Download presentation
Presentation is loading. Please wait.

1
Gonadotropin’s Bioactivity Dr. Vincenzo Volpicelli
Seconda Università degli Studi di Napoli Seconda Università degli Studi di Napoli Dipartimento di Scienze della Vita SUNfert Gonadotropin’s Bioactivity Fertility Center Cardito Dr. Vincenzo Volpicelli

2
Gonadotropins FSH, LH, HCG glycoproteins
dimers α, β (two peptide chain) α chain aspecific β chain specific (provides specificity for receptor interaction) Glycoproteins are proteins that contain oligosaccharide chains covalently attached to their side-chains. An oligosaccharide is a saccharide polymer containing a small number (typically three to ten) of component sugars, also known as simple sugars.
 α chain aspecific. β chain specific (provides specificity for receptor interaction) Glycoproteins are proteins that contain oligosaccharide chains covalently attached to their side-chains. An oligosaccharide is a saccharide polymer containing a small number (typically three to ten) of component sugars, also known as simple sugars.")
4
FSH heterodimeric hormone: The half-life of FSH is 3-4 hours
92 amino acids α-chain 111 amino acids β-chain The half-life of FSH is 3-4 hours Various types of FSH exist according to their sialic acid content Ben-Rafael Z, Levy T, Schoemaker J Pharmacokinetics of follicle-stimulating hormone: clinical significance. Fertil Steril. 63:689–700

5
LH The gene for the alpha subunit is located on chromosome 6q12.21.
The luteinizing hormone beta subunit gene is localized in the LHB/CGB gene cluster on chromosome 19q13.32

6
LH/HCG bioactivity LH & HCG: the same amino acids in sequence
LH & HCG both stimulate the same receptor the hCG β-subunit contains an additional 24 amino acids, both hormones differ in the composition of their sugar moieties. The different composition of these oligosaccharides affects bioactivity and speed of degradation. The biologic half-life: LH: 20 minutes FSH: 3-4 hours hCG: 24 hours

7
FSH, LH, HCG The protein dimer contains 2 polypeptide units, labeled alpha and beta subunits that are connected by two disulfide bridges The alpha subunits of LH, FSH, TSH, and hCG are identical, and contain 92 amino acids The beta subunits vary

8
hypothalamus (arcuate nucleus and preoptic area)
Gn secretion hypothalamus (arcuate nucleus and preoptic area) (Gn-RH pulses) pituitary gland Gn feed-back ovary estrogens
 (Gn-RH pulses) pituitary gland. Gn. feed-back. ovary. estrogens.")
9
Estradiol negative feed-back

10
Pituitary gland embryology

11
Pituitary gland by diencephalon (infundibulum) by Rathke pouch (mouth)
 by Rathke pouch (mouth)")
12
Pituitary portal system

13
Pituitary gland histology
FSH LH TSH ACTH HPRL GH

14
Gn mode action membrane receptors activate a PtdIns
Adenilcyclasi activation activate a PtdIns (phosphatidylinositol)-calcium second messenger system
-calcium second messenger system.")
15
Gn mode of action uterine blood flow:
(Index Resistance) uterine blood flow: increases the uterine blood flow during the early luteal phase, a periimplantation stage
 uterine blood flow: increases the uterine blood flow during the early luteal phase, a periimplantation stage.")
16
Gn mode of action increase in the number of receptor in preparation for ovulation After ovulation, the luteinized ovary maintains LH-R-s that allow activation in case there is an implantation

17
receptors activation binding LH to the external part of the membrane spanning receptor with LH attached, the receptor shifts conformation and thus mechanically activates the G protein and activates the cAMP system ~1% receptor sites activated The seven transmembrane α-helix structure of a G protein-coupled receptor such as LHCGR

18
Gn-R expression Its expression requires appropriate hormonal stimulation by FSH and estradiol present on: granulosa cells theca cells luteal cells interstitial cells

19
Extragonadal Gn-Rs physiologic role largely unexplored.
Gn-Rs have been found in: the uterus, sperm, seminal vesicles, prostate, skin, breast, adrenals, thyroid, neural retina, neuroendocrine cells, and (rat) brain. physiologic role largely unexplored.
 brain. physiologic role largely unexplored.")
20
Gn action in ovary follicular maturation ovulation luteal function

21
Gonadotropin’s avverse effects
OHSS Ovarian volume increased Multiple pregnancies Gynecomastia

22
FSH in early follicular phase
FSH threshold: FSH serum concentrations needed to stimulate ovarian follicle growth (Brown 1978) At the onset of the menstrual cycle, a cohort of small (2–5 mm) antral follicles is present in each ovary This cohort will continue to grow in response to stimulation by FSH a process referred to as follicle recruitment The follicle with the highest sensitivity will benefit most from increasing FSH levels and will subsequently gain dominance (leader leader) Scheele F, Schoemaker J The role of follicle-stimulating hormone in the selection of follicles in human ovaries: a survey of the literature and a proposed model. Gynecol Endocrinol. 10:55–66. Brown JB Pituitary control of ovarian function: concepts derived from gonadotropin therapy. Aust NZ J Obstet Gynaecol. 18:47–54
 At the onset of the menstrual cycle, a cohort of small (2–5 mm) antral follicles is present in each ovary. This cohort will continue to grow in response to stimulation by FSH. a process referred to as follicle recruitment. The follicle with the highest sensitivity will benefit most from increasing FSH levels and will subsequently gain dominance (leader leader) Scheele F, Schoemaker J The role of follicle-stimulating hormone in the selection of follicles in human ovaries: a survey of the literature and a proposed model. Gynecol Endocrinol. 10:55–66. Brown JB Pituitary control of ovarian function: concepts derived from gonadotropin therapy. Aust NZ J Obstet Gynaecol. 18:47–54.")
23
FSH in early follicular phase
FSH concentrations reach a maximum in the early follicular phase of the normal menstrual cycle and decrease thereafter not increase much during a normal ovulatory cycle FSH concentrations only 10–30% above the threshold level is sufficient to stimulate normal follicle development *Brown JB Pituitary control of ovarian function: concepts derived from gonadotropin therapy. Aust NZ J Obstet Gynaecol. 18:47–54. **Messinis IE, Templeton AA The importance of follicle-stimulating hormone increase for folliculogenesis. Hum Reprod. 5:153–156.

24
FSH in follicular phase
Stimulates: follicular growth, granulosa cell aromatase activity, induction of LH receptors on the granulosa cell membrane, estradiol secretion

25
Aromatase enzyme of the cytochrome P450 group
mediate androgens aromatization: producing estrogens sexual development

26
FSH in late follicular phase
decrease due to increased ovarian secretion of: E2 β-inhibin negative feedback at the hypothalamic-pituitary level Hotchkiss J, Knobil E The menstrual cycle and its neuroendocrine control. In: Knobil E, Neill JD, eds. The physiology of reproduction. New York: Raven Press; 711–750. Groome NP, Illingworth PJ, O’Brien M, et al Measurement of dimeric inhibin B throughout the human menstrual cycle. J Clin Endocrinol Metab. 81:1401–1405.

27
Granulosa Cell Thecal Cell blood Steroidogenesis LH FSH R R Basement
Membrane FSH cholesterol R CYP11 cAMP E2 pregnenolone R CYP17 Protein Kinase A 17-OH-P 17βHSD CYP17 E1 DHEA cAMP P4 3βHSD Protein kinase P450 Aldost Cortisol A A Steroidogenesis

28
FSH follicular decreasing
strict relationship with dominant follicle development As a consequence, other recruited follicles lack sufficient stimulation by FSH and enter atresia Zeleznik AJ, Hutchison JS, Schuler HM Interference with the gonadotropin-suppressing actions of estradiol in macaques overrides the selection of a single preovulatory follicle. Endocrinology. 117:991–999. Schipper I, Hop J and Fauser B: “The Follicle-Stimulating Hormone (FSH) Threshold/Window Concept Examined by Different Interventions with Exogenous FSH during the Follicular Phase of the Normal Menstrual Cycle: Duration, Rather Than Magnitude, of FSH Increase Affects Follicle Development”. The Journal of Clinical Endocrinology & Metabolism Vol. 83, No
 Threshold/Window Concept Examined by Different Interventions with Exogenous FSH during the Follicular Phase of the Normal Menstrual Cycle: Duration, Rather Than Magnitude, of FSH Increase Affects Follicle Development . The Journal of Clinical Endocrinology & Metabolism Vol. 83, No")
29
FSH follicular decreasing
Apparently, the maturing dominant follicle requires less FSH to continue its growth. It’s due to up-regulated FSH-sensitivity of leading follicle for: induction of locally various growth factors (IGF-I, AMH, inibina B, leptina, ICAM-1, VCAM-1, VEGF) induction of LH receptors that enhance FSH sensitivity Erickson GF The ovarian connection. In: Adashi EY, Rock JA, Rosenwaks Z, eds. Reproductive endocrinology, surgery, and technology. Philadephia: Lippincott-Raven; 1141–1160.
 induction of LH receptors that enhance FSH sensitivity. Erickson GF The ovarian connection. In: Adashi EY, Rock JA, Rosenwaks Z, eds. Reproductive endocrinology, surgery, and technology. Philadephia: Lippincott-Raven; 1141–1160.")
31
FSH in late luteal phase
At the end of the luteal phase, there is a slight rise in FSH that seems to be of importance to start the next ovulatory cycle a cohort of small antral follicles is prevented from undergoing atresia and is stimulated for further development Hodgen GD The dominant ovarian follicle. Fertil Steril. 38:281–300

32
LH mode action With the rise in estrogens, LH receptors are also expressed on the maturing follicle estrogen rise leads via the hypothalamic interface to the “positive LH feed-back” effect, a release of LH over a hour period This 'LH surge' triggers ovulation LH is necessary to maintain luteal function (P4) for the first two weeks LH supports thecal cells in the ovary that provide androgens and hormonal precursors for estradiol production In case of a pregnancy luteal function will be further maintained by the action of hCG (a hormone very similar to LH) from the newly established pregnancy
 for the first two weeks. LH supports thecal cells in the ovary that provide androgens and hormonal precursors for estradiol production. In case of a pregnancy luteal function will be further maintained by the action of hCG (a hormone very similar to LH) from the newly established pregnancy.")
33
FSH gene β-chain gene: locate in arme 6p21.1-23
locate in 11p13 only in gonadotrope cells of pituitary gland increased by Gn-RH and activine decreased by inhibine

34
Deficient gonadotropin’s level
hypogonadism and amenorrhoea: Kallmann syndrome Hypothalamic suppression Hypopituitarism Eating disorder (leptine) Hyperprolactinemia Gonadotropin deficiency Gonadal suppression therapy GnRH antagonist GnRH agonist (downregulation)
 Hyperprolactinemia. Gonadotropin deficiency. Gonadal suppression therapy. GnRH antagonist. GnRH agonist (downregulation)")
35
LH-R abnormalities in females can lead to infertility masculinization
In 46, XY pseudohermaphroditism, hypospadias micropenis Antibodies to LH-R can interfere with LH-R activity

36
High Gonadotropin levels
Persistently high LH levels are indicative of situations where the normal restricting feedback from the gonad is absent, leading to a pituitary production of both LH and FSH. Premature menopause Gonadal dysgenesis, Turner syndrome Castration Swyer syndrome Polycystic Ovary Syndrome Certain forms of CAH Testicular failure typical in the menopause

37
FSH in COH multiple follicle development is induced by elevating FSH concentrations far above the threshold By starting with a lower dose of gonadotropins and stepwise small increments, chances of inducing monofollicular growth should increase with a concomitant reduction of complications (step-up protocol) However, these stimulation protocols are characterized by FSH concentrations remaining above the threshold Polson DW, Mason HD, Saldahna MBY, Franks S Ovulation of a single dominant follicle during treatment with low-dose pusatile follicle stimulating hormone in women with polcystic ovary syndrome. Clin Endocrinol (Oxf). 26:205–212. White DM, Polson DW, Kiddy D, et al Induction of ovulation with low-dose gonadotropins in polycystic ovary syndrome: an analysis of 109 pregnancies in 225 women. J Clin Endocrinol Metab. 81:3821–3824.
 However, these stimulation protocols are characterized by FSH concentrations remaining above the threshold. Polson DW, Mason HD, Saldahna MBY, Franks S Ovulation of a single dominant follicle during treatment with low-dose pusatile follicle stimulating hormone in women with polcystic ovary syndrome. Clin Endocrinol (Oxf). 26:205–212. White DM, Polson DW, Kiddy D, et al Induction of ovulation with low-dose gonadotropins in polycystic ovary syndrome: an analysis of 109 pregnancies in 225 women. J Clin Endocrinol Metab. 81:3821–3824.")
38
FSH gate the "FSH-gate" or "FSH-window" concept has been proposed, which adds the element of time to the FSH threshold theory and emphasizes the significance of a transient increase in FSH above the threshold level for single dominant follicle development * Moreover, step-down dose regimen COH, has proven successful in reducing the incidence of multiple follicle development ** *Baird DT A model for follicular selection and ovulation: lessons from superovulation. J Steroid Biochem. 27:15–23 ** van Santbrink EJP, Donderwinkel PFJ, van Dessel HJHM, Fauser BCJM Gonadotrophin induction of ovulation using a step-down dose regimen: single-centre clinical experience in 82 patients. Hum Reprod. 10:1048–1053

39
FSH window the FSH window concept has been proposed, stressing the significance of the (limited) duration of FSH elevation above the threshold level rather than the height of the elevation of FSH for single dominant follicle selection Fauser BCJM, van Heusden AM Manipulation of human ovarian function: physiological concepts and clinical consequences. Endocr Rev. 18:71–106.

