Download presentation
Presentation is loading. Please wait.

1
Pelvic Floor Dysfunction
OB & GYN Hospital, Fudan University Lei Yuan , MD

2
Questions What does pelvic floor consist of? Where are they? (Location, Function)
")
3
Pelvis 版权所有

4
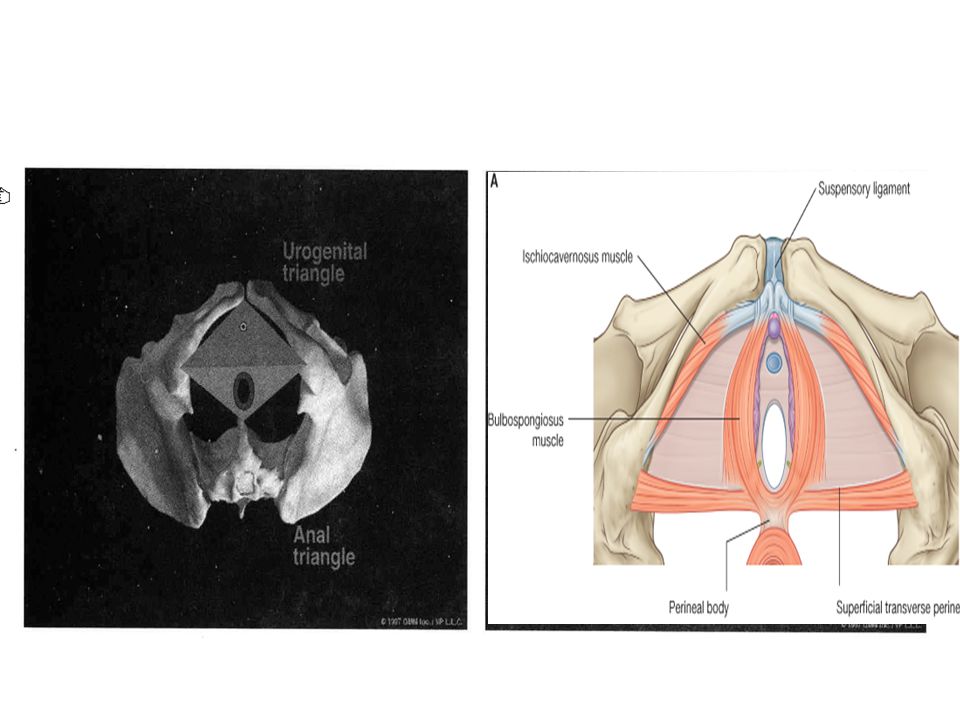
Anatomy of Pelvic floor
anal triangle urogenital triangle skin subcutaneous tissue superficial perineal fascia bulbospongiosus m./ ischiocavernosus m./ ischiorectal fossa superfical transverse perineal m. Inferior fasica of UG diaphragm deep transverse perineal m. Superior fasica of UG diaphragm Inferior fasica of Pelvic diaphragm levator ani m., coccygeus m. superior fasica of Pelvic diaphragm

8
Pelvic diaphragm 耻尾肌 (Pubococcygeus) 耻骨直肠肌 (Puborectalis) 坐骨尾骨肌
髂尾肌 (Iliococcygeus) 耻尾肌 (Pubococcygeus) 耻骨直肠肌 (Puborectalis) 版权所有
 耻尾肌 (Pubococcygeus) 耻骨直肠肌 (Puborectalis) 版权所有.")
10
Arcus tendineus(white line)
盆筋膜腱弓(白线) (Arcus tendineus fasciae pelvis) 肛提肌腱弓 (Arcus tendineus levator ani) 版权所有
 (Arcus tendineus fasciae pelvis) 肛提肌腱弓. (Arcus tendineus levator ani) 版权所有.")
11
Fascia and ligaments 版权所有

12
Anatomy of Pelvic floor
anal triangle urogenital triangle skin subcutaneous tissue superficial perineal fascia bulbospongiosus m./ ischiocavernosus m./ ischiorectal fossa superfical transverse perineal m. Inferior fasica of UG diaphragm deep transverse perineal m. Superior fasica of UG diaphragm Inferior fasica of Pelvic diaphragm levator ani m., coccygeus m. superior fasica of Pelvic diaphragm

