Download presentation
Presentation is loading. Please wait.

1
Fat Embolism Syndrome Dr Abhishek Ghosh Specialists Hospital, Kochi

2
Fat embolism syndrome First described by Zenker in 1861. Persistent debate has remained as to the specifics of the diagnosis and management of this clinical syndrome.

3
Fat Embolism syndrome Fat embolism syndrome(FES) is a serious manifestation of - respiratory - dermatological and - neurological symptoms.
 is a serious manifestation of - respiratory - dermatological and - neurological symptoms.")
4
Incidence Although fat embolization may occur in nearly 100% of traumatized patients, the incidence of FES ranges from 1% to 17%. Isolated long bone fractures - 2% to 5%. Multiply injured patient with long bone fractures or pelvic fractures- 15%. Ref:Ganong RB: Fat emboli syndrome in isolated fractures of the tibia and femur. Clin Orthop Relat Res 1993; 291:208-214.

5
Nontraumatic causes of FES Osteomyelitis, DM, Pancreatitis, Sickle cell hemoglobinopathies patients Steroid therapy, Alcoholic liver disease, Lipid infusion, Liposuction Bone marrow harvesting and transplants Bone tumor lysis, Cyclosporin A solvent

6
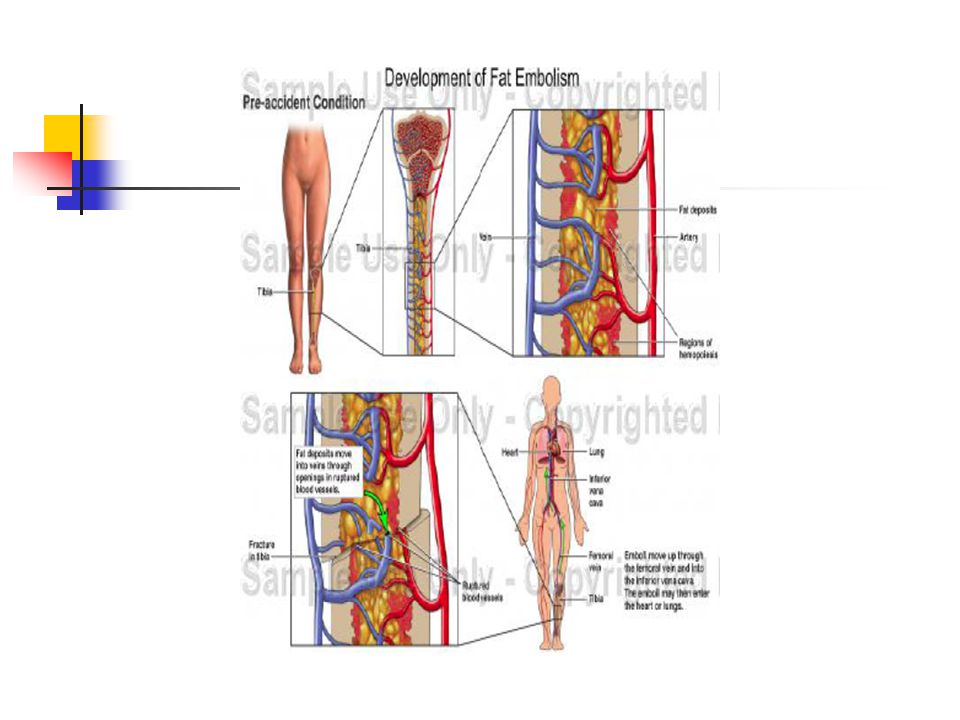
Pathophysiological mechanism Two theories - The mechanical theory: FES results from physical obstruction of the pulmonary and systemic vasculature with embolized fat. The biochemical theory: Circulating free fatty acids are directly toxic to pneumocytes and capillary endothelium in the lung FE can produce tissue damage by direct vascular occlusion, breakdown to toxic free- fatty acids, activation of platelets, and coagulative and fibrinolytic cascades with release of vasoactive amines.

