Download presentation
Presentation is loading. Please wait.

1
بسم الله الرحمن الرحيم ”وقل رب زدنى علما “

2
Dr: IMRANA ZULFIKAR ASSISSTANT PROFESSOR Surgical dept:

4
Cleft: Clefting is deformity, in fusion of mid face skeleton with soft tissue, occurs in second month of pregnancy. Cleft lip and palate(1:600 live birth). Cleft palate alone (1:1000 live birth)
. Cleft palate alone (1:1000 live birth).")
5
Incidence: Cleft lip and palate------45%, F > M Cleft lip alone-------------15% Cleft palate alone-------40% M>F Cleft lip and palate is more common on the left side Inc: in oriental groups (1:500) Dec: in negro population (1:2000)
 Dec: in negro population (1:2000)")
6
ETIOLOGY: Genetic : Family history: 1 st degree affacted have risk of(1:25 live birth). Isolated: Syndrome: over 150 syndroms are associated Pierre robin syndrome, Syickler syndrome Shprintzen, Down, apert, treacher collins. Environment: Maternal epilepsy Drug ( steroid, phenytion, diazepam)
.")
7
Genetic factors Syndrome vs. sequence Pierre Robin sequence –Small mandible (micrognathia) causes failure of tongue to descend –Failure of the tongue to descend causes cleft –Heart problems, conductive hearing loss, developmental deficits –about 40% of infants with Pierre Robin have Stickler Syndrome and about 15% have Velocardiofacial SyndromeStickler SyndromeVelocardiofacial Syndrome Treacher Collins syndrome –Under-developed cheekbones with scalp hair –Malformed ears –Conductive hearing loss –Normal cognitive functioning
 causes failure of tongue to descend –Failure of the tongue to descend causes cleft –Heart problems, conductive hearing loss, developmental deficits –about 40% of infants with Pierre Robin have Stickler Syndrome and about 15% have Velocardiofacial SyndromeStickler SyndromeVelocardiofacial Syndrome Treacher Collins syndrome –Under-developed cheekbones with scalp hair –Malformed ears –Conductive hearing loss –Normal cognitive functioning.")
8
Chromosomal abnormalities Trisomy 13 –Rare chromosomal abnormality –Multiple congenital malformations –Mean life expectancy is 130 days

9
Environmental factors Recognized teratogenic agents –Drugs –Aspirin overdose –Acne medications –Alcohol overdose –EPILEPTIC DRUGS –PHENYTOIN

10
Mechanical factors Intrauterine crowding (tumors, multiple births, placenta abnormalities) AMNIOTIC BAND SYDROME
 AMNIOTIC BAND SYDROME")
11
EMBRYOLOGY When the fetus is developing, the face forms by the fusion of five different facial processes, that must fit together perfectly to create a complete face. Frontonasal process. Maxillary process Mandibular process. Medial nasal process. Lateral nasal process. When two of these processes fail to come together, for whatever reason, a cleft is formed

12
Physiology of palate: Separate the nasal cavity from oral cavity. Soft palate cuts off oropharynx from nasopharynx during feeding. Palate generating suction with their mouths, during feeding the infant. During speech, closure of soft palate is essential. an intact palate with normal muscle function is necessary for proper drainage of the middle ear.

14
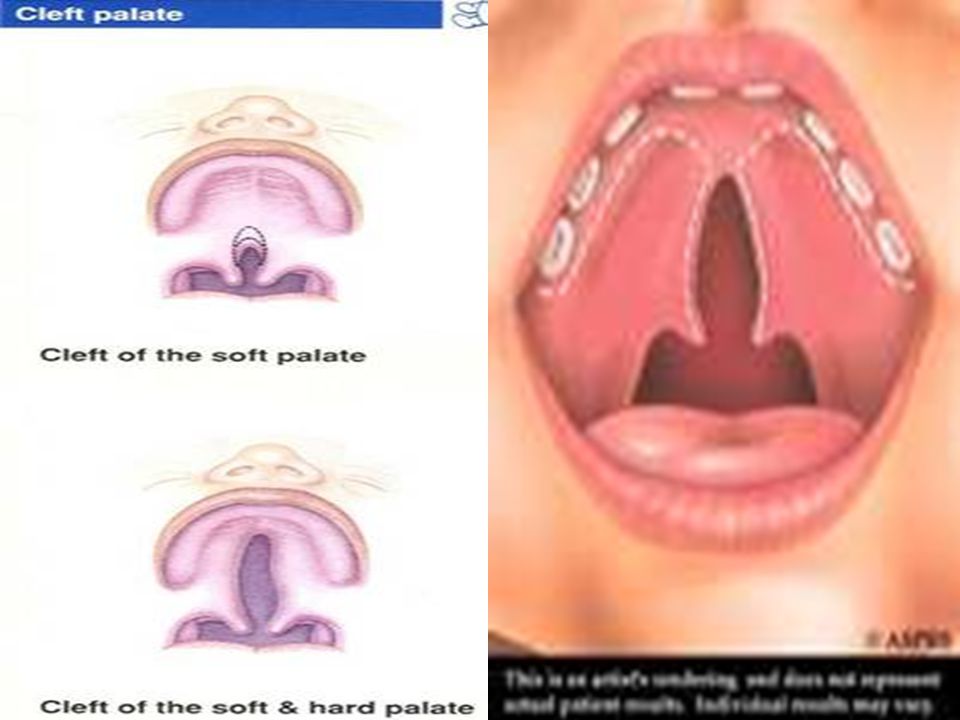
classification Cleft lip and palate Cleft lip alone This separation can vary from a subtle notch or groove to a wide gap. Cleft palate alone Cleft palate occur in midline (isolated) extend to uvula, soft palate, hard palate, incisive foramen
 extend to uvula, soft palate, hard palate, incisive foramen.")
15
LAHSHAL lahsl L CLEFT LIP A ALVEOLUS H HARD PALATE S SOFT PALATE

