Download presentation
Presentation is loading. Please wait.

1
Nananda F. Col, MD, MPP, MPH, FACP Director, Center for Outcomes Research and Evaluation Maine Medical Center Maine Medical Center Dept of Medicine Coln@MMC.org Implementing Shared Decision Making: Improving Efficiency and Quality of Care

2
INTRODUCTION Most patients want to be more involved in decisions about their healthMost patients want to be more involved in decisions about their health Shared decisions have better outcomesShared decisions have better outcomes Despite repeated calls for shared decision making, it remains uncommonDespite repeated calls for shared decision making, it remains uncommon

3
What is Shared Decision Making?

4
What is Shared Decision Making (SDM)? A recent systematic review identified 161 different conceptual definitionsA recent systematic review identified 161 different conceptual definitions “A decision-making process jointly shared by patients and their health care provider”“A decision-making process jointly shared by patients and their health care provider”

5
QUESTION 1.How often do you engage in informed decision making with your patients? A.Most visits B.Occasionally C.Seldom D.Never

6
Elements of Informed Decision Making Discuss:Discuss: –clinical issue and nature of the decision to be made –alternatives –pros and cons of the alternatives –uncertainties associated with the decision Assess patient’s understandingAssess patient’s understanding Ask patient to express preferencesAsk patient to express preferences Braddock CH, JGIM 1997

7
QUESTION 2. How often do you discuss the uncertainty about risks and benefits of treatment? A.Most visits that involve a treatment decision B.Occasionally C.Seldom D.Never

8
How common is shared decision making? Analysis of 1057 clinical encounters by PCPs and surgeons 16-18% of discussions met minimum criteria for an informed decision16-18% of discussions met minimum criteria for an informed decision 1% discussed the uncertainty about risks and benefits of treatment1% discussed the uncertainty about risks and benefits of treatment Braddock, JAMA 1999

9
QUESTION State of Knowledge 3. What percent of all treatments for clinical prevention or treatment are of unknown effectiveness? A.95% B.75% C.50% D.<10% Clinical Evidence, BMJ

10
Answer: A recent comprehensive summary of the state of medical knowledge 47%: unknown efficacy47%: unknown efficacy 7%: uncertain tradeoff between benefits and harms7%: uncertain tradeoff between benefits and harms

11
The Challenge More and more people realize that they are the best judges of their values when deliberating over a health care decisionMore and more people realize that they are the best judges of their values when deliberating over a health care decision

12
Patient barriers to shared decision making Cognitive: complex risk informationCognitive: complex risk information Affective: anxiety, fearAffective: anxiety, fear Self-efficacy: medical decision makingSelf-efficacy: medical decision making Social/environmental influencesSocial/environmental influences –Locus of control for decision making

13
The Problem 52% of pts were dissatisfied with the information given (in all aspects) and reported a desire for more information52% of pts were dissatisfied with the information given (in all aspects) and reported a desire for more information The better the match between the information that was desired and the information received, the better patient outcomesThe better the match between the information that was desired and the information received, the better patient outcomes
 and reported a desire for more information52% of pts were dissatisfied with the information given (in all aspects) and reported a desire for more information The better the match between the information that was desired and the information received, the better patient outcomesThe better the match between the information that was desired and the information received, the better patient outcomes")
14
Role of Decision Support Tools Patient –Educate about risks, treatments, and how to incorporate preferences into the treatment decision PCP’s – collect relevant pt data (risk factors, medical history) – understand patient preferences for outcomes and treatments –Integrate/synthesize risks and preferences to make informed decisions
 – understand patient preferences for outcomes and treatments –Integrate/synthesize risks and preferences to make informed decisions")
15
Patient Decision Aids Adjuncts to counselling 1.Inform 2. Clarify values 3. Support

16
1. Inform Provide facts Condition, options, benefits, harms Communicate probabilities

17
2. Clarify values Patient experience Ask which benefits/harms matters most Facilitate communication

18
3. Support Guide in steps of deliberation, communication Worksheets, list of questions