7
Pathophysiological mechanism Histological finding include microvascular occlusion from fibrin and platelet aggregate, interstitial leakage of protein and neutrophil rich fluid, leading to diffuse alveolar damage. This causes AV shunting Detectable change include decrease functional residual capacity, decrease compliance and increase pulmonary vascular resistance.May progress to ARDS

9
Diagnosis FES remains a diagnosis of exclusion and is based on clinical criteria Early signs are - Dyspnea - Tachypnea - Hypoxemia The initial evaluation - ensure airway patency and air movement. Vital signs, including pulse oximetry, are obtained and supplemental O 2 provided immediately as other causes of failure are sought. A CXR and ABG analysis are mandatory, and other studies such as ECG, bronchoscopy, ventilation-perfusion (V./Q.) scanning, and CT scanning are considered.
 scanning, and CT scanning are considered..")
10
Gurd Criteria 3 major signs of hypoxia (PaO2 0.4), CNS depression, petechiae minor signs of tachycardia(HR>120), pyrexia(T>39), thrombocytopenia (plt<150K/uL), fat globules in urine or sputum, retinal emboli, decline in hematocrit which can’t be accounted for blood loss or fluid dilution 1 major and 3 minor or 2 major and 2 minor Ref: Gurd AR, Wilson RI. The fat embolism syndrome. J Bone Joint Surg Br 1974;56B:408-16.

11
Pulmonary manifestations Hypoxia, rales, pleural friction rub ARDS may develop ½ of pts with FES require mechanical ventilation (Bulger, Archives of Surgery 1997; 132: 435-9) CXR usually normal early on, later may show ‘snowstorm’ pattern- diffuse bilateral infiltrates
 CXR usually normal early on, later may show ‘snowstorm’ pattern- diffuse bilateral infiltrates")
12
Neurological findings Usually occur after respiratory symptoms Incidence 80% patients with FES Minor global dysfunction most common, but ranges from mild delirium to coma. Seizures/focal deficits not common but can occur Transient and reversible in most cases CT Head: general edema, usu nonspecific

13
Dermatologic Manifestations Petechiae about the head, neck, anterior thorax, and axilla are nearly pathognomonic for making a firm Dx of FES however: Only occur in 20-50% of the cases Typically occur after CNS and Respiratory involvement Petechiae represent fat globules lodged in dermal capillaries with extravasation of RBC’s

15
Prevalence of signs Archives of Surgery. 132(4):435-9, 1997 Apr
:435-9, 1997 Apr")
16
Laboratory test ABG shows hypoxia with Type I resp failure thrombocytopenia, anemia and hypofibrogenemia Fat globules in urine(6 of 11) but poor specificity
 but poor specificity")
17
Imaging Chest radiography: Serial radiographs reveal increasing diffuse bilateral pulmonary infiltrates within 24-48 hours of onset of clinical findings. Noncontrast head CT : Nuclear medicine ventilation/perfusion imaging of the lungs: for ruling out pulmonary embolus, the findings from this scan may be normal or may demonstrate subsegmental perfusion defects. Helical chest CT : Nodular or ground glass opacities in the setting of trauma suggest fat embolism. MRI : Scant data exist regarding MRI findings in patients with this syndrome; however, in one small patient group, multiple, nonconfluent, hyperintense lesions were seen on proton-density– and T2-weighted images. Transcranial Doppler sonography : In a small case study, 5 patients with trauma were monitored with intracranial Doppler sonography, 2 during intraoperative nailing of long bone fractures. 1 Cerebral microembolic signals were detected as long as 4 days after injury 1

18
Fat embolism vs. thromboembolism Fat embolism syndrome often occurred within 24-48 hrs after trauma, but thromboembolism is uncommon before 5 days after immobilization. Contrast venography is diagnostic gold standard of thromboembolism.

19
Bronchoalveolar Lavage The presence of lipid within alveolar macrophages obtained by bronchoalveolar lavage may help in the early diagnosis of FES.(1) The presence of fat droplets in alveolar macrophage is not a reliable method for diagnosis of FES after trauma, as many conditions are associated with fat droplets in alveolar macrophages.(2) Ref: 1.Benzer A, Offner D, Totsch M, et al: Early diagnosis of fat embolism syndrome by automated image analysis of alveolar macrophages. J Clin Monit 1994; 10:213-215. 2.Bronchoalveolar lavage in trauma patients for diagnosis of fat embolism syndrome. Chest. 1992;102:1323-1327.