40
Gn dosage For assisted reproductive technology procedures, the usual initial dose is 150 IU to 225 IU daily for 5 days. The dose is then adjusted according to response and is usually continued for 6 to 12 days. When an adequate response is achieved, this medication is stopped and another medication, hCG, is given to induce ovulation.

41
FSH initial doses patient’s age basal FSH PCOS

42
HCG HCG Gonasi fl i.m. 1000, 2000, 5.000 UI pregnant women urine
made by the placenta LH-activity like > half-life LH (4 h vs. 15 min) Gonasi fl i.m. 1000, 2000, UI
 Gonasi fl i.m. 1000, 2000, UI.")
43
hCG in normal pregnancy

44
HCG It is heterodimeric glycoprotein:
α subunit identical to LH, FSH, TSH β subunit unique to hCG amino acids

45
HCG mode action interacts with the LHCG receptor
Follicle rupture induction maintenance of the corpus luteum during the beginning of pregnancy, causing it to secrete P4 meiosis restarting

46
HMG Menotropin (HMG) (1965s) FSH + LH (~ 50%) Urofollitropin (1983)
Climateric women urine FSH + LH (~ 50%) 5% Gn + 95% urinary proteins Urofollitropin (1983) Purified FSH (>95%) purified by chromatographic techniques (Pergonal), (Metrodin), Menogon, Fostimon fl i.m. 75 UI
 5% Gn + 95% urinary proteins. Urofollitropin (1983) Purified FSH (>95%) purified by chromatographic techniques. (Pergonal), (Metrodin), Menogon, Fostimon fl i.m. 75 UI.")
47
Chinese hamster (Cricetulus griseus), white spotted type
, white spotted type")
48
r-FSH produced by inserting the genes encoding for α and β subunits of FSH into expression vectors that are transfected into a Chinese hamster ovary cell line Purification by immunochromatography using an antibody specifically binding FSH Gonal-F, Puregon fl s.c., pen

49
r-FSH 1995 European Medicines Evaluation Agency (EMEA)
Gonal-F, Puregon fl s.c., pen

50
r-FSH properties knockdown degradation rate reduced variability interblocks firmness high degree of pureness diminished immunization

51
α-follitropine (Gonal F)
r-FSH α-follitropine (Gonal F) β-follitropine (Puregon) r-LH (Luveris 75 IU fl s.c.)
 β-follitropine (Puregon) r-LH (Luveris 75 IU fl s.c.)")
52
HMG vs. r-FSH both products are probably equally safe and similar in efficacy, based on the available literature to date. Matorras R, Rodriguez-Escudero FG: “Debate. Bye-bye urinary gonadotropins?” . Hum Reprod ;17:1675–1683 Suheil J. Muasher, Rony T. Abdallah, Ziad R. Hubayter: “Optimal stimulation protocols for in vitro fertilization”. Fertil Steril 2006; 86,2:

53
Follicles recruitment
FSH-HMG-HCG target target FSH/HMG LH HCG Follicles recruitment + + + Oocytes maturation + + Ovulation trigger E2 P4

54
Gn available in the Italy market
Gonadotropin 75 UI 1.500 UI Meropur € 12,28 € 245,6 Fostimon € 16,09 € 321,8 Puregon € 45,83 € 916,6 Gonal-F € 51,39 € 1027,8

55
COH PROTOCOLS

56
CC CC alone produces sufficient enhanced follicular recruitment
Clomiphene alone had significantly fewer follicles necessary gonadotropin support to be continued to prevent atresia of some of the cohort of follicles supplemental hCG/P4 to corrected short luteal phases M. M. Quigley: Annals of the New York Academy of Sciences, Vol 442, 1:

57
CC + HMG HMG150 IU every other day starting on day 5
CC 100 mg/day on day 3–7 of the menstrual cycle HMG150 IU every other day starting on day 5 HCG on leading follicle >18 mm and at least two follicles >15 mm Pick-up or IUI hours after HCG UI 6 days after (staff conversion) P4 50 mg/d i.m. on HCG day or E-T day M. M. Quigley: Annals of the New York Academy of Sciences, Vol 442, Issue
 P4 50 mg/d i.m. on HCG day or E-T day. M. M. Quigley: Annals of the New York Academy of Sciences, Vol 442, Issue")
58
CC + delayed HMG CC 100 mg/day on day 1–5 day
HMG150 IU every other day starting on day 6 HCG on leading follicle >18 mm and at least two follicles >15 mm IUI or Pick-up hours after HCG UI 6 days after (staff conversion) P4 50 mg/d i.m. on HCG day or E-T day
 P4 50 mg/d i.m. on HCG day or E-T day.")
59
CC + HMG best chance of COH
minimize the disruption of the subsequent luteal phase increased pregnancy rate M. M. Quigley: Annals of the New York Academy of Sciences, Vol 442, Issue

60
CC + HMG ovulation outcome
90% for cycle

61
CC/HMG Pregnancy Outcome
USG pregnancy rate/cycle: 25% * live-birth rates/cycle : 13-17% * * Published overall

62
integrins down regulation
Miscarriage integrins down regulation (markers of endometrial receptivity) endometrial EE/P-r depletion uterine artery flow impaired endometrial development
 endometrial. EE/P-r depletion. uterine artery flow. impaired endometrial development.")
63
Low Pr in CC/Gn COH desynchronized endometrial development
premature LH surge immature oocytes

64
CC/HMG Pr lower over 38 years old low ovarian reserve
poor quality sperm endometriosis tubal damage or pelvic scar tissue infertility >3 years

65
CC/HMG adverse effects
3,5% twin 1/3 of admission in TIN Twin/mono mortality 10 + PIH 5 – 10 + placenta previa Placenta detachment

66
CC + E2 CC 100 mg/d on 3° cycle day EE 0.05 mg/d on days 8-12
hCG 10,000 IU at least one follicle was >18 mm A single IUI/Pick-up 24–36 hours after progesterone 50 mg daily IM on day of E-T or 3 days after IUI* until β-hCG levels were evaluated * Gerli: Intrauterine insemination. Fertil Steril 2000; 73,1:85-89

67
CC + E2 endometrial thickness on the day of hCG administration.
= CC only = CC + ethinyl E2

68
CC + E2 Characteristics and outcome of patients who received CC plus ethinyl E2 (group A) or CC alone (group B) in IUI cycle Characteristic Group A Group B P value No. of patients 32 - - Mean (±SD) age (y) 28.0 ± 5.6 26.0 ± 4.2 NS Mean (±SD) duration of infertility (mo) 48.1 ± 18.5 36.7 ± 9.6 Ongoing Pregnancy 12 (37.5) 2 (6.25) <.05 Miscarried 6 (18.75) pulsatility index values no difference
 age (y) 28.0 ± ± 4.2. NS. Mean (±SD) duration of infertility (mo) 48.1 ± ± 9.6. Ongoing Pregnancy. 12 (37.5) 2 (6.25) <.05. Miscarried. 6 (18.75) pulsatility index values. no difference.")
69
Traditional COH HMG or r-FSH 300 IU on 2° day cycle
HCG IU on leading follicle >17 mm and at least two follicles >15 mm Pick-up after h P4 50 mg i.m. for luteal supplementation

70
Traditional COH FSH remain elevated
recruitment and growth of ovarian follicles continues throughout treatment This FSH serum pattern profoundly diverges from the spontaneous menstrual cycle * Filicori M: Characterization of the physiological pattern of episodic gonadotropin secretion throughout the human menstrual cycle . J Clin Endocrinol Metab ;62:1136–1144

71
Traditional COH heterogeneous size cohorts of follicles are often found at hCG day the optimal outcome of COH would be the selective attainment of numerous large mature homogeneous follicles. * Arnot AM , Vandekerckhove P , DeBono MA , Rutherford AJ . Follicular volume and number during in-vitro fertilization (association with oocyte developmental capacity and pregnancy rate) . Hum Reprod ;10:256–261
 . Hum Reprod ;10:256–261.")
72
Traditional protocol Long protocol
n° ampules 5.7 25 Mature oocytes 8 16 Fertilization rate 83% 78% PR/ET 28% 31% Cost-saving + + + — — MF Stress

74
Gn-RH Gn-RH neurons are inside the medium-basal hypothalamus (arcuate nucleus and median eminence) Lately scientists showed Gn-RH syntesis in pituitary gland too

75
Gn-RH biochemistry (1977s)
a decapeptide (10 amino acids) in mammals. This chain is represented by: pyroGlu-His-Tyr-Ser-Gly-Leu-Arg-Pro-Gly-NH2 The identity of GN-RH1 was clarified by the Nobel Laureates Roger Guillemin and Andrew V. Schally
 in mammals. This chain is represented by: pyroGlu-His-Tyr-Ser-Gly-Leu-Arg-Pro-Gly-NH2. The identity of GN-RH1 was clarified by the 1977 Nobel Laureates Roger Guillemin and Andrew V. Schally.")
76
Pituitary gland histology
Melanocyte-stimulating hormone (MSH) by pars intermedia (part of adenohyphysis) is the predominant hormone secreted
 by pars intermedia (part of adenohyphysis) is the predominant hormone secreted.")
77
NEUROHYPOPHYSIS - PARS NERVOSA
This region of the pituitary is non secretory. Its cells are neuroglial-like pituicytes. The pars nervosa stores ADH and Oxytocin which were secreted by the hypothalamus.

78
Melatonin/steroidogenesis
The direct involvement of melatonin in modulation of ovarian steroidogenesis, the high levels of melatonin found in human follicular fluid, and the presence of melatonin binding sites in the ovary led us to hypothesize that melatonin acts as a modulator of ovarian function. the mechanism of melatonin action at the level of the ovary is still poorly understood

79
Melatonin/steroidogenesis +
P4

81
Gn-RH secretion males/females
in males, in pulses at a constant frequency in females the frequency of the pulses varies during the menstrual cycle there is a large surge of GN-RH1 just before ovulation

82
Gn-RH frequency Low frequency FSH release high frequency LH release

83
The seven transmembrane α-helix structure of a G protein-coupled receptor

84
Gn-Rh analogues While Gn-RH1 has been synthesized and become available, its short half-life requires infusion pumps for its clinical use. Modifications of the decapeptide structure of Gn-RH1 have led to Gn-RH1 analog medications that either stimulate (Gn-RH1 agonists) or suppress (Gn-RH1 antagonists) the gonadotropins
 or suppress (Gn-RH1 antagonists) the gonadotropins.")
85
Effects of Gn-RH analogues
agonist antagonist Prevent premature luteinization + + + + + Prevent premature ovulation To synchronize early follicular development +

