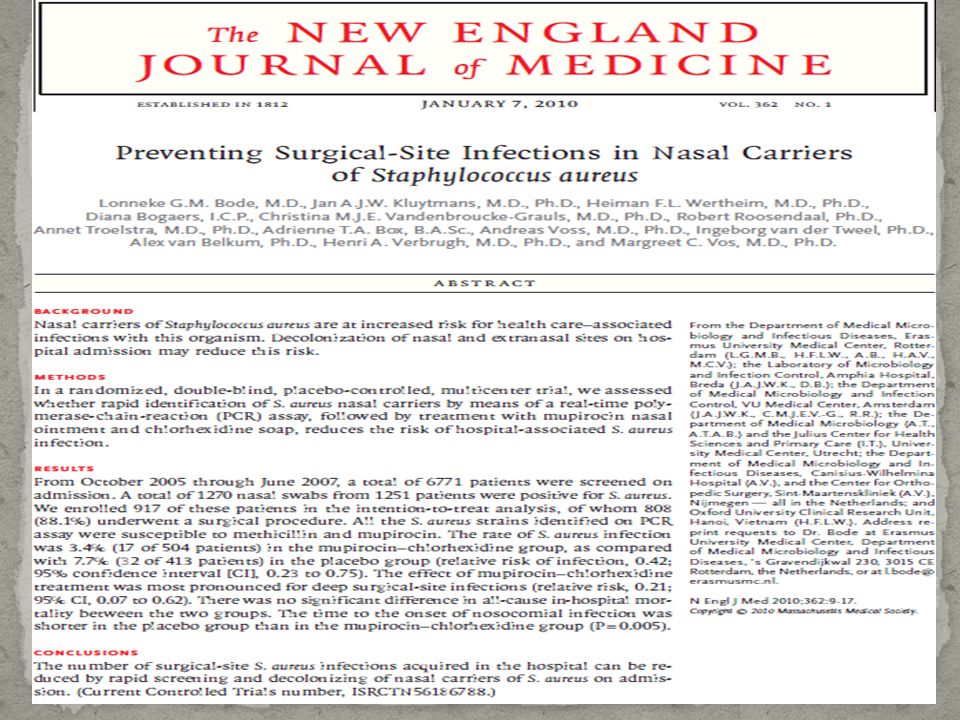