20
Chest X-ray

21
Risk factors of fracture pattern The literature suggest a higher incidence of FES in patient with more than one long bone fracture. Location clearly favors the lower extremities, but no greater risk of total fracture population A highter proportion of open fracture in the group with FES(26%) than total fracture population Ref:1) Current concepts of respiratory insufficiency syndromes after fracture. Journal of Bone & Joint Surgery - British Volume. 83(6):781-91, 2001 Aug. 2)Fat embolism syndrome. A 10-year review. Archives of Surgery. 132(4):435-9, 1997 Apr
 than total fracture population Ref:1) Current concepts of respiratory insufficiency syndromes after fracture. Journal of Bone & Joint Surgery - British Volume. 83(6):781-91, 2001 Aug. 2)Fat embolism syndrome. A 10-year review. Archives of Surgery. 132(4):435-9, 1997 Apr.")
22
Management strategies Supportive care Adequate oxygenation(>90%)/ ventillation Intubation for hypoxia or altered mental status. Maintainence of hydration and haemodynamic stability( fluids, blood, ionotropes) DVT prophylaxis Nutrition
 DVT prophylaxis Nutrition.")
23
Indications for intubation SOAP - excessive S ecretions requiring pulmonary toilet, impaired O xygenation requiring positive pressure ventilation, A irway obstruction or inability to protect the airway compromised P ulmonary function

24
Ventilatory strategies Lung protective stratery: Low tidal volumes, adequate PEEP. Pressure-control mood(PCV) and inverse I:E ratio can increase mean distending pressure without increasing peak pressure. To achieves SaO2>90% with FiO2<0.6 and no significant cardiac output compromise prone position
 and inverse I:E ratio can increase mean distending pressure without increasing peak pressure. To achieves SaO2>90% with FiO2<0.6 and no significant cardiac output compromise prone position.")
25
Prophylactic measures Early fracture fixation decreases the incidence of FES and subsequent ARDS. Bone LB, Johnson KD, Wiegelt J, Scheinberg R. Early versus delayedstabilization of femoral fractures. J Bone Joint Surg Am. 1989;71:336-340. Johnson KD, Cadambi A, Seibert GB. Incidence of adult respiratory distresssyndrome in patients with multiple musculoskeletal injuries: effect of earlyoperative stabilization of fractures. J Trauma. 1985;25:375-384. Behrman SW, Fabian TC, Kudsk KA, Taylor JC. Improved outcome with femur fractures: early vs. delayed fixation. J Trauma. 1990;30:792-797.

26
Prophylactic Steroids Nearly all trials of both low and high dose methylprednisolone have demonstrated a reduction in the incidence of FES as well as less severe hypoxemia(1,2,3,4) But s ince most cases of FES are mild and the great majority of patients recover, concerns regarding the risk of infection and wound healing impairment have limited the routine use of corticosteroids.One rational, conservative approach would be to give prophylactic steroid therapy only to those patients at high risk for FES, eg, those with long bone or pelvic fractures, especially closed fractures.
 But s ince most cases of FES are mild and the great majority of patients recover, concerns regarding the risk of infection and wound healing impairment have limited the routine use of corticosteroids.One rational, conservative approach would be to give prophylactic steroid therapy only to those patients at high risk for FES, eg, those with long bone or pelvic fractures, especially closed fractures.")
27
1.Kallenbach J, Lewis M, Zaltzman M, Feldman C, Orford A, Zwi S. "Lowdose" corticosteroid prophylaxis against fat embolism. J Trauma 1987;27:1173-1176. 2. Lindeque BG, Schoeman HS, Dommisse GF, Boeyens MC, Vlok AL. Fatembolism and the fat embolism syndrome. A double blind therapeutic study.J Bone Joint Surg Br. 1987;69:128-131. 3. Schonfeld SA, Ploysongsang Y, DiLisio R, et al. Fat embolism prophylaxiswith corticosteroids: a prospective study in high-risk patients. Ann InternMed. 1983;99:438-443. 4.Rokkanen P, Alho A, Avikainen V, et al. The efficacy of corticosteroids in severe trauma. Surg Gynocol Obstet 1974;138:69-73.