19
What’s wrong with the status quo? Standard counseling is inadequateStandard counseling is inadequate Clinicians are poor judges of pts’ valuesClinicians are poor judges of pts’ values Leads to overuse of treatments that patients do not valueLeads to overuse of treatments that patients do not value Preference sensitive surgeries (hip replacements, prostatectomy, mastectomy, discectomy, CABG) vary 2-5 foldPreference sensitive surgeries (hip replacements, prostatectomy, mastectomy, discectomy, CABG) vary 2-5 fold Informing pts about these procedures ↓ use 25%Informing pts about these procedures ↓ use 25% –No adverse impact on pt satisfaction or health outcomes
 vary 2-5 foldPreference sensitive surgeries (hip replacements, prostatectomy, mastectomy, discectomy, CABG) vary 2-5 fold Informing pts about these procedures ↓ use 25%Informing pts about these procedures ↓ use 25% –No adverse impact on pt satisfaction or health outcomes.")
20
Compared to standard care, decision aids… Improve decision quality Improve decision quality 15% higher knowledge scores 15% higher knowledge scores 70% more realistic expectations (probabilities) 70% more realistic expectations (probabilities) better match between values & choices better match between values & choices Reduce decisional conflict (9 points) Reduce decisional conflict (9 points) Help undecided to decide (50%) Help undecided to decide (50%) Patients 40% less passive in decisions Patients 40% less passive in decisions Reduce over-use Reduce over-use ↓ 25% surgery; ↓ 20% PSA; ↓ 29% HRT ↓ 25% surgery; ↓ 20% PSA; ↓ 29% HRT Potential to reduce under-use Potential to reduce under-use O’Connor et al., Cochrane Library, 2007
 70% more realistic expectations (probabilities) better match between values & choices better match between values & choices Reduce decisional conflict (9 points) Reduce decisional conflict (9 points) Help undecided to decide (50%) Help undecided to decide (50%) Patients 40% less passive in decisions Patients 40% less passive in decisions Reduce over-use Reduce over-use ↓ 25% surgery; ↓ 20% PSA; ↓ 29% HRT ↓ 25% surgery; ↓ 20% PSA; ↓ 29% HRT Potential to reduce under-use Potential to reduce under-use O’Connor et al., Cochrane Library, 2007")
21
Are they cost-effective? A randomized controlled trial measured economic impact of using pt decision aidsA randomized controlled trial measured economic impact of using pt decision aids Hysterectomy for heavy menstrual bleeding:Hysterectomy for heavy menstrual bleeding:

22
Kennedy et al. JAMA 2002; 288: 2701-2708

23
Growth in trials and PtDAs Registered in Cochrane Collaboration’s Inventory

24
How are decision aids available? Paper (pamphlet)Paper (pamphlet) Game boardsGame boards Touch screen monitorsTouch screen monitors VideosVideos CD ROMsCD ROMs InternetInternet
Paper (pamphlet) Game boardsGame boards Touch screen monitorsTouch screen monitors VideosVideos CD ROMsCD ROMs InternetInternet.")
25
Delivery Models 1.Internet [8 million in 2006] 2.Call Center 3.Practice Centers or Shared DM Center
![Delivery Models 1.Internet [8 million in 2006] 2.Call Center 3.Practice Centers or Shared DM Center](http://images.slideplayer.com/10/2727551/slides/slide_25.jpg "Delivery Models 1.Internet [8 million in 2006] 2.Call Center 3.Practice Centers or Shared DM Center")
26
Range of Decision Support Tools PATIENT DOCTOR Information: diagnostic tests: Where to orderWhere to order CostsCosts Tools to assess risk Patient electronic medical record (EMR) Risk self- assessment Information: cancer, risk factors, diagnostic tests MD-pt interaction ?? Patient portals: Tricare personal health journal disease tracking & management tools Clinical trials