86
Gn-RH agonist is a synthetic peptide modeled after the hypothalamic neurohormone Gn-RH that interacts with its receptor to elicit its biologic response, the release of the pituitary hormones FSH and LH Agonists do not quickly dissociate from the Gn-RH receptor As a result initially there is an increase in FSH and LH secretion (so-called flare-up effect) however after about ten days a profound hypogonadal effect is achieved through receptor down-regulation. Generally this induced and reversible hypogonadism is the therapeutic goal. Gn-RH agonists are synthetically modeled after the natural Gn-RH decapeptide with specific amino acid substitutions typically in position 6 and 10.
 however after about ten days a profound hypogonadal effect is achieved through receptor down-regulation. Generally this induced and reversible hypogonadism is the therapeutic goal. Gn-RH agonists are synthetically modeled after the natural Gn-RH decapeptide with specific amino acid substitutions typically in position 6 and 10.")
87
Gn-RH-a Aminoacid sequence 6 10
name act 1 2 3 4 5 6 7 8 9 10 for Gn-RH Pyro-glu His Trp se ro to nin Tyr Leu Arg Pro Gly-NH2 iv Leuproreline* 15 D-Leu N-EtNH2 sc, im Buserelin * * 20 D-Ser triptor * * * D-Trip Goserelin* * * * 100 AzGly-NH2 depot sc * Enantone 3.75, mg fl s.c. im; Enantone die 1 mg/die (0.2 ml) fl s.c.; * * Suprefact 5.5 ml fl s.c.; Suprefact spray nasale 10 gr (1 buff = 200 mg) * * * Decapeptyl 3.75, mg fl s.c. im; Decapeptyl die 0.1 mg fl s.c. * * * * Zoladex 3.6, 10.8 mg fl s.c. im Triptorelin is an agonist with only a single substitution at position 6
 fl s.c.; * * Suprefact 5.5 ml fl s.c.; Suprefact spray nasale 10 gr (1 buff = 200 mg) * * * Decapeptyl 3.75, mg fl s.c. im; Decapeptyl die 0.1 mg fl s.c. * * * * Zoladex 3.6, 10.8 mg fl s.c. im. Triptorelin is an agonist with only a single substitution at position 6.")
88
Gn-RH-a triptorelin, buserelin and goserelin are equally effective
brand name Injection mg/ml Leuproreline acetate Enantone die 1 fl 1.6 ml 8 doses 1 mg (0.2 ml) s.c Triptoreline Decapeptyl depot 1 fl i.m. 3.75 mg Decapeptyl die 14 fl pre-filled 0.2 ml (0.1 mg) s.c. daily Buserelin Suprefact fl 5.5 ml 0.5 ml/d spray 1 flac 1 buff = 100 μg triptorelin, buserelin and goserelin are equally effective
 s.c. Triptoreline. Decapeptyl depot. 1 fl i.m mg. Decapeptyl die. 14 fl. pre-filled. 0.2 ml. (0.1 mg) s.c. daily. Buserelin. Suprefact fl. 5.5 ml. 0.5 ml/d. spray. 1 flac. 1 buff = 100 μg. triptorelin, buserelin and goserelin are equally effective.")
89
Gn-RH-a pharmacokinetics
two hours: peak serum. It rapidly binds to the LHRH receptor cells in the pituitary gland thus leading to an initial increase in production of LH (flare-up) after 10 days: receptor desensitization and/or down-regulation
 after 10 days: receptor desensitization and/or down-regulation.")
90
Gn-RH-a lysine replacement with ethylamide in 10 → half-time (4 min vs 3 h)
")
91
Gn-RH-a lysine replacement with D-amynoacide in 6 → Increase effectiveness ( times) D-aminoacid is hydrophobe chain carrier with enhancement receptor link

92
Gn-RH-a effects Follicles synchronization ++++
Fewer small follicles on HCG day ++ Avoids premature luteinization Multiple pregnancies ≡ ≡ ≡ Decreases OHSS frequency

93
Triptoreline depot serum levels

94
Triptorelin [d-Trp6]GnRH
![Triptorelin [d-Trp6]GnRH](http://slideplayer.com/slide/2803302/10/images/94/Triptorelin+%5Bd-Trp6%5DGnRH.jpg "Triptorelin [d-Trp6]GnRH")
95
Goserelin* * Zoladex 3.75 mg, 11.25 mg fl im (FDA, 1989)
D-Ser(But)6Azgly10LHRH * Zoladex 3.75 mg, mg fl im (FDA, 1989)
6Azgly10LHRH. * Zoladex 3.75 mg, mg fl im (FDA, 1989)")
96
Goserelin* has a serum elimination half-life of two to four hours in patients with normal renal function. After administration, peak serum concentrations are reached in about two hours after a period of about days, production of LH is greatly reduced due to receptor downregulation

97
Gn-RH-a protocols long protocol short (“flare-up”) protocol
ultrashort protocol microdose flare protocol

98
Long protocol: Avoid pre-menses FSH surge Follicles timing
Avoid premature LH surge Higher follicular recruitment (synchronization) Improvement immune attitude Expensive cost High responders PCOS
 Improvement immune attitude. Expensive cost. High responders. PCOS.")
99
short protocols follicles timing avoid premature LH surge
lower follicular recruitment make procedures easier Poor responders

100
Short/long protocol (Volpicelli V. 2003)
Serum levels Short protocol Long protocol E2 idem Idem D4 +++ + depression Pregnancy rate/cicle 9.2% 16. 5% PR/transfer 9..9% 23. 5% patients «poor responders» «High responders» PCOS > 40 years hyrsutism HMG ampules Cancelled cycles

101
PR/transfer in Gn-RH-a
Flare-up protocol 19.2% Long protocol 25.7% Media 24.8% without analogues 23.2% FIV nel periodo (da FIV-NAT ’97) sec. Barrière et al. 1999
 sec. Barrière et al")
102
Gn-RH-a Long protocol Gn-Rh-a depot 3.75 mg in one dose on 21st day only of previous cycle Gn-Rh-a low-dose daily on the 21st day of previous cicle to HCG day: Buserelin (Suprefact fl 5.5 ml) 0.3 ml fl s.c. Buserelin nasally 1 buff x 3/d (300 μg) Leuproreline (Enantone die fl s.c.) 0.2 ml/day Triptoreline (Decapeptyl die fl s.c.) 0.2 ml or on any day when: LH <0.5 E2 <30 No ovarian cyst >10 mm 8
 0.3 ml fl s.c. Buserelin nasally 1 buff x 3/d (300 μg) Leuproreline (Enantone die fl s.c.) 0.2 ml/day. Triptoreline (Decapeptyl die fl s.c.) 0.2 ml. or. on any day when: LH <0.5. E2 <30. No ovarian cyst >10 mm. 8.")
103
Gn-RH-a long protocol r-FSH/HMG IU/day on 2nd cycle day to HCG day HCG IU on the least two follicles >18 mm Pick-up after hours P4 supplementation HCG IU six days after E-T 8

104
Short (flare-up) protocol
9 Short (flare-up) protocol Gn-RH-a 3.75 mg depot ½ fl i.m. on 2° cycle day only r-FSH IU/d on 3th day (step-down regimen) HCG IU (18 mm ) Pick-up after h HCG (+ P4) poor responder
 protocol. Gn-RH-a 3.75 mg depot ½ fl i.m. on 2° cycle day only. r-FSH IU/d on 3th day (step-down regimen) HCG IU (18 mm ) Pick-up after h. HCG (+ P4) poor responder.")
105
Gn-RH-a flare low dose protocol
EE-P for 1-2 cycles on 1st cycle day at HCG day: Triptoreline (decapeptyl die) 0.2 ml (0.1 mg) s.c. daily Leuproreline acetate (enantone die) 0.2 ml (1 mg) s.c. daily Buserelin (Suprefact flac 5.5 ml) 0.3 ml s.c. Buserelin nasally 3 buff/day (300 μg) or on any day when: LH <0.5 E2 <30 No ovarian cyst >10 mm r-FSH/HMG UI/d on 3rd cycle day After administration s.c. enantone die reachs a serum peak of 32.3 mg/ml in 0.6 h
 0.2 ml (0.1 mg) s.c. daily. Leuproreline acetate (enantone die) 0.2 ml (1 mg) s.c. daily. Buserelin (Suprefact flac 5.5 ml) 0.3 ml s.c. Buserelin nasally 3 buff/day (300 μg) or. on any day when: LH <0.5. E2 <30. No ovarian cyst >10 mm. r-FSH/HMG UI/d on 3rd cycle day. After administration s.c. enantone die reachs a serum peak of 32.3 mg/ml in 0.6 h.")
106
Gn-RH-a ultrashort protocol
11 on 2nd cycle day for three days: Triptoreline 0.2 ml s.c Leuproreline 0.2 ml s.c. Buserelin 0.5 ml s.c. Buserelin nasally 3 buff/day or on any day when: LH <0.5 E2 <30 No ovarian cyst >10 mm r-FSH/HMG on the 2nd cycle day

107
11 ~ ~ ~ Ultrashort Long + + + HMG ampoules cancelled cycles
n. oocytes fertilization rate embryo cleavage rate supernumerary embryos Samuel F. Marcus: “Comparative trial between an ultra-short and long protocol of luteinizing hormone-releasing hormone agonist for ovarian stimulation in in-vitro fertilization”. Human Reproduction, 1993; Vol. 8, No. 2, pp

108
HCG low-dose long protocol
12 HCG low-dose long protocol Granulosa cells in ovarian follicles of larger size (>10–12 mm) normally express the LH/hCG receptor and become sensitive to LH activity stimulation (1). For a long time it was thought that this physiologic phenomenon was finalized to make mature follicles susceptible to the midcycle LH surge and thus ovulate. Nevertheless, GCs LH/hCG receptors may also be highly relevant to permit continued dominant follicle growth in the spontaneous mid-late follicular phase, at a time when the physiologic serum FSH decline may curtail adequate GC support and growth. At this time LH appears capable of exerting virtually all the physiologic actions of FSH on GCs (2). 1. Zeleznik AJ , Hillier SG . The role of gonadotropins in the selection of the preovulatory follicle . Clin Obstet Gynecol ;27:927–940 . 2. Campbell BK , Dobson H , Baird DT , Scaramuzzi RJ . Examination of the relative role of FSH and LH in the mechanism of ovulatory follicle selection in sheep . J Reprod Fertil ;117:355–367
 normally express the LH/hCG receptor and become sensitive to LH activity stimulation (1). For a long time it was thought that this physiologic phenomenon was finalized to make mature follicles susceptible to the midcycle LH surge and thus ovulate. Nevertheless, GCs LH/hCG receptors may also be highly relevant to permit continued dominant follicle growth in the spontaneous mid-late follicular phase, at a time when the physiologic serum FSH decline may curtail adequate GC support and growth. At this time LH appears capable of exerting virtually all the physiologic actions of FSH on GCs (2). 1. Zeleznik AJ , Hillier SG . The role of gonadotropins in the selection of the preovulatory follicle . Clin Obstet Gynecol ;27:927– Campbell BK , Dobson H , Baird DT , Scaramuzzi RJ . Examination of the relative role of FSH and LH in the mechanism of ovulatory follicle selection in sheep . J Reprod Fertil ;117:355–367.")
109
HCG low-dose in a-long protocol
12 HCG low-dose in a-long protocol Based on this information we postulated that LH activity could substitute FSH administration in the late stages of COH to allow larger follicles growth and maturation. 1. Filicori M , Cognigni GE , Taraborrelli S , Parmegiani L , Bernardi S , Ciampaglia W . Intracytoplasmic sperm injection pregnancy after low-dose human chorionic gonadotropin alone to support ovarian folliculogenesis . Fertil Steril ;78:414–416

