Download presentation
Presentation is loading. Please wait.

1
The Future of the HCV Workforce: Lessons Learned from HIV Marissa Tonelli Senior Manager, HealthHCV

3
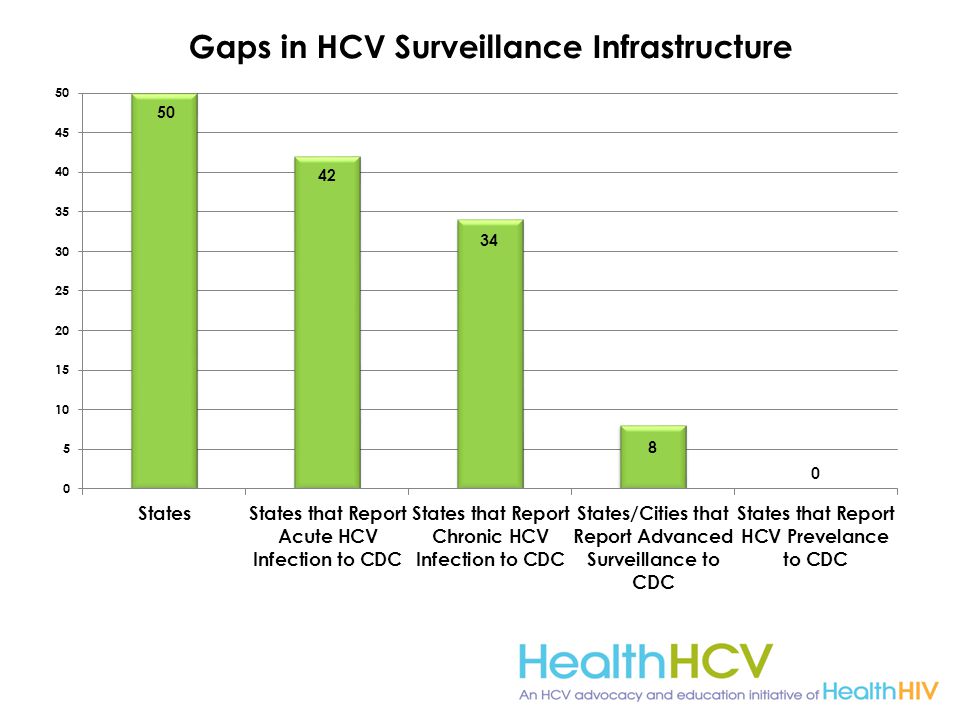
HIV/Hep C Surveillance Comparison

4
Purpose Education & Training: deliver medical and consumer education and training programs to improve the ability of organizations, professionals, and individuals to address HCV Research & Evaluation: conduct health services research to identify trends across HCV, HIV, and the broader health care landscape Advocacy: develop sound public health policy responsive to the shifting landscape of HCV and health care

5
Chronic HCV Infection in the US More than 5.2 million living with chronic HCV in US – Prevalence: 2% Chronic HCV cases not included in NHANES (CDC health statistics survey) estimate – Homeless (n=142,761-337,6100) – Incarcerated (n=372,754- 664,826) – Veterans (n=1,237,461- 2,452,006) – Active military (n=6,805) – Healthcare workers (n=64,809-259,234) – Nursing home residents (n=63,609) Chak E, et al. Liver Int. 2011; 31:1090-1101; http://www.cdc.gov/hepatitis/HCV/HCVfaq.htm#section2.