16
Cleft lip and palate Classification systems Numerous classification systems: Veau American Cleft Palate-Craniofacial Assn (ACPA) Kernahan and Stark Veau’s system: ICleft of soft palate only II Cleft of hard and soft palate to incisive foramen III Complete unilateral cleft of soft and hard palate and lip and alveolar ridge on one side IV Complete bilateral cleft of soft and hard palate and lip and alveolar ridge on both sides
 Kernahan and Stark Veau’s system: ICleft of soft palate only II Cleft of hard and soft palate to incisive foramen III Complete unilateral cleft of soft and hard palate and lip and alveolar ridge on one side IV Complete bilateral cleft of soft and hard palate and lip and alveolar ridge on both sides")
17
Anatomical defects : Cleft lip: Nasolabial and bilabial muscle rings disruption results deformities involving mucocutanous tissue, muscular and bony deformity.

18
Unilateral: Muscle rings disrupt on one side results asymmetrical deformity. Bilateral : Bilateral disruption produce symmetrical deformity.

19
Complete CL: A gap goes all the way from the lip, mouth into nose, called Complete cleft. Incomplete CL: A gap does not extend from mouth all the way into nose, called an Incomplete cleft. Microform CL: Incomplete cleft is very minor (a groove or a notch), called a Microform cleft.
, called a Microform cleft..")
22
Cleft palate : Failure of fusion of two palatine process.it may involve: Soft palate Hard and soft palate. Hard palate may be: Complete: nasal septum and vomer bone completely separated from palatine process. Incomplete: cleft of hard palate remains attached to nasal septum and vomer.

26
Antenatal diagnosis : Only possible for cleft lip by US after 18wk of gestation. Postnatal diagnosis: Immediate problems : feeding problem breathing problem Associated anamolies.

27
Late problems : Recurrent serous otitis media Hearing language delays speech problem (hypernasality, articulation error ) Orthodentic complication (delayed development. Delayed eruption, morphological abnormalities, hypodontia, hyperdontia) Cosmetic disfigurement. psychological problems.
 Cosmetic disfigurement. psychological problems..")
28
Primary management Feeding problem manage : Breathing problems manag Primary surgical procedure

29
Feeding problem management: Mother advised: Breastfeeding is unlikely to be unsuccessful. Bottle feeding with soft plastic bottle (squeezed rhythmically to squirt milk into oral cavity). Position of baby should upright, prevent nasal regurgitation.
. Position of baby should upright, prevent nasal regurgitation..")
30
Breathing problems management : Nursing the in prone position. Persistent airway compromise managed by “retained nasopharyngeal intubation”. Labioglossopexy in first few days is alternative.

31
Primary surgical procedure

32
Goals of surgery: Normal appearance of lip, nose, face. Normal speech Dentition and facial growth within normal range of development. Principals of surgery: To restore the normal anatomy by muscular reconstruction.

35
Timing of primary surgical procedure CL repair is performed B/W 3-6 month of age. CP repair is performed B/W 6- 18month of age.

36
Cleft lip alone : one operation Unilateral: 5-6 month. Bilateral: 4-5 month. Cleft palate alone: Soft palate only: 6month Soft and hard palate: Two operation Soft palate at 6month Hard palate at 15-18 month. Cleft lip and palate: Unilateral and Bilateral: Two operation - Cleft lip and Soft palate at 5-6 month. - Hard palate and gum pad with or - without lip revision at 15- 18 month

40
Secondary management Hearing problems Speech problems Dental development Facial growth

41
Hearing management: Sensoneuranal hearing loss: with hearing aid Conductive loss due to serious otitis media Prophylactic myringotomy grommet insertion. Regular autological testing.

42
Speech problem management: Speech and language therapy Secondary palatal surgery Intralveolar veloplasty Pharyngoplasty Speech training devices.

43
Orthodontic management : In two phases 1. mixed dentition (8-10 yrs) to expend maxillary arches by alveolar bone graft. 2. Parmanent dentition (14-18 yrs) to aligndentition by maxillar osteotomy.
 to expend maxillary arches by alveolar bone graft. 2. Parmanent dentition (14-18 yrs) to aligndentition by maxillar osteotomy..")
44
Cleft lip revision surgery: Indication: Lip deformity: -Misaligned vermilion -Asymmetrical or muscle discontinuity. Nasal deformity: -Lateral drift of alar base -Poor nasal tip projection -Deviation of cartilaginous nasal septum.

Similar presentations





























 and Scotland (SC041034) Cleft Lip and Palate.>")