13
Longitudinal view

14
Function of pelvic diaphragm
版权所有

15
Function of pelvic floor
Supportive structure Orchestrate a series of physiological function Parturition Micturition Defecation Pelvic organ prolapse Lower urinary tract disorder (SUI) Anorectal Disorder ( fecal incontinence)
 Anorectal Disorder. ( fecal incontinence)")
16
Integral Theory (Petros)
Anatomic anomaly functional abnormalities Site specific defects LEVEL 1 ligaments(cardinal lig. Uterosacral lig.) LEVEL 2 pelvic diaphragm, muscle( levator ani.) LEVEL 3 perineum & soft tissue
 LEVEL 2 pelvic diaphragm, muscle( levator ani.) LEVEL 3 perineum & soft tissue.")
17
Integral Theory (Petros)
RFRF Restoration of form(structure) leads to Restoration of function Principles of surgery Retain; Reconstruction; Replacement(mesh)
 leads to Restoration of function. Principles of surgery. Retain; Reconstruction; Replacement(mesh)")
18
3 levels of support Delancey, 1994

19
Three zones (compartments )of pelvis
Anterior zone Middle zone Posterior zone

20
Case discussion

21
Chief complain:feeling a ball in the vagina for 4 years and progressively worsen for the last 6 months 版权所有

22
Question What else would you like to know about the patient’s history?
版权所有

23
Risk factors for PFD Pregnancy Vaginal childbirth Menopause Aging Hypoestrogenism Chronically increased intra-abdominal pressure Chronic obstructive pulmonary disease (COPD) Constipation Obesity Pelvic floor trauma Genetic factors Race Connective tissue disorders Hysterectomy Spina bifida
 Constipation Obesity Pelvic floor trauma Genetic factors Race Connective tissue disorders Hysterectomy Spina bifida")
24
The causes of uterine prolapse?
Age? The causes of uterine prolapse? chronic coughing? Chronic diarrhea or constipation? Cachexia? Clinical symptoms bulge symptom; urinary and bowel symptoms; sexual symptom; pain Accessory examination and history acquiring History of pregnancy and parturition History of DM、TB, etc Accessory examination to exclude malignant disease and other nervous system disease Previous treatment 版权所有

25
The complete case Chief complain:
feeling a ball in the vagina for 4 years and progressively worsen for the last 6 months History: Previous menstruation: regular, 7/27-32,moderate volume; dysmenorrhea(-). Natural menopause for 30 yrs and never receive HRT after menopause. No abnormal vaginal bleeding and vaginal discharge. Sensation of a vaginal protrusion 4 yrs ago and the size was the same like a bean, the symptom was deteriorated when standing or pelvic pressure increased while alleviated after lying down. Pessary use was recommended 1 yr ago, however, the patient didn’t use it because of the difficulty of removing the pessary. 版权所有
. Natural menopause for 30 yrs and never receive HRT after menopause. No abnormal vaginal bleeding and vaginal discharge. Sensation of a vaginal protrusion 4 yrs ago and the size was the same like a bean, the symptom was deteriorated when standing or pelvic pressure increased while alleviated after lying down. Pessary use was recommended 1 yr ago, however, the patient didn’t use it because of the difficulty of removing the pessary. 版权所有.")
26
The symptom was deteriorated in the last 6 months with the egg-like ball bulged totally from the vagina when walking and only part of it can be returned to the vagina after lying down. However, the protrusion can be totally returned to the vagina by hand. No concurrent urinary frequency, urinary urgency, seldom complain of voiding dysfunction but didn’t receive any treatment. Good control of urination and never had involuntary leakage of urine with coughing. No abdominal pain or low back pain, no abnormal vaginal discharge. No change in appetite or sleep pattern, no cachexia, complain of constipation in recent months.

27
Marital and Fertile History:
Previous history: Hypertension for 1 yr, BP: /50-60mmHg,maxium: 180/80mmHg. Current treatment: Levamlodipine Beslate p.o DM for 6-7yrs, Current treatment: Insulin 14u(am), 0u(noon), 5u(pm), s.c; Acarbose: 1# tid, p.o No previous surgery Marital and Fertile History: G2P2,1963,1966 vaginal delivery,fetal birth weight :3kg No dystocia history 版权所有
, 0u(noon), 5u(pm), s.c; Acarbose: 1# tid, p.o. No previous surgery. Marital and Fertile History: G2P2,1963,1966 vaginal delivery,fetal birth weight :3kg. No dystocia history. 版权所有.")
28
Cervix: atrophy, decent totally beyond the hymen
Pelvic examination Vagina: no congestion Cervix: atrophy, decent totally beyond the hymen Uterus: decent totally beyond the hymen, atrophy, unfixed, no tenderness Adnexal: normal Vagino-recto-abdominal examination: normal Valsalva maneuver 版权所有

29
POP-Q +3 +5 4 2 7 +6 版权所有

30
Question Initial diagnosis?
Pelvic floor dysfunction: Anterior III, Middle IV, Posterior III II-DM Chronic hypertension 版权所有