110
HCG low-dose long protocol
12 HCG low-dose long protocol The longer half-life and greater affinity for the LH/hCG receptor of hCG account for a potency ratio estimate of hCG-to-LH of around 1:6 (1,2). hCG alone (200 IU/d), corresponding to roughly 1,200 IU/d of LH The hCG is also drastically less expensive than recombinant FSH or hMG . Stokman PG , de Leeuw R , van den Wijngaard HA , Kloosterboer HJ , Vemer HM , Sanders AL . Human chorionic gonadotropin in commercial human menopausal gonadotropin preparations . Fertil Steril ;60:175–178 Sullivan MW , Stewart-Akers A , Krasnow JS , Berga SL , Zeleznik AJ . Ovarian responses in women to recombinant follicle-stimulating hormone and luteinizing hormone (LH) (a role for LH in the final stages of follicular maturation) . J Clin Endocrinol Metab ;84:228–232
. hCG alone (200 IU/d), corresponding to roughly 1,200 IU/d of LH. The hCG is also drastically less expensive than recombinant FSH or hMG . Stokman PG , de Leeuw R , van den Wijngaard HA , Kloosterboer HJ , Vemer HM , Sanders AL . Human chorionic gonadotropin in commercial human menopausal gonadotropin preparations . Fertil Steril ;60:175–178. Sullivan MW , Stewart-Akers A , Krasnow JS , Berga SL , Zeleznik AJ . Ovarian responses in women to recombinant follicle-stimulating hormone and luteinizing hormone (LH) (a role for LH in the final stages of follicular maturation) . J Clin Endocrinol Metab ;84:228–232.")
111
HCG low-dose in long protocol
Gn-RH-a long protocol r-FSH/hMG (1:1/2) IU on 2° day at least six follicles >12 mm and E2 >300 pg/ml hCG 250 IU/day alone until the end of COH or variable amounts of r-FSH and low-dose (10-50) IU hCG reduced r-FSH/hMG consumption outcome comparable to traditional COH regimens; reduced number of small preovulatory follicles; did not cause premature luteinization; more estrogenic intrafollicular environment 12 Filicori M: Fertil Steril 2005: 84, 2:
 IU on 2° day at least six follicles >12 mm and E2 >300 pg/ml. hCG 250 IU/day alone until the end of COH. or. variable amounts of r-FSH and low-dose (10-50) IU hCG. reduced r-FSH/hMG consumption. outcome comparable to traditional COH regimens; reduced number of small preovulatory follicles; did not cause premature luteinization; more estrogenic intrafollicular environment. 12. Filicori M: Fertil Steril 2005: 84, 2:")
112
gonadotropin and steroid at HCG day
12 gonadotropin and steroid at HCG day Group A Group B P value (no hCG) (hCG) LH (IU/L) ± ± NS FSH (IU/L) 11.3± ± <.001 hCG (IU/L) 0.4± ± <.001 E2 (pg/mL) ± ± <.05 P (ng/mL) 1.1± ± NS T (ng/mL) ± ± <.05 Filicori M: Fertil Steril 2005: 84, 2:
 (hCG) LH (IU/L) 0.6± ±0.3 NS. FSH (IU/L) 11.3± ±0.6 <.001. hCG (IU/L) 0.4± ±0.5 <.001. E2 (pg/mL) 2.358± ±317 <.05. P (ng/mL) 1.1± ±0.1 NS. T (ng/mL) 0.9± ±0.1 <.05. Filicori M: Fertil Steril 2005: 84, 2:")
113
12 Clinical outcome no-HCG HCG COH days 11.6±0.2 11.9±0.1 NS
r-FSH/hMG days 8.6±0.1 <.001 Daily hCG duration (days) — 3.3±0.1 r-FSH/hMG dose (IU) 2,779±160 1,960±99 Immature oocytes (n) 1.4±0.2 1.6±0.3 Mature oocytes (n) 8.0±0.7 8.2±0.6 Fertilization rate (%) 48±4% (0–100) 74±3% (36–100) Good quality embryos (%) 86±6% 84±5% Embryos transferred (n) 2.3±0.2 2.5±0.1 Implantation rates (%) 11% 12% Pregnancy rates (%) 21% 25% 12 Filicori M: Fertil Steril 2005: 84, 2:
 — 3.3±0.1. r-FSH/hMG dose (IU) 2,779±160. 1,960±99. Immature oocytes (n) 1.4± ±0.3. Mature oocytes (n) 8.0± ±0.6. Fertilization rate (%) 48±4% (0–100) 74±3% (36–100) Good quality embryos (%) 86±6% 84±5% Embryos transferred (n) 2.3± ±0.1. Implantation rates (%) 11% 12% Pregnancy rates (%) 21% 25% 12. Filicori M: Fertil Steril 2005: 84, 2:")
114
13 FSH/HMG long protocol Gn-RH-a depot on 21° day of previous cycle only or Gn-RH-a low dose on 21° day up HCG day r-FSH UI, step-down regimen, on 2nd at 8th cycle day 8 r-FSH continued until HCG day (if LH ≥5 mUI/ml) or HMG on 9th until HCG day (if LH < 1 mUI/ml) Ye H: Fertil Steril 2006;86,3S:S420-S421
 or. HMG on 9th until HCG day (if LH < 1 mUI/ml) Ye H: Fertil Steril 2006;86,3S:S420-S421.")
115
r-FSH/HMG Long protocol
13 1 2 3 4 5 6 7 8 9 10 11 12 LH >5 mIU/ml LH <1 mIU/ml r-FSH HMG Gn-RH-a low dose 21° Gn-RH-a depot or low dose long protocol

116
r-FSH/HMG Long protocol
13 Normal LH Low LH r-FSH r- & HMG Oocytes MII 14 12 13 10 Oocyt fert 10.5 8.8 9.9 7.2 Embryos 2.4 1.5 1.9 1.3 Implant % 35.8% 31.4% 40.7% 32.3% Pregn rate 55.2% 43.8% 61.7% 54.1% miscarriage 7.1% 18.9% 3.0%

117
Antagonists (1990s) They bind immediately to the receptor
Receptor target this leads to immediate pituitary down-regulation and do not activate classic postreceptor events; no “flare-up” *Orgalutran, Cetrotide 0.25 mg fl s.c

118
Gn-RH Antagonists Lubecca Method, delayed somministration 0.25 mg s.c. on 6° COH day or leading follicle >14 mm until HCG day California method early administration (very high-responders) On 1° COH day until leading follicle ≥18 mm and at least two follicles ≥ 15 mm Ovulation triggering with Gn-RH-a long-acting
 On 1° COH day until leading follicle ≥18 mm and at least two follicles ≥ 15 mm. Ovulation triggering with Gn-RH-a long-acting.")
119
on 1° days Gn stimulation on 5°-6° days on leading follicle ≥14 mm
Antagonists protocol on 1° days Gn stimulation on 5°-6° days on leading follicle ≥14 mm HMG or r-FSH + LH added Fixed and early start of the antagonist is probably more effective than an individualized and late start.

120
Gn-RH Antagonist disavantages LDP advantages: peak E2 on HCG day
mature follicles oocytes embryos PR advantages: Prevention surge LH larger cohort of follicles Avoidance of adverse effects of agonists More friendly stimulation protocol OHSS

122
LH added The early follicular phase is characterized by the presence of LH receptors on theca cells and the presence of FSH receptors on granulosa cells, with a prevalence of FSH activity. The middle-late follicular phase is characterized by the presence of LH receptors on both theca and granulosa cells, with a prevalence of LH activity and declining FSH levels. This leads to a selection of the dominant follicle and monofollicular ovulation. . Filicori M. Use of luteinizing hormone in the treatment of infertility: time for reassessment? Fertil Steril 20003;79:253–5.

123
LH added Granulosa cells in ovarian follicles of larger size (>10–12 mm) normally express the LH/hCG receptor and become sensitive to LH activity stimulation * Campbell et al. showed that pulsatile LH administration in sheep maintained elevated ovulatory rates despite FSH withdrawal ** LH/hCG receptors may also be highly relevant to permit continued dominant follicle growth in the spontaneous mid-late follicular phase, at a time when the physiologic serum FSH decline * * * Zeleznik AJ , Hillier SG .: Clin Obstet Gynecol ;27:927–940 * * Campbell BK , Dobson H , Baird DT , Scaramuzzi RJ .: J Reprod Fertil ;117:355–367
 normally express the LH/hCG receptor and become sensitive to LH activity stimulation * Campbell et al. showed that pulsatile LH administration in sheep maintained elevated ovulatory rates despite FSH withdrawal ** LH/hCG receptors may also be highly relevant to permit continued dominant follicle growth in the spontaneous mid-late follicular phase, at a time when the physiologic serum FSH decline * * * Zeleznik AJ , Hillier SG .: Clin Obstet Gynecol ;27:927–940. * * Campbell BK , Dobson H , Baird DT , Scaramuzzi RJ .: J Reprod Fertil ;117:355–367.")
124
LH ADDED target LH <1 UI/ml at the start of Gn stimulation
Gn-RH-a flare protocol (LH suppression) Gn-RH antagonist during stimulation >35 years Poor responders High responders (LH prevalence activity decrease n. small follicles and OHSS risk)
 Gn-RH antagonist during stimulation. >35 years. Poor responders. High responders (LH prevalence activity decrease n. small follicles and OHSS risk)")
125
LH added target

126
LH added target the early follicular phase is characterized by the presence of LH receptors on theca cells and FSH receptors on granulosa cells, with a prevalence of FSH activity. The middle-late follicular phase is characterized by the presence of LH receptors on both teca and granulosa cells, with a prevalence of LH activity and declining FSH levels* * Filicori 2003

127
Prevalence activity of
LH added target Cycle’s phase FSH rec LH rec Prevalence activity of early follicolar + + + (G) + (T) FSH late follicolar + + (G) + + + (T&G) LH luteal - - + + + (CL)
 + (T) FSH. late follicolar. + + (G) (T&G) LH. luteal (CL)")
128
LH added target FSH: earlier cycle follicular phase:
follicles recruitment Follicles growth LH: late cycle follicular phase: mature oocytes Ovulation LH: Luteal cycle phase: corpus luteum, LDP * Filicori 2003

129
Rationale for LH added (Sullivan 1999)
The rationale for this hypothesis is that the FSH-stimulated induction of LH receptors on granulosa cells could enable the maturing follicle to respond to LH and thereby continue to mature in the presence of continuously declining FSH concentrations

130
Rationale for LH added (Sullivan 1999)
It is generally accepted that E2 production by the maturing follicle occurs by way of the two-cell, two-gonadotropin model. In this model, theca cells produce androstenedione and testosterone under LH stimulation, and FSH induces granulosa cell aromatase, thus enabling the thecally derived androgens to be metabolized to E2. Assuming the validity of this model in humans, our results indicate that thecal androgen production is exquisitely sensitive to LH, as a plasma LH concentration of 1.5 IU/L was sufficient to maintain E2 production as well as plasma androstenedione concentrations. Our observation of E2 production despite very low serum LH concentrations is in agreement with other published data showing that women treated with GnRH agonists to suppress gonadotropin secretion maintain E2 production in the presence of very low levels of serum LH (<0.5 IU/L). Our current study also indicates that although LH concentrations of approximately 1.5 IU/L are able to sustain thecal androgen production, these levels of LH are unable to maintain granulosa cell aromatase activity when FSH concentrations decline. (vedi iperandrogenismo in PCOS)
. Our current study also indicates that although LH concentrations of approximately 1.5 IU/L are able to sustain thecal androgen production, these levels of LH are unable to maintain granulosa cell aromatase activity when FSH concentrations decline. (vedi iperandrogenismo in PCOS)")
131
LH Added protocol 15 leuprolide acetate 1 mg daily, sc, from menstrual day 21 for 14 days (+ 7 days) excluded from further treatment if E2 >20 pg/ml and/or LH >2,5 IU after 21 days leuprolide LH <2.5 IU/L and E2 <20 pg/mL r-FSH starting at 150 IU sc daily at h. for 4 days On 5° day If serum E2 levels were less than 100 pg/mL, the r-FSH dose was increased to 225 IU If serum E2 levels were greather than 100pg/mL, the r-FSH was maintained at 150 IU/day r-LH 375 IU twice a day (7.30 and h) for the last 2 days of COH or Leading follicle ≥14 mm *Sullivan MW et al: “Ovarian Responses in Women to Recombinant Follicle-Stimulating Hormone and Luteinizing Hormone (LH): A Role for LH in the Final Stages of Follicular Maturation” J Clin Endocrinol Metab ;84:228–232 .
 for the last 2 days of COH. or. Leading follicle ≥14 mm. *Sullivan MW et al: Ovarian Responses in Women to Recombinant Follicle-Stimulating Hormone and Luteinizing Hormone (LH): A Role for LH in the Final Stages of Follicular Maturation J Clin Endocrinol Metab ;84:228–232 .")
132
LH added vs. HMG in over 38 * r-FSH + HMG 75 UI (group I) and r-FSH + r-LH 75 UI (group II) HMG group LH group n. follicles on 6 day 6.72 2.22 5.87 1.29 COH days 10.5 1.7 12 1.8 M II oocytes 75.3% 93.1% Pregnancy rate 26% 47% * Gomez-Palomares J. L. ; Acevedo-Martin B. ; Andres L. ; Ricciarelli E. ; Hernandez E. R.; Reproductive biomedicine online ISSN ; 2008

134
Luteal supplementation in agonists/antagonists protocols
Pituitary depletion Pituitary desensitization Negative estrogen feed-back Compulsory supplementation E/P HCG supplementation absolutely necessary !!!