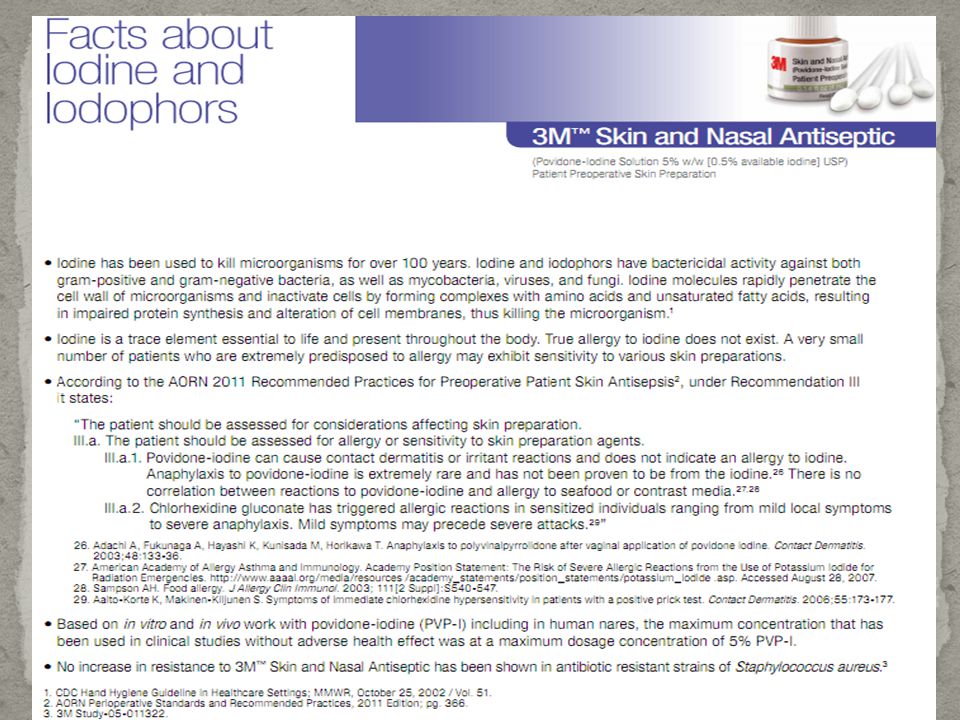
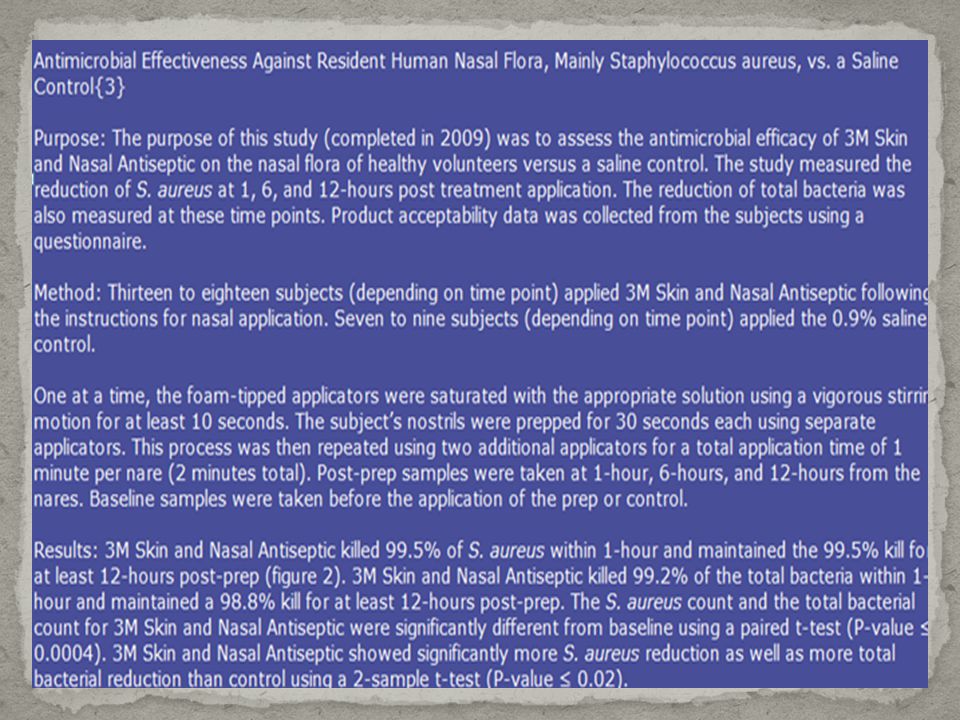