31
Question Next step? (Accessory examination) Urodynamics
Detect blood glucose(BG), BP ECG+Holter Pulmonary function (>70ys) Echocardiography(>70ys) 版权所有
, BP. ECG+Holter. Pulmonary function (>70ys) Echocardiography(>70ys) 版权所有.")
32
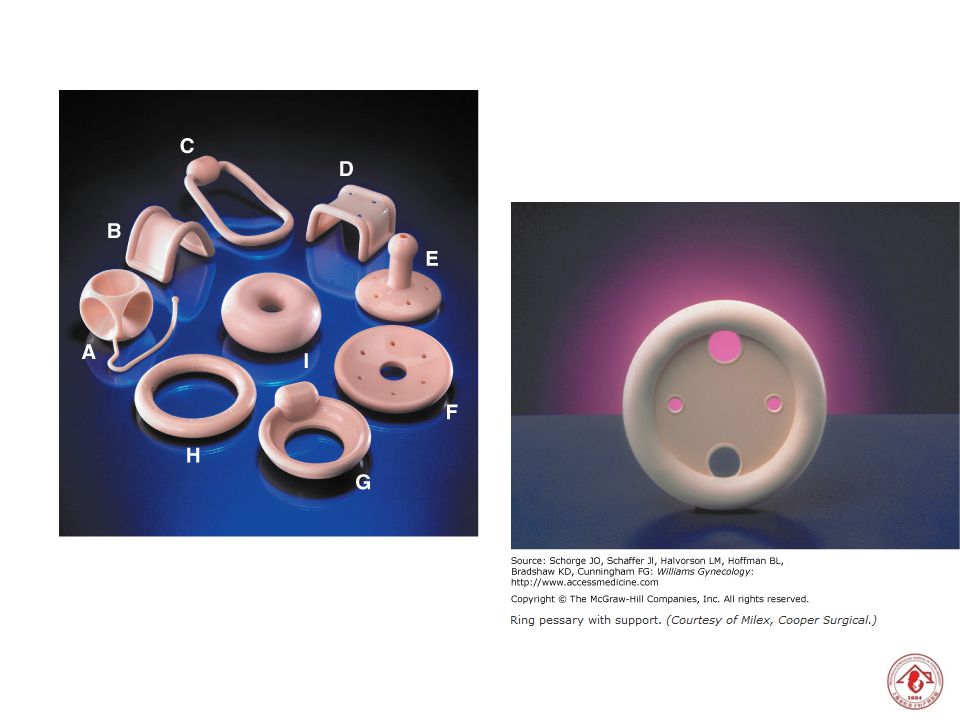
Question Treatment( Principle? Option?) Pessary Laprotomy Laproscopy
Vaginal surgery Transvaginal hysterectomy +Pelvic floor reconstruction(Total prolift) Transvaginal hysterectomy + anterior and posterior vaginal wall repair Transvaginal hysterectomy + Sacrospinous Ligament Fixation + Midurethral Slings (tension free vaginal tape , TVT) Transvaginal hysterectomy +Lefort surgery Lefort surgery 手术方式,针对不同compartment的手术方式不同 Individulized therapy 治疗分:Conservative and surgical 保守性治疗中又分:pelvic floor muscle training (PFMT).(有Kegal 训练及生物电刺激 )及Mechnical treatment(子宫托) 版权所有
 Transvaginal hysterectomy + anterior and posterior vaginal wall repair. Transvaginal hysterectomy + Sacrospinous Ligament Fixation. + Midurethral Slings (tension free vaginal tape , TVT) Transvaginal hysterectomy +Lefort surgery. Lefort surgery. 手术方式,针对不同compartment的手术方式不同. Individulized therapy. 治疗分:Conservative and surgical. 保守性治疗中又分:pelvic floor muscle training (PFMT).(有Kegal 训练及生物电刺激 )及Mechnical treatment(子宫托) 版权所有.")
33
Treatment principles(1)
Treatment choice depends on the type and severity of symptoms, age and medical co-morbidities, desire for future sexual function and/or fertility, and risk factors for recurrence