135
P4 secretion Follicular phase Luteal phase * Ovary 48% 95%
Adrenal gland 4% from pregnenolone 1% *P4 serum level: 4 ng/ml is low level; 40 ng/ml is high

136
luteal P4 supplementation
Few studies in the last 20 years Currently, no reliable method for specific diagnosis of P4 deficiency in luteal phase Regimens often determined by clinical experience The rationale for P4 supplementation: Aspiration of the granulosa cells Presence of high levels of E2 Analogues poor luteal function (due to residual suppression of pituitary LH secretion) ASRM Practice Committee: “Exogenous progesterone supplementation” Fertil Steril 2008;89,4:
 ASRM Practice Committee: Exogenous progesterone supplementation Fertil Steril 2008;89,4:")
137
luteal P4 supplementation
P4 50 mg/d i.m. Or mg/day vaginally Starting: 3 days after IUI or at E-T day Prontogest fl im 100 mg

138
luteal P4 supplementation
Higher pregnancy rate * Lack of evidence in literature * * Increased of hypospadias (progestins derived from androgens and that bind to androgen receptors) * * * * Yovich JL et al: “Early luteal serum progestyerone concentration are higher in pregnancy cycles”. Fertil Steril 1985;44: ** Ziad R. Hubayter: “luteal supplementation in in vitro fertilization: more question than answers”. Fertil Steril 2008; 89,4: ***ASRM Practice Committee: “Exogenous progesterone supplementation” Fertil Steril 2008;89,4: Carmichael SL et al: “Maternal progestin intake and risk of hypospadias”. Arch Pediatr Adolesc Med 2005;159:957
 * * * * Yovich JL et al: Early luteal serum progestyerone concentration are higher in pregnancy cycles . Fertil Steril 1985;44: ** Ziad R. Hubayter: luteal supplementation in in vitro fertilization: more question than answers . Fertil Steril 2008; 89,4: ***ASRM Practice Committee: Exogenous progesterone supplementation Fertil Steril 2008;89,4: Carmichael SL et al: Maternal progestin intake and risk of hypospadias . Arch Pediatr Adolesc Med 2005;159:957.")
139
P4 Orally: bioavailabilty diminished by the liver first pass the serum level typically returns to baseline level by 6 hours dizziness and somnolence fatigue, headache, urinary frequency vaginal route: the level remains elevated for up 48 hours Crinone gel 8% once a day and contains 90 mg of P4 Progeffik gel 200 mg 1-3/day Uterine tissue higher level P4 despite a lower serum P4 Vaginal irritation Intramuscular: P4 in oil result in higher plasma concentration and longer duration * Severe allergic reaction Adult respiratory distress syndrome Eosinophilic pneumonitis *Posaci C, Smitz J, Camus M, Osmanagaoglu K, Devroey P: “Progesterone for the luteal support of ART: clinical options”. Human Reprod 2000; 15,S1:

140
luteal supplementation in agonist/antagonist protocols
Pituitary desensitization for 2-3 w after last administration Worldwide standard practice * * Belaisch-Allart J et al: “ JL et al: “The effect of HCG supplementation after combined Gn-RH agonist/HMG treatment in an IVF programme”. Human Reprod 1990;5:

141
luteal suppl agonist/antagonist protocols
or/and HCG : more effective Increased production of E2 and P4 Better endocrine profile No differences in pregnancy outcome OHSS risk (E2 peak at HCG day) *Martinez F: “ Human Corionic Gonadotropin and intravaginal natural progesterone are equally effective for luteal phase support in IVF”. Gynecol Endocrinol 2000; 14:
 *Martinez F: Human Corionic Gonadotropin and intravaginal natural progesterone are equally effective for luteal phase support in IVF . Gynecol Endocrinol 2000; 14:")
142
Luteal E2 supplementation
In IVF cycles, the levels of E2 and P4 drop in the mid-late luteal phase Lower E2 at 11 days after pick-up is associated with lower pregnancy rate E2 orally 2-6 mg/d (Progynova cpr 2 mg) * Start on: E-T day or 7 days after E-T Increases implantation rate Increases pregnancy rate * Lukaszuk K: Fertil Steril 2005;83:
 * Start on: E-T day. or. 7 days after E-T. Increases implantation rate. Increases pregnancy rate. * Lukaszuk K: Fertil Steril 2005;83:")
143
PROTOCOLS: 6 9 10 11 16-27

144
Poor response — the devil is in the definition
The original definition of low response to ovarian response by Garcia et Acosta was based on low peak E2 concentrations alone They stimulated patients with hMG (150 IU IM daily) and defined low responders as patients with a peak E2 concentration of <300 pg/mL
 and defined low responders as patients with a peak E2 concentration of <300 pg/mL.")
145
Poor responders diminished ovarian reserve
A lower expression of FSH receptor in the granulosa cells Advanced maternal age E2 < 500 pg/mL on day of hCG <4 de Graaf follicles on HCG day lower fertilization rates lower cleavage rates lower resulting embryos Lower implantation rate lower pregnancy rates “occult ovarian failure” 10–25% of the ART population* * Keay et al., 1997 ; Karande and Gleicher, 1999 ; Fasouliotis et al., 2000 ; Tarlatzis et al., 2003

146
increase Gn dose 16 first and simplest approach
limited benefit to 450 IU per day 300 IU r-FSH + hMG 150 IU beyond this amount little or no improvement Murat Arslan: Fertil Steril 2005; 84,3:

147
the stop Gn-RH-a protocol
17 Gn-RH-a low dose on 21° day until the beginning of menstruation. Stop analogues gonadotropins from day 2 of the cycle until HCG day Target of this protocol: Stop to pre-menstrual FSH and, subsequently, stop to size discrepancy in the developing follicles

148
18 CC + HMG + Antagonist CC 150 mg/d on 1°-5° days
HMG (r-FSH) large dosage ( IU/d) on 2-3° cycle day Antagonist delayed administration: on 6°-8° stimulation days or leader follicle ≥ 14 mm if very few follicles CG HCG UI on day dominant follicle ≥18 mm Luteal supplementation: HCG IU/d (+ P4)
 large dosage ( IU/d) on 2-3° cycle day. Antagonist delayed administration: on 6°-8° stimulation days. or leader follicle ≥ 14 mm if very few follicles. CG. HCG UI on day dominant follicle ≥18 mm. Luteal supplementation: HCG IU/d (+ P4)")
149
E-P Antagonist protocol
19 Farmakon Dosage Time length E-P pill previous cycle 14-21 days FSH/HMG 2° cycle d up HCG d CC 150 mg/d 1° cycle d 5-7 days Antagon 0.25 mg/d 7-8° d HCG IU >18 mm

150
CC + HMG + Antagonist Long protocol n° ampules 50 83 follicles >14
Age >40 Long protocol CC + HMG + Antagonist n° ampules 50 83 follicles >14 3.7 5.8 E2 on day 5 36 74 E2 on day 9 169 945 ( ) E2 on HCG day 744 833 ( ) Cancellation rate 34% 4.8% total oocytes 3.3 5.5 Mature oocytes 2.6 4.29 n° embryo 1.4 1.6 PR 15.3% 22.2% Implant rate 7.6% 13.5% Weghofer, 2004
 E2 on HCG day ( ) Cancellation rate. 34% 4.8% total oocytes Mature oocytes n° embryo PR. 15.3% 22.2% Implant rate. 7.6% 13.5% Weghofer,")
151
Luteal estradiol protocol
20 lowering FSH levels with estrogen, the ovary will respond when high doses of FSH are added in COH protocol Oral micronized E2 2 mg twice a day On luteal day 21 At 3 days of COH r-FSH IU/d down regimen on 2° day microdose flare Gn-RH-a on 3° COH day or delayed Gn-RH antagonist HCG low-dose (10-50 IU/d) on 8° day Dragisic KG Fertil Steril 2005;84:
 on 8° day. Dragisic KG Fertil Steril 2005;84:")
152
Luteal estradiol protocol *
outcome All cycles Luteal Estradiol Standard protocol Clinical Pr 38,3% 40,9% 31,3% Miscarriage rate 43,5% 38,9% 60,0% Delivery rate 20.0% 25.0% 12.5% * Frattarelli J, et al: “A luteal estradiol protocol for expected poor-responders improves embryo number and quality” Fertil Steril 2008;89,5:

153
AACEP Protocol E-P pills for 1 to 3 weeks
Gn-RH-a low-dose in a standard long protocol overlapping the last 5 to 7 days of E-P pills until onset of menses Gn-Rh antagonist low-dose (0.125 mg/day) on cycle day 2 Estradiol valerate* 2 mg/d on 1° to 10° cycle day Estrogen suppositories** were used to maintain the endometrium until at last one follicle measured 15 mm r-FSH in initial doses of 600 or 750 IU/day, decreasing to 225 IU/day of r-FSH. * Progynova cpr 2 mg ** Vagifem cpr vaginali mg Fisch JD, Keskintepe L and Sher G: “Gonadotropin-releasing hormone agonist/antagonist conversion with estrogen priming in low responders with prior in vitro fertilization failure”. Fertil Steril 2008;89,2:
 on cycle day 2. Estradiol valerate* 2 mg/d on 1° to 10° cycle day. Estrogen suppositories** were used to maintain the endometrium until at last one follicle measured 15 mm. r-FSH in initial doses of 600 or 750 IU/day, decreasing to 225 IU/day of r-FSH. * Progynova cpr 2 mg. ** Vagifem cpr vaginali mg. Fisch JD, Keskintepe L and Sher G: Gonadotropin-releasing hormone agonist/antagonist conversion with estrogen priming in low responders with prior in vitro fertilization failure . Fertil Steril 2008;89,2:")
154
* AACEP Protocol a g o n i t E-P p I l s E T A E
1 2 3 4 5 6 7 8 9 10 12 13 14 15 16 17 … E T P4 A E HCG r-FSH 150 IU A antagonist

155
22 Androgens androgens may influence the responsiveness of ovaries to gonadotrophins positive regulators of follicular development augments follicular FSH-receptor expression in granulosa cells IGF-I oocyte expression promotes initiation of primordial follicle growth increases the number of growing preantral and small antral follicles Vendola K, Zhou J, Wang J, Famuyiwa OA, Bievre M, Bondy CA. Androgens promote oocyte insulin-like growth factor I expression and initiation of follicle development in the primate ovary. Biol Reprod 1999; 61:353–357.

156
Androgens T DHT DHEA Letrolozole

157
DHEA DHEA is the cornerstone to all sex hormones
For women under 50, DHEA levels of less than 150 ng/dL are considered low Casson PR: “Dehydroepiandrosterone supplementation augments ovarian stimulation in poor responders: a case series Human” Reproduction, Vol. 15, No. 10, , October 2000

158
DHEA protocol and during COH POF High FSH
75 mg/d for 4-12 months previous COH and during COH Reduces FSH level release more and better quality eggs prior to IVF reduces miscarriage rates - especially in older women similar effects of GH increasing IGF-I paracrine effects Increases IGF-I serum levels Leonidas Mamas, Eudoxia Mamas,: “Premature ovarian failure and dehydroepiandrosterone” Fertil Steril 2008 in press