6
Davis GL. Rev Gastroenterol Disord 2004;4:7-17. Disease Burden of Patients Infected 20 Years or More is Peaking Now Patients infected Infected >20 yrs Prevalence (%) 1960 1970 1980 1990 2000 2010 2020 2030 4.0 3.0 2.0 1.0 0.0 People living with HCV for over 20 years in relation to all infected patients is increasing.
 People living with HCV for over 20 years in relation to all infected patients is increasing..")
7
20002010202020302040 HCV infection 2,940,6782,870,3912,281,5562,433,7092,177,089 Cirrhosis 472,103720,807858,788879,747828,134 Decompensated Cirrhosis 65,294103,117134,743146,408142,732 Hepatocellular Carcinoma 7,27111,18513,18313,39012,528 Liver-related death 13,00027,73236,48339,87539,064 Davis GL et al. Liver Transpl 2003;9:331-338. Morbidity and Complications Increase as Infected Population Ages

8
Baby Boomers 5x more likely to be infected with HCV 3 out of every 4 people living with HCV are born between these years 73% of HCV-related deaths are among baby boomers CDC Know More Hepatitis Campaign. http://www.cdc.gov/knowmorehepatitis/media/pdfs/infographic-paths.pdfhttp://www.cdc.gov/knowmorehepatitis/media/pdfs/infographic-paths.pdf

9
Increasing Burden of Disease Large pool of surviving patients remains at risk of progressive disease as the duration of their infection increases A dramatic increase will occur in the number patients with liver failure, HCC (cancer), and death caused by liver disease Identification and treatment of a larger proportion of infected patients may decrease morbidity and mortality from this disease Davis GL et al. Liver Transpl 2003;9:331-338.

10
The Problem: Only One-Half of Those Infected with HCV Are Aware of Their Infection Adapted from Volk ML et al. Hepatology 2009;50:1750-1755. 49% Aware of their infection 51% Unaware of their infection

11
Who Should Be Screened for HCV Everyone born from 1945 through 1965 (one-time) Persons with abnormal ALT levels HIV positive persons Past or present injection drug use Sex with an IDU; other high-risk sex Incarceration Intranasal drug use Receiving an unregulated tattoo Children born to an HCV- infected mother Recipients of blood transfusion or organ transplant prior to 1992 Persons who received clotting factor concentrates produced before 1987 (such as persons with hemophilia) Chronic (long-term) hemodialysis Occupational percutaneous exposure (needle stick) Surgery before implementation of universal precautions Smith at al. Ann Intern Med 2012; 157:817-822. Moyer et al. Ann Intern Med epub 25 June 2013

12
USPSTF/CDC Guidelines Recommends screening for hepatitis C virus (HCV) infection in persons at high risk for infection (Grade B) Recommends offering 1-time screening for HCV infection to adults born between 1945 and 1965 (Grade B)
 infection in persons at high risk for infection (Grade B) Recommends offering 1-time screening for HCV infection to adults born between 1945 and 1965 (Grade B)")
13
Asymptomatic patients without any other medical problems may not seek medical attention Many primary care physicians lack knowledge about risk factors and testing for hepatitis C Patients may be reluctant to reveal risk factors Patients may be outside healthcare system (young, poor, drug addicts) Reasons for Failure to Identify Chronic HCV Infection Adapted from Volk ML et al. Hepatology 2009;50:1750-1755.

17
Undiagnosed/Untreated HCV May Lead to Chronic Liver Disease and Liver Cancer Fibrosis 1 Chronic HCV infection can lead to the development of fibrous scar tissue within the liver Fibrosis 1 Chronic HCV infection can lead to the development of fibrous scar tissue within the liver FibrosisCirrhosis Hepatocellular Carcinoma (with cirrhosis) Cirrhosis 1,2 Over time, fibrosis can progress, causing severe scarring of the liver, restricted blood flow, impaired liver function, and eventually liver failure Cirrhosis 1,2 Over time, fibrosis can progress, causing severe scarring of the liver, restricted blood flow, impaired liver function, and eventually liver failure HCC 3 Cancer of the liver can develop after years of chronic HCV infection HCC 3 Cancer of the liver can develop after years of chronic HCV infection Chronic liver disease includes fibrosis, cirrhosis, and hepatic decompensation; HCC=hepatocellular carcinoma. 1. Highleyman L. Hepatitis C Support Project. http://www.hcvadvocate.org/hepatitis/factsheets_pdf/Fibrosis.pdf. Accessed August 18, 2011; 2. Bataller R et al. J Clin Invest. 2005;115:209-218; 3. Medline Plus. http://www.nlm.nih.gov/medlineplus/enxy.article/000280.htm. Accessed August 28, 2012; 4. Centers for Disease Control and Prevention. http://www.cdc.gov/hepatitis/HCV/HCVfaq.htm. Accessed May 8, 2012. Decompensated cirrhosis: Ascites Bleeding gastroesophageal varices Hepatic encephalopathy Jaundice