28
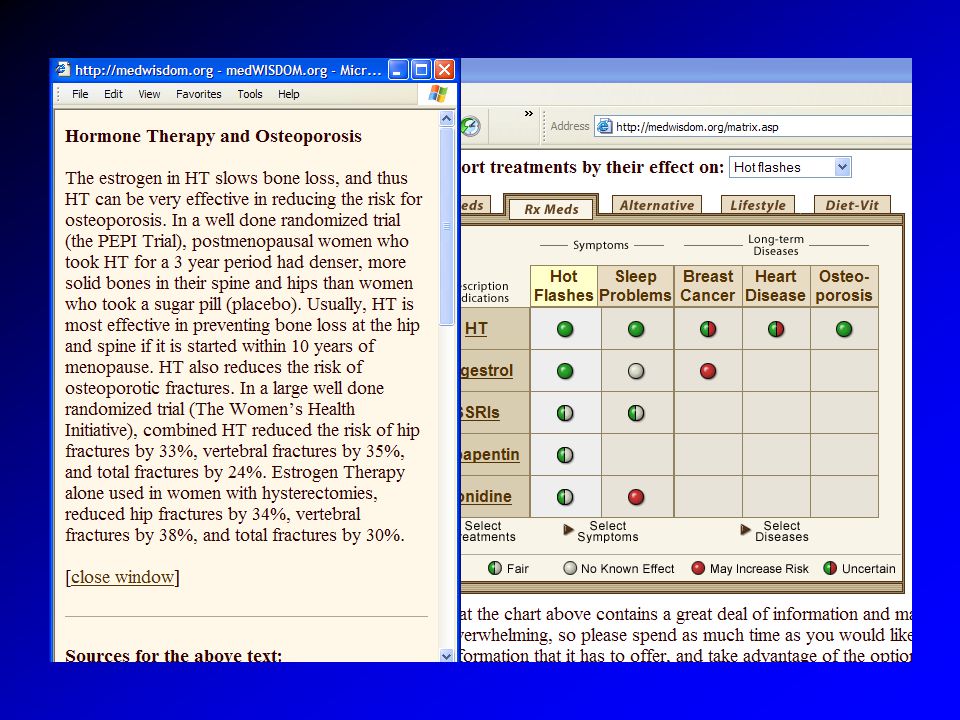
Foundation for Informed Decision Making The Informed Health Care ConsumerThe Informed Health Care Consumer Treatment Choices for Benign Prostatic HyperplasiaTreatment Choices for Benign Prostatic Hyperplasia Treatment Choices for Prostate CancerTreatment Choices for Prostate Cancer Is a PSA Test Right for You?Is a PSA Test Right for You? Treatment Choices for Abnormal Uterine BleedingTreatment Choices for Abnormal Uterine Bleeding Treatment Choices for Uterine FibroidsTreatment Choices for Uterine Fibroids Ovarian Cancer: Reducing Your RisksOvarian Cancer: Reducing Your Risks Early Breast Cancer: Hormone Therapy and ChemotherapyEarly Breast Cancer: Hormone Therapy and Chemotherapy Early Stage Breast Cancer: Choosing Your SurgeryEarly Stage Breast Cancer: Choosing Your Surgery Breast Reconstruction: Is It Right For You?Breast Reconstruction: Is It Right For You? Living with Metastatic Breast CancerLiving with Metastatic Breast Cancer Ductal Carcinoma In Situ: Choosing Your TreatmentDuctal Carcinoma In Situ: Choosing Your Treatment Managing Menopause: Choosing Treatments for Menopause SymptomsManaging Menopause: Choosing Treatments for Menopause Symptoms

29
Ottawa Health Research Institute: www.ohri.ca

30
Fox Chase Cancer Center: http://www.fccc.edu

32
Decision Aid Personal Decision Form

33
GP/Physio screens for surgical eligibilityGP/Physio screens for surgical eligibility –Decision Aid Assess patients’ informed preferenceAssess patients’ informed preference –Patient decision aid –Decision quality