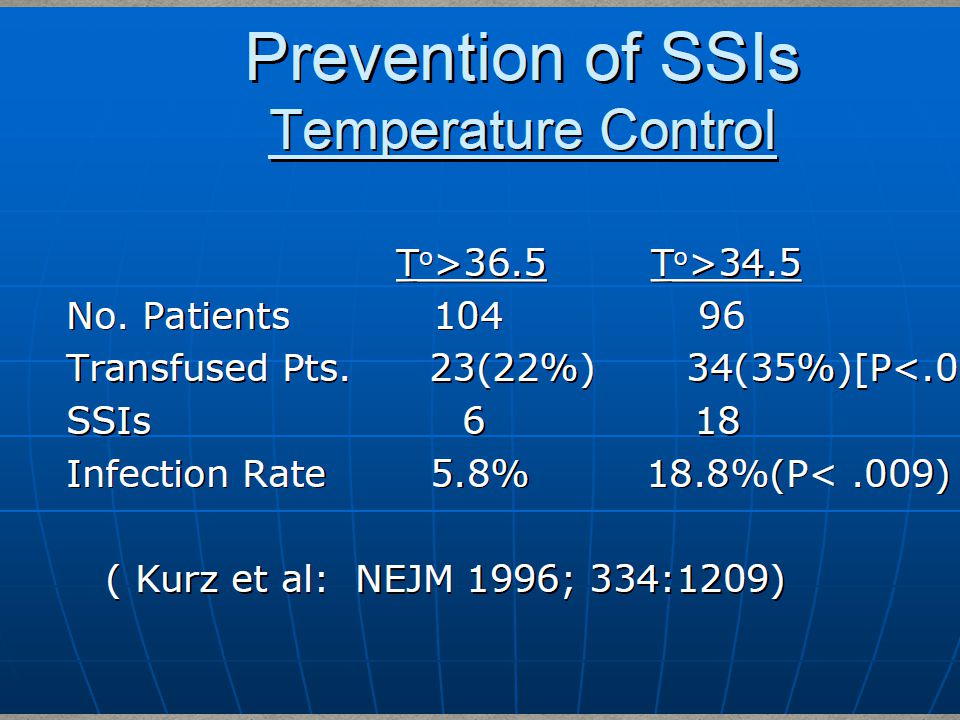



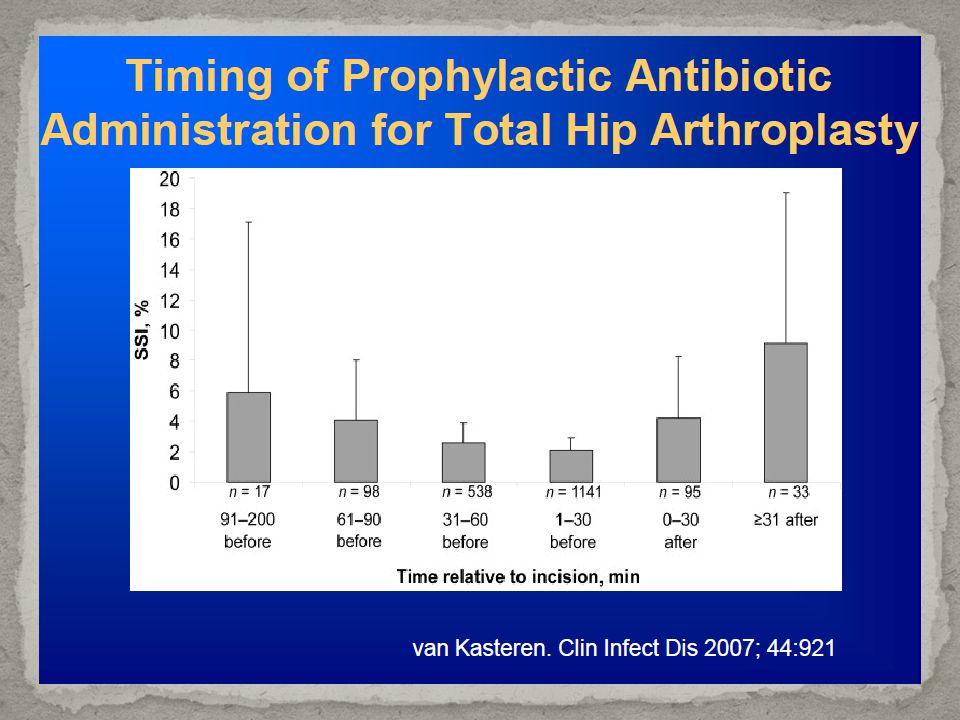









: What the Direct Caregiver Should Know>")





 CATHETER RELATED URINARY TRACT INFECTIN (CR-UTI)>")



>")



 Community Health Assessment Training July 16, 2008.>")