19
HIV/HCV Co-infection Epidemiology 20-30% of people with HIV are co-infected with HCV HIV/HCV co-infection is more common in people with high exposures to blood and blood products 60-90% of HIV positive hemophiliacs have HCV 50-70% of HIV positive IDUs have HCV Increasing incidence of HCV in HIV+ MSM Liver disease (mostly related to HCV) is the second leading cause of death in people with HIV infection Over 80% of people with HIV/HCV have genotype 1 infection (harder to treat) Maier, World Zj Gastro 2002; Sherman, CID 2002; Smith, AIDS 2012;
 is the second leading cause of death in people with HIV infection Over 80% of people with HIV/HCV have genotype 1 infection (harder to treat) Maier, World Zj Gastro 2002; Sherman, CID 2002; Smith, AIDS 2012;")
20
Comparing HIV/HCV Co-infection to HCV Mono-infection Positives: Higher rate of HCV diagnosis Better coverage and services for HCV infection (sometimes) through ADAP/Ryan White Negatives: Faster progression to cirrhosis Fewer diagnosed people treated for HCV (due to co- infection complications) Delayed inclusion in clinical trials for HCV Neither: Cure rates with DAA-containing regimens (has not been determined) Clinical benefits of cure Graham CID 2001; Davies, PLoS ONE 8(2): e55373. doi:10.1371/journal.pone.0055373

21
Who is Providing HCV Treatment? Primarily Hepatologists Gastroenterologists Infectious Diseases Specialists Secondarily PCPs Physician extenders – NP, PA

22
Costs of HCV Treatment Standard cost of HCV treatment (Peg-INF & RBV)= about $35k Plus DAA (telaprevir/boceprevir)= about $90k Estimated cost of new market treatments (sofosbuvir)= additional $84k Over the next 20 years, total medical costs for patients with HCV infection are expected to increase from $30 billion in 2009 to over $85 billion in 2024 FDA Approves 'Game Changer' Hepatitis C Drug Sofosbuvir. Medscape. Dec 06, 2013. NVHR 2014

23
Don’t Assume Regimens That Cost Less Are Actually Cheaper Actual Costs of Peg- IFN/RBV + TVR or BOC 1 (DAAs) Prior Response Mean Cost per SVR Naïve (n=57)$125,915 Relapse (n=61)$164,840 Partial or Null Responders (n=82) $302,070 Willingness-to-pay threshold for new regimens Need payer data, real- world clinical effectiveness data, and models Cirrhosis (n=82) $266,670 1 Sethi, AASLD 2013; #1847
 Prior Response Mean Cost per SVR Naïve (n=57)$125,915 Relapse (n=61)$164,840 Partial or Null Responders (n=82) $302,070 Willingness-to-pay threshold for new regimens Need payer data, real- world clinical effectiveness data, and models Cirrhosis (n=82) $266,670 1 Sethi, AASLD 2013; #1847")
24
McAdam-Marx C, McGarry LJ, Hane CA, Biskupiak J, Deniz B, Brixner CI. All- Cause and Incremental Per Patient Per Year Cost Associated with Chronic Hepatitis C Virus and Associated liver Complications in the United States: A Managed Care Perspective. J Manag Care Pharm. 2011 Sep;17(7): 531-46.
:")
25
Implications of ACA USPSTF recommendations for HCV screening for at-risk and baby boomers Private Insurance: Only exceptions are grandfathered plans that existed before ACA implementation o Medicaid (Traditional): Elected independently on a state-by-state basis o Medicaid (Expanded): Required to cover without cost- sharing o Medicare: No finalized NCD for baby boomers, but covers screening at “increased risk” All forms of insurance are required to provide one drug per class to treat HCV
: Elected independently on a state-by-state basis o Medicaid (Expanded): Required to cover without cost- sharing o Medicare: No finalized NCD for baby boomers, but covers screening at increased risk All forms of insurance are required to provide one drug per class to treat HCV")
26
HealthHIV’s 3 rd Annual State of HIV Primary Care Survey Findings