34
Treatment principles(2)
Conservative treatment Indication: mild-moderate prolapse Procedures: Pessary Pelvic floor muscle exercise (Kegel exercises, biofeedback therapy)
")
35
Treatment principles(3)
Surgical treatment Indication: severe prolapse(>III), fail of conservative treatment Procedures: Obliterative procedures (Lefort colpocleisis; complete colpocleisis) Reconstructive procedures (depend on different compartments) If with concurrent SUI, midurethral sling is recommended
, fail of conservative treatment. Procedures: Obliterative procedures (Lefort colpocleisis; complete colpocleisis) Reconstructive procedures (depend on different compartments) If with concurrent SUI, midurethral sling is recommended.")
36
术式 Anterior compartment
anterior colporrhaphy(repair) If with moderate or severe SUI: TVT (Tension-Free Vaginal Tape) TVT-O Middle compartment (uterine prolapse, vaginal vault prolapse, enterocele, Douglas hernia) Tradition:vaginal hysterectomy、Manchester surgery、 colpocleisis Now:Pubovaginal Sling(PIVS)、Sacrospinous Ligament Fixation (SSLF) Posterior compartment posterior colporrhaphy(repair) Mesh 版权所有
 If with moderate or severe SUI: TVT (Tension-Free Vaginal Tape) TVT-O. Middle compartment (uterine prolapse, vaginal vault prolapse, enterocele, Douglas hernia) Tradition:vaginal hysterectomy、Manchester surgery、 colpocleisis. Now:Pubovaginal Sling(PIVS)、Sacrospinous Ligament Fixation (SSLF) Posterior compartment. posterior colporrhaphy(repair) Mesh. 版权所有.")
39
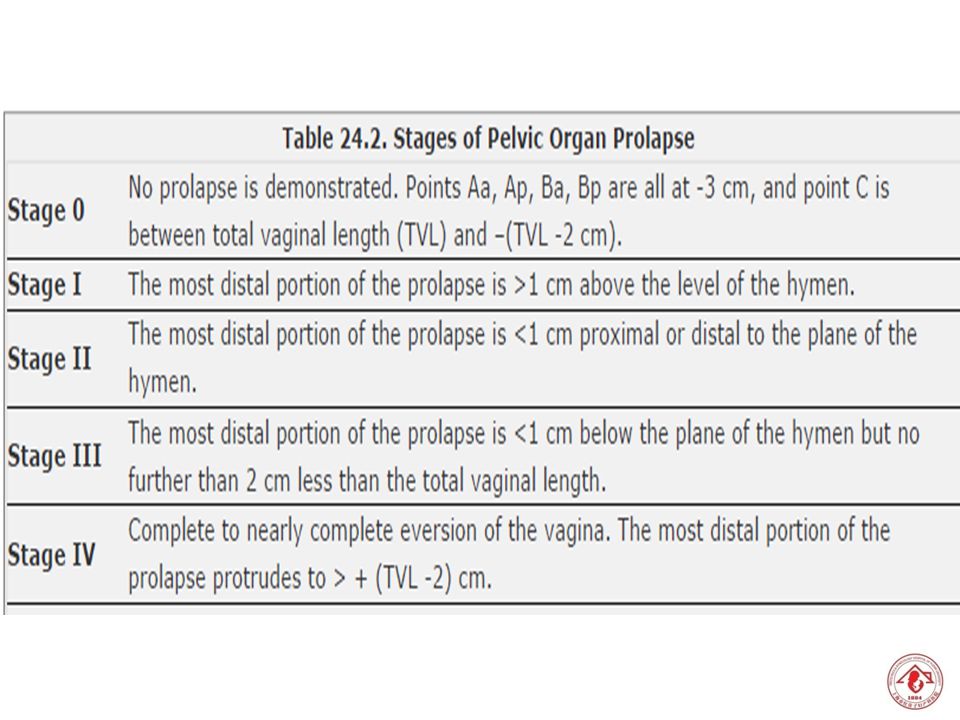
POP-Quantification

42
STAGE 3 STAGE 2 STAGE 4

43
Quiz: POP-Q application
1. POP-Q score? Anterior:III°(Ba+6) Posterior:I°(Bp-2) Middle(vaginal vault):I°(C-2) 2.Management 阴道前壁修补术 经阴道阴道旁修补术 TVT-O 版权所有
 Posterior:I°(Bp-2) Middle(vaginal vault):I°(C-2) 2.Management. 阴道前壁修补术. 经阴道阴道旁修补术. TVT-O. 版权所有.")
44
Quiz: POP-Q application
POP-Q score? Posterior:III °(Bp+5) Middle(vaginal vault):I°(C-6) 2.Management 经阴道后路悬吊带术(p-IVS) 骶棘韧带固定术(SSLF) Posterior colporrhaphy 版权所有
 Middle(vaginal vault):I°(C-6) 2.Management. 经阴道后路悬吊带术(p-IVS) 骶棘韧带固定术(SSLF) Posterior colporrhaphy. 版权所有.")
45
人类站起来了, 器官却掉下去了 Treatment When human being stand up,
Their organs decent…

46
Take home message Understand the anatomy of pelvic floor and etiology of pelvic floor dysfunction. Understand definition and types of pelvic organ prolapse and principle of treatment. Understand definition and types of lower urinary tract disorders and principle of treatment.

47
Thank You !

Similar presentations






















>")