34
Dear Dr. Thank you for the referral. Your patient, ___________________, was assessed at the Orthopaedic Intake Clinic at the Riverside campus of the Ottawa Hospital. We used the following standardized assessment: A. Clinical Assessment of Surgical Eligibility Your patient completed an osteoarthritis specific quality of life measure, the validated WOMAC (Western Ontario McMaster Osteoarthritis Index). Higher scores indicate worse quality of life (threshold for consideration of joint replacement > 39). A physician completed joint replacement assessment tool, HKPT (Hip & Knee Priority Tool) developed and validated for the Western Canada Wait List Project and includes aspects of history, physical examination and X-ray interpretation. Higher scores indicate higher need for joint replacement Your patient self-reported a WOMAC osteoarthritis score of ____/120 and was assigned a HKPT screening score of _______/80. Both forms are attached for your information. Based on this global assessment, your patient meets the criteria for further assessment by an orthopaedic surgeon. B. Assessment of Patients’ Informed Preferences Your patient watched an evidence-based, validated video/DVD patient decision aid on total knee replacement surgery. It describes the options, benefits, risks, and their associated probabilities. It also helps them to clarify the personal importance of benefits versus risks. Your patient completed a decision quality measure eliciting: a) their knowledge of options, benefits, and harms; b) the personal importance they place on benefits versus risks; and c) unresolved decisional needs. The form is appended. After viewing a patient decision aid on total knee replacement surgery, your patient prefers non- operative alternatives at this time and did not want to consider surgery. Other non-operative alternatives to consider include: physiotherapy, bracing_______________; intra- articular cortisone injection; viscosupplementation injections; weight loss Information on these alternatives can be found at www.aaos.org/Research/documents/oainfo_knee.aspwww.aaos.org/Research/documents/oainfo_knee.asp The Ottawa Hospital Orthopaedic Intake Clinic staff would be happy to reassess your patient in 6 months if the condition changes and your patient re-considers having surgery.
. Higher scores indicate worse quality of life (threshold for consideration of joint replacement > 39). A physician completed joint replacement assessment tool, HKPT (Hip & Knee Priority Tool) developed and validated for the Western Canada Wait List Project and includes aspects of history, physical examination and X-ray interpretation. Higher scores indicate higher need for joint replacement Your patient self-reported a WOMAC osteoarthritis score of ____/120 and was assigned a HKPT screening score of _______/80. Both forms are attached for your information. Based on this global assessment, your patient meets the criteria for further assessment by an orthopaedic surgeon. B. Assessment of Patients’ Informed Preferences Your patient watched an evidence-based, validated video/DVD patient decision aid on total knee replacement surgery. It describes the options, benefits, risks, and their associated probabilities. It also helps them to clarify the personal importance of benefits versus risks. Your patient completed a decision quality measure eliciting: a) their knowledge of options, benefits, and harms; b) the personal importance they place on benefits versus risks; and c) unresolved decisional needs. The form is appended. After viewing a patient decision aid on total knee replacement surgery, your patient prefers non- operative alternatives at this time and did not want to consider surgery. Other non-operative alternatives to consider include: physiotherapy, bracing_______________; intra- articular cortisone injection; viscosupplementation injections; weight loss Information on these alternatives can be found at The Ottawa Hospital Orthopaedic Intake Clinic staff would be happy to reassess your patient in 6 months if the condition changes and your patient re-considers having surgery..")
37
Challenges in Counseling Women about Menopause HT: complex benefits versus risksHT: complex benefits versus risks Many other treatments availableMany other treatments available Long-term vs short-term effectsLong-term vs short-term effects Importance of individual riskImportance of individual risk Uncertainty/probabilitiesUncertainty/probabilities Women often harbor other concernsWomen often harbor other concerns Quality of menopausal counseling poorQuality of menopausal counseling poor

38
An Interactive Website Patient-specific decision model translates RCT findings to individual patientsPatient-specific decision model translates RCT findings to individual patients –Applies RR from WHI to individual baseline risks Links decision model to comprehensive database of treatmentsLinks decision model to comprehensive database of treatments Considers major outcomes affected by HT, including relief from menopausal symptomsConsiders major outcomes affected by HT, including relief from menopausal symptoms Col et al: JAMA, AIM, MDM

39
Women’s Interactive System for Decisions on Menopause Purpose:Purpose: –Empower women to make better decisions about menopause –Help clinicians counsel menopausal patients Designed by multidisciplinary teamDesigned by multidisciplinary team Funding: AHRQ R01Funding: AHRQ R01