28
Role of steroids in treatment Once FES is established, steroids have not shown improved outcomes. Though old studies in the 70's(1,2) had commented on the use of steroids and heparin no newer study has shown them to be of any value. The proposed mechanism of action of steroids is largely as an anti-inflammatory agent, reducing the perivascular haemorrhage and oedema and stabilizing the membrane. There are insufficient data to support initiating steroid therapy once fat embolism syndrome is established. There have been no prospective,randomized, and controlled clinical studies that have demonstrateda significant benefit with their use.
 had commented on the use of steroids and heparin no newer study has shown them to be of any value. The proposed mechanism of action of steroids is largely as an anti-inflammatory agent, reducing the perivascular haemorrhage and oedema and stabilizing the membrane. There are insufficient data to support initiating steroid therapy once fat embolism syndrome is established. There have been no prospective,randomized, and controlled clinical studies that have demonstrateda significant benefit with their use..")
29
Medications, including steroids, heparin, alcohol,have been found to be ineffective. (3,4,5,6,7,8,9,10) In addition steroids have the propensity to increase the incidence of infections, hamper BSL regulation and delays healing. Hence the use of steroids in the treatment of fat embolism syndrome is not advocated.
 In addition steroids have the propensity to increase the incidence of infections, hamper BSL regulation and delays healing. Hence the use of steroids in the treatment of fat embolism syndrome is not advocated..")
30
1.Can Med Assoc J. 1973 November 3; 109(9): 867–871. Fat embolism: a rational approach to treatment Arthur A. Scott and R. Peter Welsh 2.Emergency Orthopedics By Robert Rutha Simon, Steven J. Koenigsknecht 3.Fat embolism syndrome.J Am Board Fam Pract 14(4):310-313, 2001. © 2001 American Board of Family Practice 4.Shaikh N. Emergency management of fat embolism syndrome. J Emerg Trauma Shock 2009;2:29-33 5.Enneking FK. Cardiac arrest during total knee replacement. J Clin Anaesth 1995;7:253-63. 6. Fat embolism syndrome. Changing prognosis. C A Guenter and T E Braun.Chest 1981;79; 143-145 7.Shaikh N, Parchani A, Bhat V, Kattren MA. Fat embolism syndrome: Clinical and imaging considerations: Case report and review of literature. Indian J Crit Care Med [serial online] 2008 [cited 2009 Feb 26];12:32-6. 8. Early diagnosis of evolving fat embolism.... Dr. Deepanjali Pant, Dr. Narani K. K., Dr. Vijay Vohra, Dr. Jayashree Sood. Indian J of Anaes 2006;50(6):463-465 9.Fat embolism.Amandeep Gupta, MB BS FRCA; Charles S. Reilly, MD FRCA.Cont Edu Anaesth Crit Care & Pain. 2007;7(5):148-151. ©2007 Oxford University Press 10. Fat embolism.Dr. P. Glover, Critical Care and Resuscitation 1999; 1: 276-284
: , © 2001 American Board of Family Practice 4.Shaikh N. Emergency management of fat embolism syndrome. J Emerg Trauma Shock 2009;2: Enneking FK. Cardiac arrest during total knee replacement. J Clin Anaesth 1995;7: Fat embolism syndrome. Changing prognosis. C A Guenter and T E Braun.Chest 1981;79; Shaikh N, Parchani A, Bhat V, Kattren MA. Fat embolism syndrome: Clinical and imaging considerations: Case report and review of literature. Indian J Crit Care Med [serial online] 2008 [cited 2009 Feb 26];12: Early diagnosis of evolving fat embolism.... Dr. Deepanjali Pant, Dr. Narani K. K., Dr. Vijay Vohra, Dr. Jayashree Sood. Indian J of Anaes 2006;50(6): Fat embolism.Amandeep Gupta, MB BS FRCA; Charles S. Reilly, MD FRCA.Cont Edu Anaesth Crit Care & Pain. 2007;7(5): ©2007 Oxford University Press 10. Fat embolism.Dr. P. Glover, Critical Care and Resuscitation 1999; 1:")
31
Prognosis The duration of FES is difficult to predict because FES is often subclinical or overshadowed by other illnesses or injuries. Pt with FES may have persistent neurological deficits but generally recover in 1 yr. Mortality in Severe trauma from FES is usually between 5-15%.

32
Newer therapies Posttreatment with NAcetylCysteine was effective to alleviate the pathologic and biochemical changes caused by FE in rats Critical Care Medicine:Volume 36(2)February 2008pp 565-571
February 2008pp")
Similar presentations









>")

. - Major cause of mortality and morbity. in multiple trauma patients. - Most common 2 nd – 3 rd decode - Decrease on children.>")

>")



 Dr. Meg-angela Christi Amores.>")

 Acute Respiratory Distress Syndrome Paramedic Program Chemeketa Community College.>")