159
Testosterone Two IVF treatment cycle cancellations due to poor follicular response, in spite of vigorous gonadotrophin ovarian stimulation and having normal basal FSH levels Balasch J, Fábregues F, Peñarrubia J, Carmona F, Casamitjana R, Creus M, Manau D, Casals G and Vanrell JA: “Pretreatment with transdermal testosterone may improve ovarian response to gonadotrophins in poor-responder IVF patients with normal basal concentrations of FSH”. Human Reproduction (7):
:")
160
Testosterone protocol
Gn-RH-a low dose (Leuprolide 1 mg or triptoreline 0.1 mg) long protocol-like started in the midluteal phase of the previous cycle at menses start Gn-RH-a is reduced to 0.5 mg and continued until the administration of HCG 1° cycle Gn-RH-a 0.5 mg/day of leuprolide from the midluteal phase at menses start 0.25 mg/day thereafter 2° cycle Balasch J, Fábregues F, Peñarrubia J, Carmona F, Casamitjana R, Creus M, Manau D, Casals G and Vanrell JA: “Pretreatment with transdermal testosterone may improve ovarian response to gonadotrophins in poor-responder IVF patients with normal basal concentrations of FSH”. Human Reproduction (7):
 long protocol-like started in the midluteal phase of the previous cycle. at menses start Gn-RH-a is reduced to 0.5 mg and continued until the administration of HCG. 1° cycle. Gn-RH-a 0.5 mg/day of leuprolide from the midluteal phase at menses start mg/day thereafter. 2° cycle. Balasch J, Fábregues F, Peñarrubia J, Carmona F, Casamitjana R, Creus M, Manau D, Casals G and Vanrell JA: Pretreatment with transdermal testosterone may improve ovarian response to gonadotrophins in poor-responder IVF patients with normal basal concentrations of FSH . Human Reproduction (7):")
161
Testosterone transdermal testosterone 20 µg/kg per day
Androderm 2.5 mg daily single patch Removed always at 9.00 a.m. 0.1 mg/h delivery rate (a predetermined number of hours provides the desired daily dose of testosterone [e.g. in a woman weighing 60 kg and needing 1200 µg/day, the patch was used for 12 h (0.1 mg/h delivery rate x 12 h = 1.2 mg or 1200 µg) and thus applied at hours]. during the 5 days preceding COH Balasch J, Fábregues F, Peñarrubia J, Carmona F, Casamitjana R, Creus M, Manau D, Casals G and Vanrell JA: “Pretreatment with transdermal testosterone may improve ovarian response to gonadotrophins in poor-responder IVF patients with normal basal concentrations of FSH”. Human Reproduction (7):
 and thus applied at hours]. during the 5 days preceding COH. Balasch J, Fábregues F, Peñarrubia J, Carmona F, Casamitjana R, Creus M, Manau D, Casals G and Vanrell JA: Pretreatment with transdermal testosterone may improve ovarian response to gonadotrophins in poor-responder IVF patients with normal basal concentrations of FSH . Human Reproduction (7):")
162
Testosterone COH 1° cycle 2° cycle
Gonadotrophin ovarian stimulation was started the day following last testosterone patch application 1° cycle On day 1 of ovarian stimulation, r-FSH 450 IU s.c. On day 2 r-FSH 300 IU On days 3 and 4 of ovarian stimulation, 150 IU per day From day 5 onwards, r-FSH was administered on an individual basis 2° cycle On days 1 and 2 of ovarian stimulation, r-FSH 300 IU per day + HMG 300 IU i.m. On days 3 and 4 of ovarian stimulation, 300 IU HMG From day 5 onwards, HMG on an individual basis Balasch J, Fábregues F, Peñarrubia J, Carmona F, Casamitjana R, Creus M, Manau D, Casals G and Vanrell JA: “Pretreatment with transdermal testosterone may improve ovarian response to gonadotrophins in poor-responder IVF patients with normal basal concentrations of FSH”. Human Reproduction (7):
:")
164
Testosterone 80% showed an increase of over fivefold in the number of recruited follicles, produced 5.8 ± 0.4 oocytes, received two or three embryos pregnancy rate: 30% per oocyte retrieval cancelled cycles: 20% Balasch J, Fábregues F, Peñarrubia J, Carmona F, Casamitjana R, Creus M, Manau D, Casals G and Vanrell JA: “Pretreatment with transdermal testosterone may improve ovarian response to gonadotrophins in poor-responder IVF patients with normal basal concentrations of FSH”. Human Reproduction (7):
:")
166
Letrozole A E1 T E2 Third-generation aromatase inhibitors (AIs)
nonsteroidal, reversible, orally administered The excellent oral bioavailability (100%) relatively short half-life (45 hours) able to effectively block the conversion of : A E1 T E2
 relatively short half-life (45 hours) able to effectively block the conversion of : A E1. T E2.")
167
Letrozole + HMG CC resistant Poor responders
20%–25% of women are resistant to CC comparable pregnancy results vs.: CC/HMG r-FSH alone significant saving in the amount of Gonadotropins Grabia A, Papier S, Pesce R, Mlayes L, Kopelman S, Sueldo C: “Preliminary experience with a low-cost stimulation protocol that includes letrozole and human menopausal gonadotropins in normal responders for assisted reproductive technologies” Fertil Steril 2006;86,4:

168
Letrozolo + HMG Letrozolo 2.5 mg days 3–7 day cycle
HMG 150 IU on day 5 up lead. foll. >18 HCG IU hours after Pick-up hours after HCG P4 50 mg/d i.m. on HCG day or E-T day Mohamed F.M Mitwally, Robert F Casper: “Use of an aromatase inhibitor for induction of ovulation in patients with an inadequate response to clomiphene citrate” Fertil Steril 2001; 75,2:

169
Increasing AA Poor responders: lower expression of FSH receptor in the granulosa cells PCOs Patients: hyperexpression of FSH receptor

170
Increasing AA inducing a temporary and reversible PCO-like condition in the ovaries of poor responder patients could enhance their follicular recruitment and development

171
Aromatase inhibitors protocol
aromatase inhibitor which induces a temporary accumulation of intraovarian androgens ADVANTAGES AIs vs. CC Lack of down-regulation of hypothalamic-pituitary estrogen receptors Lower FSH dose Higher number of mature oocytes Less adverse effects on endometrium1 and cervix Pregnacy rate: 21% 1 Endometrial thickness <5 mm is usually associated with failure to conceive (Gonen Yand Casper RF: “Sonografic determination of an adverse effect of clomiphene citrate on endometrial growth”. Human Reprod 1990;5: ).
.")
172
Increasing AA synergistical role of androgens with FSH to promote early follicular recruitment trophic effects of androgens in small antral follicles Positive estrogen feed-back on hypotalamic-hypophyseal axis AA too high reduce follicular health

173
Letrozole E-P for 15-21 days or E2 <60 pg/ml
absence of cysts >10 mm letrozole, 2.5 mg/day from day 1-5 of the menstrual cycle FSH ( IU/day) starting on day 6 hCG (10,000 IU) when two leading follicles were ≥20 mm Mitwally MFM and Casper RF. (2002) Aromatase inhibition improves ovarian response to follicle-stimulating hormone in poor responders. Fertil Steril 77:776–780.
 starting on day 6. hCG (10,000 IU) when two leading follicles were ≥20 mm. Mitwally MFM and Casper RF. (2002) Aromatase inhibition improves ovarian response to follicle-stimulating hormone in poor responders. Fertil Steril 77:776–780.")
174
Letrozole + Antagonist
letrozolo 5 mg on 1° to 5° cycle day r-FSH 300 IU + HMG 150 IU on 1° to 5° cycle day On 6° day individual dosages r-FSH/HMG delayed antagonist 0.25 mg/d HMG + Antagonist until HCG day r-HCG 250 mg on leading follicle >18 mm P4 supplementation with 200 mg of vaginal micronized P (Progeffik) Garcia-Velasco JA. ,Moreno L, Pacheco A, Guillén A, Duque L, Requena A, Pellicer A: “The aromatase inhibitor letrozole increases the concentration of intraovarian androgens and improves in vitro fertilization outcome in low responder patients: A pilot study”. Fertil Steril 2005;84,1:82-87.
 Garcia-Velasco JA. ,Moreno L, Pacheco A, Guillén A, Duque L, Requena A, Pellicer A: The aromatase inhibitor letrozole increases the concentration of intraovarian androgens and improves in vitro fertilization outcome in low responder patients: A pilot study . Fertil Steril 2005;84,1:")
175
A Antagon E T A r-FSH 150 IU HMG 150 UI
2 3 4 5 6 7 8 9 10 12 13 14 15 16 17 18 19 … E T P4 A r-FSH 150 IU HMG 150 UI Letrozole 2,5 mg r-HCG 250 mg A Antagon

176
Letrozole + Antagonist
control oocytes retrieved 6.1 ± 0.4 4.3 ± 0.3 Fertilization rate 68,2 % 63,3 % embryos transferred 2 ± 0.1 2.3 ± 0.1 PR/cycle 22.4 % 15.2 % PR/transfer 41.7 % 28.9 % Implantation rate 25 % 9.4 % Miscarriage rate 20 % 7.7 % twins 46.7% 7.7% Garcia-Velasco. Letrozole in poor responder JVF patients. Fertil Steril 2005

177
Assisted hatching a b c M. Carrino, M. Wilding, E. Tosti, V. Volpicelli, B. Dale: “Zona Binding” e “Zona Penetration” come tests predittivi dell’infertlità maschile; Atti “IV GIORNATE ANDROLOGICHE ITALIANE”; Perugia, settembre 1998.

178
E-T on the day 2 Microdose flare agonist protocol day 2 day 3
Implantation rate 23.9% 17.2% Pregn rate/oocyte 27.7% 16.2% Pregnancy rate/E-T 29.0 18.3 Luteal supplementation: progesterone 100 mg/day i.m. On oocyte collection through the luteal phase Bahceci M.: Fertil Steril 2006;86,1:81-85

179
Ovary deficiency 1) gonadic disgenesia
“streak gonad” absence of ovary tissue 2) Ovary disgenesia Ovary tissue without follicles and without functionality 3) POF Ovary tissue without follicles but with past functionality 4) Proof Ovary (Savage Symdrome) Ovary tissue with hystologic normal follicles
 Ovary. disgenesia. Ovary tissue without follicles and without functionality. 3) POF. Ovary tissue without follicles but with past functionality. 4) Proof Ovary (Savage Symdrome) Ovary tissue with hystologic normal follicles.")
184
endometriosis

185
adenomiosis

186
endometriosis

187
endometriosis presence of ovarian endometriomas
responsiveness to gonadotropins: - 25%

188
Long protocol + prednisone
3.75 mg Gn-Rh-a depot in one dose on 21st day or Low-dose daily on the 21st day of previous cicle to HCG day on any when LH <0.5 and E2 <30 on the 3th day of menstrual cycle USG LH <0.5 UI/ml E2 <30 pg/ml

189
Long protocol + prednisone
Prednisone 15 mg/day on 1° day at HCG day (Deltacortene cpr 5 mg) r-FSH 450 IU on 2° day up 6° day r-FSH variable dosage Luteal supplementation: P4 50 mg/d i.m.
 r-FSH 450 IU on 2° day up 6° day. r-FSH variable dosage. Luteal supplementation: P4 50 mg/d i.m.")
190
lean women reproductive performance was not poorer
Donna magra come un treno (Mango) reproductive performance was not poorer “inverted U shape theory” applies only to native oocyte conceptions. Levens ED, Skarulis MC: “Assessing the role of endometrial alteration among obese patients undergoing assisted reproduction”. Fertil Steril 2008;89,6:
 reproductive performance was not poorer. inverted U shape theory applies only to native oocyte conceptions. Levens ED, Skarulis MC: Assessing the role of endometrial alteration among obese patients undergoing assisted reproduction . Fertil Steril 2008;89,6:")
192
Overweight according to body mass index (BMI): lean (<20 kg/m2),
normal (20.0–24.9 kg/m2), overweight (25.0–29.9 kg/m2), obese (≥30 kg/m2). Levens ED, Skarulis MC: “Assessing the role of endometrial alteration among obese patients undergoing assisted reproduction”. Fertil Steril 2008;89,6:
, overweight (25.0–29.9 kg/m2), obese (≥30 kg/m2). Levens ED, Skarulis MC: Assessing the role of endometrial alteration among obese patients undergoing assisted reproduction . Fertil Steril 2008;89,6:")
193
Overweight in PMA Higher cancellation rate Lower pregnancy rates
Poor reproductive performance: Higher cancellation rate Lower pregnancy rates higher miscarriage rates lower live-birth rates in natural and PMA more frequent complications in pregnancy *Fedorcsáck P, Storeng R, Dale PO, Tanbo T, Abyholm T. Obesity is associated with early pregnancy loss after IVF or ICSI. Acta Obstet Gynecol Scand. 2000;79:43–48. * the effect of recipient body weight on reproductive performance

194
Overweight Extraovum effects of obesity on FIVET outcome:
insulin resistance hyperandrogenism elevated leptin levels Norman RJ, Clark AM. Obesity and reproductive disorders: a review. Reprod Fertil Dev. 1998;10:55–63.