28
Respondent Breakdown RespondentsProfessional DesignationLocation 2,531Prescribing Providers (MD, DO, NP, PA), Pharmacists, Dentists, Researchers, Health Administrators, Social Workers/Case Managers, Consumers 50 US States, 4 US territories, 28 Countries 2,494 (of 2,531) Prescribing Providers (MD, DO, NP, PA), Pharmacists, Dentists, Researchers, Health Administrators, Social Workers/Case Managers, Consumers 50 US States and Puerto Rico 371 (of 2,531) Prescribing Providers (MD, DO, NP, PA) working in the scope of primary care 45 US States and Puerto Rico
, Pharmacists, Dentists, Researchers, Health Administrators, Social Workers/Case Managers, Consumers 50 US States, 4 US territories, 28 Countries 2,494 (of 2,531) Prescribing Providers (MD, DO, NP, PA), Pharmacists, Dentists, Researchers, Health Administrators, Social Workers/Case Managers, Consumers 50 US States and Puerto Rico 371 (of 2,531) Prescribing Providers (MD, DO, NP, PA) working in the scope of primary care 45 US States and Puerto Rico")
29
Methods Fifty-five question instrument (51 quantitative, 4 qualitative) Distributed online using Survey Monkey TM (March 7 – June 17, 2013) Recruited using email lists, monthly newsletters, and website postings Convenience sample; no incentive provided
 Distributed online using Survey Monkey TM (March 7 – June 17, 2013) Recruited using lists, monthly newsletters, and website postings Convenience sample; no incentive provided")
30
HIV PCP Profile Comparison

31
Gaps in HCV Care Capacity 89% of PCPs treating HIV also provide HCV screening 97% provide HCV screening to all patients born between 1945 and 1965, or based on identified risk factors

32
Gaps in HCV Care Capacity

33
Survey Implications Highlights need for HCV education among both PCPs treating HIV and those who are not Leverage specialists working in primary care as mentors to train other PCPs on treating HIV/HCV Correlation between mental health/substance abuse and poor health outcomes for people living with HIV/HCV suggests services have yet to be integrated fully into primary care settings PCPs must be trained more thoroughly on ACA, especially changes to service delivery and reimbursement (i.e. treatment costs)
.")
34
HCV Provider Survey HealthHIV surveyed 64 providers at AASLD’s Liver Meeting on Nov 1-4 th, 2013: Over half of respondents (56%) were MDs 11% of respondents were NPs 5% of respondents were PAs Half of respondents (48%) practice in the US
 were MDs 11% of respondents were NPs 5% of respondents were PAs Half of respondents (48%) practice in the US")
35
HCV Survey Findings Half (51%) believe capacity of healthcare system is insufficient to diagnose/treat HCV Roughly one-third (36%) believe PCPs should co- manage HCV care/treatment with specialist -Only 16% believe PCPs should provide comprehensive HCV care Over half (62%) believe low patient awareness on HCV risk factors is a barrier to providing HCV testing Clear majority (80%) expressed strong interest in receiving medical education on new HCV therapies HCV treatment algorithms was the most requested CME topic
 believe capacity of healthcare system is insufficient to diagnose/treat HCV Roughly one-third (36%) believe PCPs should co- manage HCV care/treatment with specialist -Only 16% believe PCPs should provide comprehensive HCV care Over half (62%) believe low patient awareness on HCV risk factors is a barrier to providing HCV testing Clear majority (80%) expressed strong interest in receiving medical education on new HCV therapies HCV treatment algorithms was the most requested CME topic")
36
Best Practices for Screening Testing needs to be implemented in settings with high HCV prevalence such as prisons, substance abuse programs, and STD clinics Prevention efforts are needed for the younger population in high-risk settings such as substance abuse programs Routinize HCV screening: Consider EMR reminders help to prompt providers to test patients born between 1945-1965 MedScape Hot Topics, Nov 2013