195
Overweight Obesity could impair reproduction by acting on: the ovary
and/or the endometrium (unfavorable intrauterine milieu) * 35-50% PCOS are overweight or obese ** Discrepancies in miscarriage rates mainly due to statistical flaws caused by small sample sizes *Beliver J: “Obesity and poor reproductive outcome: the potential role of the endometrium “. Fertil Steril 2007;88: * Levens ED, Skarulis MC: “Assessing the role of endometrial alteration among obese patients undergoing assisted reproduction”. Fertil Steril 2008;89,6: * Loveland JB, McClamrock HD, Malinow AM, Sharara FI. Increased body mass index has a deleterious effect on in vitro fertilization outcome. J Assist Reprod Genet. 2001;18:382–386. * * Gambineri A, Pelusi C, Vicennati V, Pagotto U, Pasquali R. Obesity and polycystic ovary syndrome. Int J Obes Relat Metab Disord. 2002;26:883–896.
 * 35-50% PCOS are overweight or obese ** Discrepancies in miscarriage rates mainly due to statistical flaws caused by small sample sizes. *Beliver J: Obesity and poor reproductive outcome: the potential role of the endometrium . Fertil Steril 2007;88: * Levens ED, Skarulis MC: Assessing the role of endometrial alteration among obese patients undergoing assisted reproduction . Fertil Steril 2008;89,6: * Loveland JB, McClamrock HD, Malinow AM, Sharara FI. Increased body mass index has a deleterious effect on in vitro fertilization outcome. J Assist Reprod Genet. 2001;18:382–386. * * Gambineri A, Pelusi C, Vicennati V, Pagotto U, Pasquali R. Obesity and polycystic ovary syndrome. Int J Obes Relat Metab Disord. 2002;26:883–896.")
196
Figure 1 Ongoing pregnancy rate per cycle (%) in each BMI group. CI: confidence interval (women undergoing ovum donation) * Fedorcsáck P, Storeng R, Dale PO, Tanbo T, Abyholm T. Obesity is associated with early pregnancy loss after IVF or ICSI. Acta Obstet Gynecol Scand. 2000;79:43–48. MEDLINE
 * Fedorcsáck P, Storeng R, Dale PO, Tanbo T, Abyholm T. Obesity is associated with early pregnancy loss after IVF or ICSI. Acta Obstet Gynecol Scand. 2000;79:43–48. MEDLINE.")
197
Overweight low-calorie diet for a short period (4-6 week)
before IVF cycle and during IVF cycle weight loss can improve spontaneous ovulation * Positive correlation between weight loss and ovulation and pregnancy outcome: ** *Norman RJ, Noakes M, Wu R, Davies MJ, Moran L, Wang JX. Improving reproductive performance in overweight/obese women with effective weight management. Hum Reprod Update. 2004;10:267–280. MEDLINE | CrossRef ** Clark AM: Human Reprod 1998; 13:

198
Overweight BMI < 25: Gn-RH-a: Pr 29.9% Gn-RH antagonists: Pr 17.5%
Robinson J: Gn-RH-a vs. Gn-RH antagonist in ovarian stimulation: the influence of BMI on in vitro fertilization outcome”. Fertil Steril 2008;89,2:

199
Stimulation protocol starting with luteal phase leuprolide acetate 1 mg or 0.25 mg Gn-RH-a was decreased to 0.25 or 0.5 mg at the start of gonadotropins and continued daily until the day of hCG R-FSH or HMG on cycle day 2–4 at a dose of IU daily 10,000 IU of hCG on the leading follicle >18 mm II° Protocol Women not undergoing the standard protocol received a modified microdose flare protocol: After at least 21 days of oral contraceptives, 40 μg of Lupron twice daily beginning on the second day of withdrawal bleeding. r-FSH or HMG IU daily on 2 days after Lupron at HCG day Two days before ET, 16 mg of methylprednisolone daily for 5 days. On the day of ET, assisted hatching was performed on all 3- and 4-day embryos through the use of a diluted Tyrodes acid solution. P4 supplementation: 50 mg im or 90 mg vaginally daily Nichols, Jr. BMI extremes and IVF pregnancy rates. Fertil Steril 2003.

200
TABLE 1. Distribution of variables and outcomes by BMI group.
ampules FSH 29.5 (18.7)* 27.8 (13.9) * 30.5 (16.7) * COH days 9.2 (1.3) * 9.0 (1.3) * thickness 10.8 (1.9) * 10.7 (2.2) * 11.6 (2.5) * pregnancy rate 35.6% 52.1% 35.2% abortion 0% 5.9% 4.0% * ± SD Nichols, Jr. BMI extremes and IVF pregnancy rates. Fertil Steril 2003.
* 27.8 (13.9) * 30.5 (16.7) * COH days. 9.2 (1.3) * 9.0 (1.3) * thickness (1.9) * 10.7 (2.2) * 11.6 (2.5) * pregnancy rate. 35.6% 52.1% 35.2% abortion. 0% 5.9% 4.0% * ± SD. Nichols, Jr. BMI extremes and IVF pregnancy rates. Fertil Steril")
202
Low dose aspirin protocol
Patients with autoimmune disorders Suppressed tromboxane A2 but Decreases PG I2 too Improves number mature follicles Improve size follicles Not improve pregnancy rate/ET

203
Low dose aspirin protocol
Start in previous cycle of COH 100 mg/day until pick-up day r-FSH 450 IU/d HCG 20 IU/d Microdose flare on 2° day of COH or Delayed antagonist Frattarelli JL et al: “Low-dose aspirin use does not improve in vitro fertilization outcomes in poor responders”. Fertil Steril 2008;89,5:

205
Ovary hyperstimulation
OHSS physiopathology Ovary hyperstimulation Multiple follicle recruitment Luteal cysts Neovascularisation Massive luteinization histamine prostaglandins citochine renin Ovary enlargement permeability vascular alteration Abdomen distension Abdomen pain Nausea Vomiting Ascites Hypovolemia Oliguria CID

206
OHSS Classification (Volpicelli V. CIC Roma 1998)
SLIGHTY MODERATE SEVERE I° II° III° IV° V° VI° ovary (cm) < 5 5-8 8-11 12-20 > 20 >20 Abdomen distension + ++ +++ ++++ Abdomen pains Peritoneal flogosis Vomiting Nausea Diarrhoea Hydrothorace Ascites [1] Electrolytic Imbalance Hypovolemia Venous central pressure Hypovolemic shock Acidosis Kidney perfusion Oliguria Hyperazotemia [1] Key symptom to hypersevere syndrome
 < > 20. >20. Abdomen distension Abdomen pains. Peritoneal flogosis. Vomiting. Nausea. Diarrhoea. Hydrothorace. Ascites [1] Electrolytic Imbalance. Hypovolemia. Venous central pressure. Hypovolemic shock. Acidosis. Kidney perfusion. Oliguria. Hyperazotemia. [1] Key symptom to hypersevere syndrome.")
207
High responders protocol I
CC 100 mg/d 3°-7° days r-FSH 150 UI s.c. on cycle day 9 at HCG day antagonist 0.25 mg/d delayed regimen Aspirin 100 mg/d on 1° at 45° cycle day HCG UI on leading follicle ≥18 mm

208
High responders protocol II
Gn 225 UI/d on 2° cycle days step-down regimen antagonist 0.25 mg/d on 2° day up HCG day Doxycycline* 80 mg/Kg/day (inhibits vascular leakage) * Folkman HJ: fertil Steril 2007;88,S1:O14 *Bassado cpr 100 mg
 * Folkman HJ: fertil Steril 2007;88,S1:O14. *Bassado cpr 100 mg.")
209
FSH – Antagonist – Agonist + HCG
received triptorelin 0.2 mg in addition to the hCG. The GnRH-a dose was administered at the same time as the hCG; this was devised to achieve the induction of an endogenous LH surge that would coincide with the LH-like 34–36 hours before oocyte retrieval.

210
AA high responders III 0% OHSS
FSH 225 IU/d on the 2° cycle day (step-down regimen) antagonist 0.25 mg/d on the 2° cycle at HCG day Agonist (3.75 mg) as HCG trigger to achieve an endogenous LH surge when E2 ≥ pg/ml (range ) 0% OHSS
 antagonist 0.25 mg/d on the 2° cycle at HCG day. Agonist (3.75 mg) as HCG trigger to achieve an endogenous LH surge. when E2 ≥ pg/ml (range ) 0% OHSS.")
211
Agonist vs. HCG as trigger
Gn-RH-a: HCG UI mature oocytes premature oocytes implantation rate clinical pregnancy ongoing pregnancy OHSS

212
34 OHSS/withholding High responders Young PCOS E2 >4.000 pg/ml
and/or Follicles >10 in each ovary term ≤3 day High responders Young PCOS Yorie Ohata, Tasuku Harada, Masayuki Ito, Souichi Yoshida, Tomio Iwabe, Naoki Terakawa: “Coasting May Reduce the Severity of the Ovarian Hyperstimulation Syndrome in Patients with Polycystic Ovary Syndrome”. Gynecol Obstet Invest 2000;50:

213
34 OHSS/Coasting Until drop of estrogen level <3.000 pg/ml
Coasting >3 days no affects on Pr Egbase PE , Al Sharhan M , Berlingieri P , Grudzinskas JG . Serum oestradiol and progesterone concentrations during prolonged coasting in 15 women at risk of ovarian hyperstimulation syndrome following ovarian stimulation for assisted reproduction treatment . Hum Reprod ;15:2082–2086

214
inverse relationship OHSS/Coasting
duration of coasting/number of mature oocytes retrieved Pregnancy rate M. Aygun, F. Vanlioglu, G. Karlikaya, H. Karagozoglu, B. Kumbak, S. Kahraman: “Coasting may effect endometrial thickness and outcome”. Fertil Steril 2004; 82, S 2, S211 * Ulug U , Ben Shlomo I , Bahceci M . Predictors of success during the coasting period in high-responder patients undergoing controlled ovarian stimulation for assisted conception . Fertil Steril ;82:338–342

215
34 Coasting Gn-RH-a long protocol
HMG or r-FSH 225 IU step-down regimen On 2nd cycle day at HCG or coasting day Coasting HCG IU when E2 <3.000 pg/ml) Owj , E . Tehrani Negad , E . Amirchaghmaghi , Z . Ezabadi , A . Baghestani: “The Evaluation of Withholding Gonadotropins (Coasting) Effects on the Outcome of In-Vitro Fertilization Cycles”. Fertil Steril 2005;84,S254
 Owj , E . Tehrani Negad , E . Amirchaghmaghi , Z . Ezabadi , A . Baghestani: The Evaluation of Withholding Gonadotropins (Coasting) Effects on the Outcome of In-Vitro Fertilization Cycles . Fertil Steril 2005;84,S254.")
216
Ganirelix Orgalutran fl s.c mg

217
“Ganirelix salvage” 35 Gn-RH-a long protocol on late luteal phase previous r-FSH 225 IU/d starting dose (down regimen) Antagonist 0.25 mg daily dose at E2 > 4.000 and or >10 follicles in each ovary daily measurement of serum E2 HCG IU at E2 ≤3.000 pg/ml M . Wittenberger , R . Gustofson , A . Armstrong , J . Segars: “A Cost Comparison of “Ganirelix Salvage” Protocol Versus “Coasting” Strategy for Patients at Risk for Ovarian Hyperstimulation Syndrome (OHSS)” . Fertility and Sterility 2005, 84 ,S318
 . Fertility and Sterility 2005, 84 ,S318.")
218
35 reduce E2 levels (4.219 2.613/24 h) and avoid cycle cancellation
“Ganirelix salvage” reduce E2 levels (4.219 2.613/24 h) and avoid cycle cancellation 24 oocytes mean/cycle 79.2% MII Gustofson RL,, Segars JH and Larsen FW: “Ganirelix acetate causes a rapid reduction in estradiol levels without adversely affecting oocyte maturation in women pretreated with leuprolide acetate who are at risk of ovarian hyperstimulation syndrome”. Human Reproduction (11):
 and avoid cycle cancellation. 24 oocytes mean/cycle. 79.2% MII. Gustofson RL,, Segars JH and Larsen FW: Ganirelix acetate causes a rapid reduction in estradiol levels without adversely affecting oocyte maturation in women pretreated with leuprolide acetate who are at risk of ovarian hyperstimulation syndrome . Human Reproduction (11):")
219
36 PCOS Protocol Pre-treatment with metformin ≥6 months 2.000 mg/day
Improvment in menstrual cyclicity Long-protocol agonist Higher pregnancy outcome F Essah et al Fertil Steril 2006;86,1:

220
IVF cycle cost (ASRM’s average)
total IVF cycle $ 12,500 with “coasting” were $ 400/day the cost per day of “ganirelix salvage” $ 553 cycle cancellation prior to retrieval $ 6379 plus the costs associated with either “coasting” or “ganirelix salvage M.D. Wittenberger, R.L. Gustofson, A. Armstrong, J.H. Segars : “A Cost Comparison of “Ganirelix Salvage” Protocol Versus “Coasting” Strategy for Patients at Risk for Ovarian Hyperstimulation Syndrome (OHSS)”. Fertil Steril 2995; 84,S1:S318
 . Fertil Steril 2995; 84,S1:S318.")
221
OHSS SUPPLEMENTATION * crinone 8% vaginal gel; prometrium cps 100 mg
Micronized progesterone vaginally* mg/d E2 orally** 4 mg/d No HCG ! ! ! * crinone 8% vaginal gel; prometrium cps 100 mg ** progynova cpr 2 mg; sprediol spray 1.5 mg; sandrena gel

223
Natural cycle modification
37 Natural cycle modification when dominant follicle ≥ 14 mm (8°-9° days) r-FSH 75 UI/d up HCG day ± antagonist 0.25 mg/d up HCG day HCG UI (leading follicle ≥18 mm and at least two follicles ≥15 mm) 50 mg/d of im P4 in oil after oocyte retrieval Women aged 40 years FSH elevated Poor responders Cost-saving alternative
 r-FSH 75 UI/d up HCG day. ± antagonist 0.25 mg/d up HCG day. HCG UI (leading follicle ≥18 mm and at least two follicles ≥15 mm) 50 mg/d of im P4 in oil after oocyte retrieval. Women aged 40 years. FSH elevated. Poor responders. Cost-saving alternative.")
224
Luteal supplementation
The luteal phase was supported with 50 mg/d of IM P in oil initiated immediately (?) after oocyte retrieval. Prontogest, AMSA fl i.m. 100 mg
 after oocyte retrieval. Prontogest, AMSA fl i.m. 100 mg.")
225
SUMMARY Controversies on gonadotropins Controversies on analogues
Controversies on E-P pills Controversies on LH added Arslan MA, Bocca S, Mirkin S, Barroso G, Stadtmauer L, Oehninger S: “Controlled ovarian hyperstimulation protocols for in vitro fertilization : two decades of experience after the birth of Elizabeth Carr” Fertil Steril 2005;84,3:

226
higher clinical pregnancy rate with hMG
HMG or r-FSH higher clinical pregnancy rate with hMG but no significant differences in ongoing pregnancy rates or live births Van Wely M , Westergaard L , Bossuyt P , Van Der Veen M . Effectiveness of human menopausal gonadotropin versus recombinant follicle-stimulating hormone for controlled ovarian hyperstimulation in assisted reproductive cycles (a meta-analysis) . Fertil Steril ;80:1086–1093 .
 . Fertil Steril ;80:1086–")
227
intermediate responders
excellent outcome: with either a Gn-RH-a (long protocol) or a GnRH antagonist but tailoring of gonadotropin dose must be performed to achieve optimized results. Arslan MA, Bocca S, Mirkin S, Barroso G, Stadtmauer L, Oehninger S: “Controlled ovarian hyperstimulation protocols for in vitro fertilization : two decades of experience after the birth of Elizabeth Carr” Fertil Steril 2005;84,3:
 or a GnRH antagonist. but tailoring of gonadotropin dose must be performed to achieve optimized results. Arslan MA, Bocca S, Mirkin S, Barroso G, Stadtmauer L, Oehninger S: Controlled ovarian hyperstimulation protocols for in vitro fertilization : two decades of experience after the birth of Elizabeth Carr Fertil Steril 2005;84,3:")
228
High Responders High responders perform favorably with gentler stimulation that minimizes the occurrence of OHSS The number of oocytes retrieved is predictive of clinical pregnancy only in patients over 40 years of age M. Luna-Rojas, B. Sandler, M. Duke, A.B. Copperman, L. Grunfeld, J. Barritt Fertility and Sterility September 2004 (Vol. 82, Page S206)
")
229
Low Responders outcome suboptimal: poor ovarian response
poor oocyte/embryo quality in spite of stimulation regimens used Arslan MA, Bocca S, Mirkin S, Barroso G, Stadtmauer L, Oehninger S: “Controlled ovarian hyperstimulation protocols for in vitro fertilization : two decades of experience after the birth of Elizabeth Carr” Fertil Steril 2005;84,3:

230
LH ADDED Adding LH should be considered in severe situations of LH suppression: use of potent GnRH-agonists Gn-RH-antagonists Over 35 years Suheil J. Muasher, Rony T. Abdallah, Ziad R. Hubayter: “Optimal stimulation protocols for in vitro fertilization” Fertil Steril 2006; 86,2:

231
Conclusion(s) Ovarian stimulation is a critical step in in vitro fertilization therapy. A variety of controlled ovarian hyperstimulation regimens are available and efficacious, but individualization of management is essential and depends on assessment of the ovarian reserve. Identification of the etiologies of poor ovarian response constitutes a formidable challenge facing reproductive endocrinologists. Arslan MA, Bocca S, Mirkin S, Barroso G, Stadtmauer L, Oehninger S: “Controlled ovarian hyperstimulation protocols for in vitro fertilization : two decades of experience after the birth of Elizabeth Carr” Fertil Steril 2005;84,3:

Similar presentations
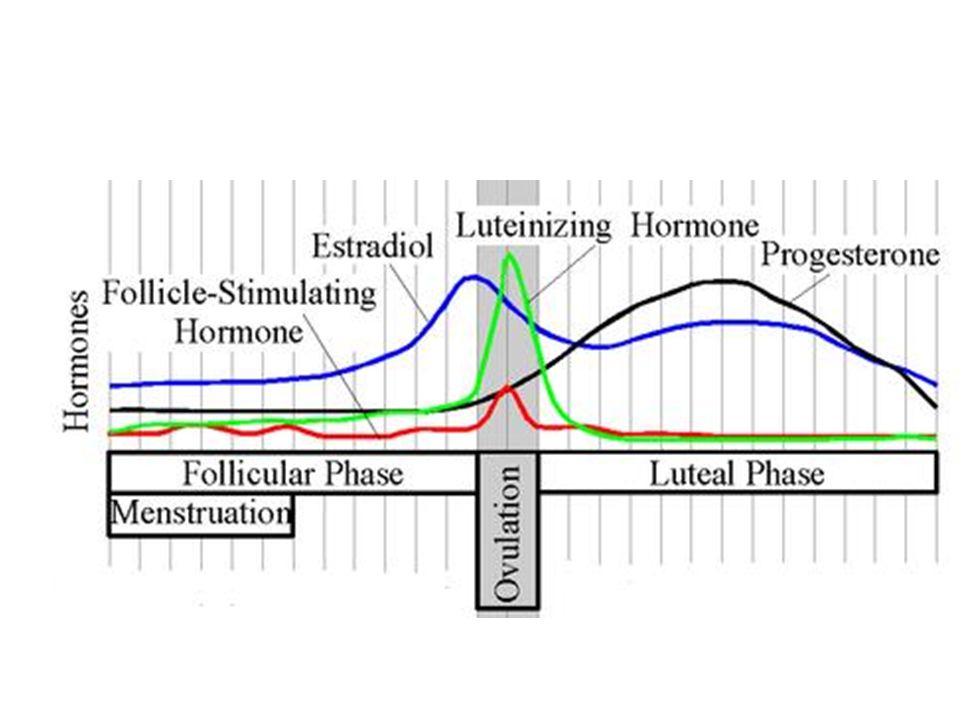
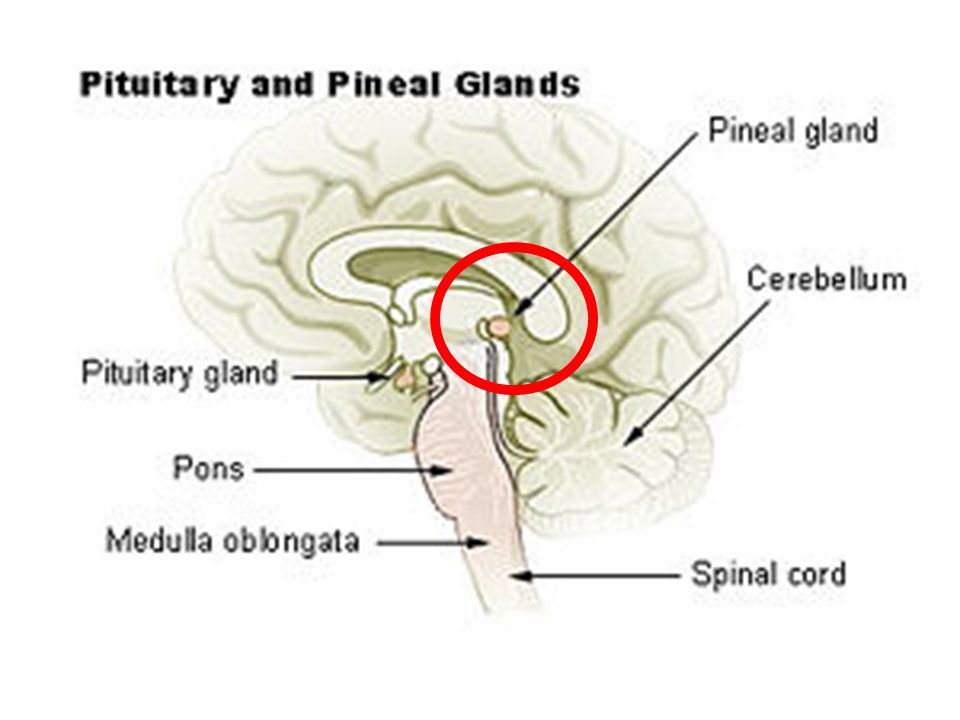

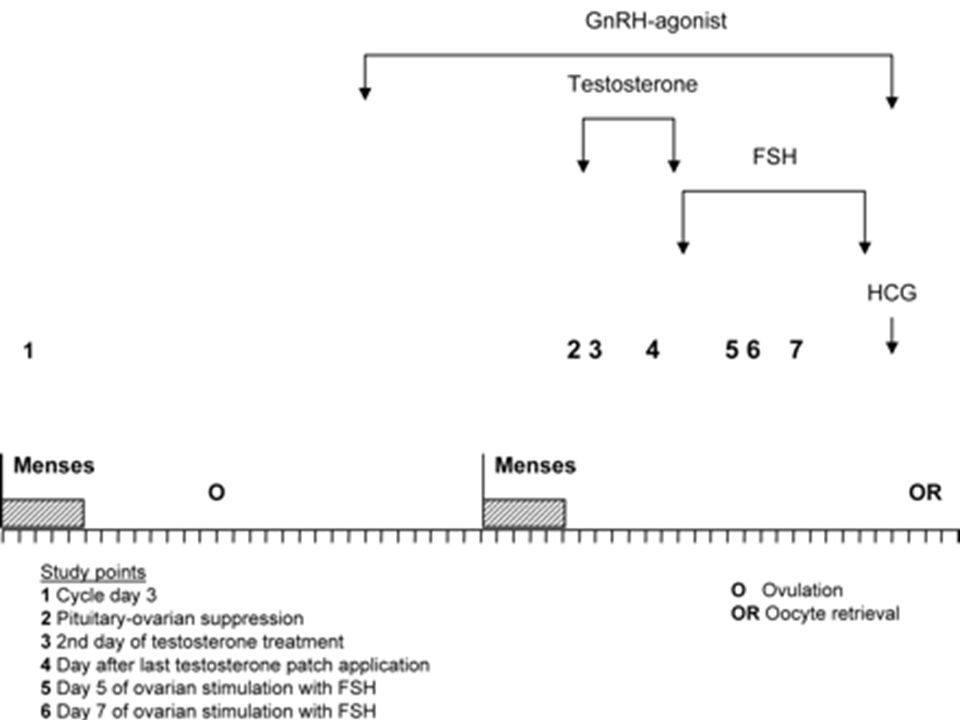
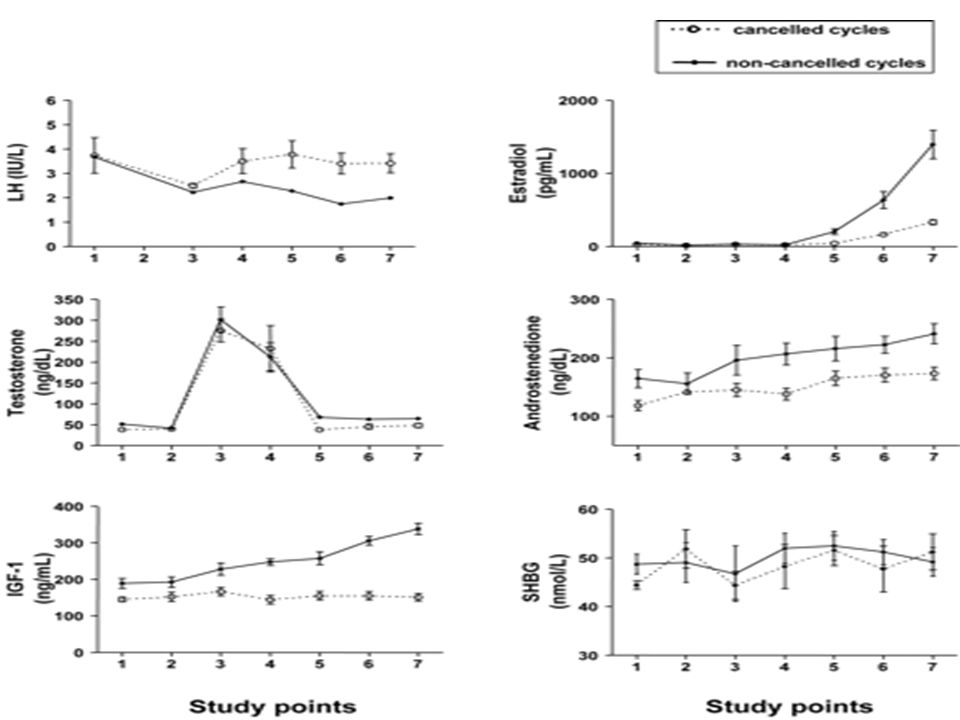

























 Endocrinology D R Davies School of Biological Sciences Purves Life: the Science of Biology Chapters 41 (Animal Hormones) and 15.>")