37
Education for Patients Educate patients on: o Transmission of HCV o Need to be screened for HCV o Importance of adherence and engagement in care o Screening and treatment coverage/availability that result from the ACA and new treatment development MedScape Hot Topics, Nov 2013

38
Education for Advocates Advocates need to be aware of: o Burden of disease and surveillance o Need for increase in surveillance mechanisms o At-risk populations (in order to advocate for appropriate allocation of resources) o Best methods to translate educational initiatives to at-risk populations o What treatment is available to patients depending on insurance to ensure treatment access for all patients regardless of socioeconomic or insurance status o How PCPs can increase adherence to treatment and reduce risk factors for cirrhosis, etc in primary care settings MedScape Hot Topics, Nov 2013
 o Best methods to translate educational initiatives to at-risk populations o What treatment is available to patients depending on insurance to ensure treatment access for all patients regardless of socioeconomic or insurance status o How PCPs can increase adherence to treatment and reduce risk factors for cirrhosis, etc in primary care settings MedScape Hot Topics, Nov 2013")
39
Education and Training for PCPs Expanding HVC patient population creates a need for PCPs to initiate and provide HCV treatment PCPs need information on: o Screening guidelines (at-risk populations and birth cohort) o Newest treatment methods and side effects of those methods o Determining treatment options for patients, including special populations, to ensure SVR Implement team approach with PCP, physician extenders (NP/PA), support staff, specialist, and patient PCPs (and physician extenders) are responsible for educating patients about their disease, drug regime, side effects, the importance of adherence to treatment, and the consequences of non-adherence to treatment MedScape Hot Topics, Nov 2013
 o Newest treatment methods and side effects of those methods o Determining treatment options for patients, including special populations, to ensure SVR Implement team approach with PCP, physician extenders (NP/PA), support staff, specialist, and patient PCPs (and physician extenders) are responsible for educating patients about their disease, drug regime, side effects, the importance of adherence to treatment, and the consequences of non-adherence to treatment MedScape Hot Topics, Nov 2013")
40
Provides HIV expert mentoring to clinicians in primary care practices, community health centers, health clinics, and residency program Matches MD, NP, PA to HIV clinical experts for coaching and training on HIV care Offers expansive educational resources to mentors and mentees

41
Lessons Learned from Workforce Initiative PCPs have the skills to treat complex infectious diseases (such as HIV/HCV), but lack confidence There is an increased need for PCP integration in HIV/HCV care in rural areas with fewer specialists As PCPs became more advanced in HIV treatment, they asked more about HCV co- infection and mono-infection PCPs are overburdened and need incentives for completing training programs
, but lack confidence There is an increased need for PCP integration in HIV/HCV care in rural areas with fewer specialists As PCPs became more advanced in HIV treatment, they asked more about HCV co- infection and mono-infection PCPs are overburdened and need incentives for completing training programs")
42
HealthHIV’s HIV Primary Care Training and Certificate Program

43
2000 S Street NW Washington, DC 20009 202.232.6749 www.healthhiv.org

Similar presentations












 New Orleans September 10, 2013 Jen Kates, Kaiser Family Foundation.>")





 www.ahrq.gov.>")