40
Screen Shots from WISDOM

41
Treatment Options Chart

42
Alternative Treatments

43
Drilling Down to Tailor Amount of Information to Information Needs

45
Drilling Down: References

46
Risk Assessment

47
Personalized Risk Report

49
Clinician Summary

50
Clinician Summary (cont)
")
51
How Patients Use WISDOM Clinic or doctor refers patient to WISDOM (URL and password) before her clinic appointmentClinic or doctor refers patient to WISDOM (URL and password) before her clinic appointment Patient visits WISDOMPatient visits WISDOM –Enters information about her risks, symptoms, and preferences –Explores personalized information about menopause, her symptoms & risks, & treatments Patient sends summary report to her doctorPatient sends summary report to her doctor Clinic appointment to discuss menopauseClinic appointment to discuss menopause Patient uses website as resource after doctor visitPatient uses website as resource after doctor visit
 before her clinic appointmentClinic or doctor refers patient to WISDOM (URL and password) before her clinic appointment Patient visits WISDOMPatient visits WISDOM –Enters information about her risks, symptoms, and preferences –Explores personalized information about menopause, her symptoms & risks, & treatments Patient sends summary report to her doctorPatient sends summary report to her doctor Clinic appointment to discuss menopauseClinic appointment to discuss menopause Patient uses website as resource after doctor visitPatient uses website as resource after doctor visit")
52
The Randomized Trial Evaluated in multi-site RCT (n=200)Evaluated in multi-site RCT (n=200) Intervention: WISDOMIntervention: WISDOM Control: standard careControl: standard care 4 Clinic sites4 Clinic sites Randomization at patient level within each clinicianRandomization at patient level within each clinician –6 control/6 intervention patients per clinician
Evaluated in multi-site RCT (n=200) Intervention: WISDOMIntervention: WISDOM Control: standard careControl: standard care 4 Clinic sites4 Clinic sites Randomization at patient level within each clinicianRandomization at patient level within each clinician –6 control/6 intervention patients per clinician")
53
Outcome Measures Medication UseMedication Use Decisional ConflictDecisional Conflict KnowledgeKnowledge SatisfactionSatisfaction Behavioral changeBehavioral change Quality of counselingQuality of counseling Risk perceptionRisk perception

54
Feedback from Doctors WISDOM…% of positive responses prepared the patient for the visit70% improved the quality of the visit65% improved the way time was spent during the visit60% helped me understand the issues important to my patient80% helped my patient understand treatment risks, benefits75% helped my patient be as involved in the decision making process as she desired 85% helped my patient to make a more informed decision90% affected the patient-physician relationship75% saved time in my clinic visits50% improved the efficiency of my patient consultation55% improved my counseling session on menopause70%

55
Summary WISDOM users:WISDOM users: –Decrease use of HT and MT –Higher use of other prescription meds To treat HTN, depression, insomniaTo treat HTN, depression, insomnia –More likely to try exercise/diet/soy

57
Possible Mechanisms of Action? –WISDOM users more knowledgeable about risks of HT, impact of HT on other conditions –WISDOM users more aware of the benefits of lifestyle improvements –Doctors and patients better able to identify and address critical non- menopausal issues –Doctors and patients are more aware of the patient’s risks and symptoms & better able to prioritize

58
Impact on Decisional Conflict

59
Access to WISDOM URL: www.medwisdom.orgURL: www.medwisdom.org Currently password protectedCurrently password protected –Username: “guest5” –Password: gue5t5

60
Question 4. Would you be interested in using this website if it were free of charge? A. Yes B. No C. Not sure

61
Can Patient-Centered Technology Transform Health Care? Help identify high-risk patientsHelp identify high-risk patients –Facilitate targeted counseling, risk reduction Help PCPs counsel patients about treatmentsHelp PCPs counsel patients about treatments More efficient use of PCP timeMore efficient use of PCP time –Shift time consuming tasks to those better equipped: computers and patients –Technology performs data collection, integration, synthesis, mapping –PCP has more time to address other areas –Less error, less bias

62
QUESTION: 5. What would most prevent you from incorporating Shared Decision Making into your practice? A.Not enough time B.Don’t believe its applicable to characteristics of my patients C.Don’t believe applicable to clinical situation D.Believe it’s not possible to reconcile patient preferences with SDM E.Don’t believe in concept of asking patients about their preferences F.Believe can’t perform SDM G.Don’t understand SDM (lack of familiarity) H.Difficult to find/access the appropriate decision tool at the time when it is needed
 H.Difficult to find/access the appropriate decision tool at the time when it is needed.")
63
QUESTION Would you use DS to help: 6. Choose the best drug for your patient? A.Yes B.No C.Not sure

64
QUESTION Would you use DS to help: 7. Prioritize your patient’s risks for chronic disease? A.Yes B.No C.Not sure

65
QUESTION Would you use DS to help: 8. Identify patient preferences for treatments? A.Yes B.No C.Not sure

66
QUESTION Would you use DS to help: 9. Educate patients about disease self- management? A.Yes B.No C.Not sure

67
QUESTION Would you use DS to help: 10. Patient identify/prioritize what they want to talk about during the clinic visit? A.Yes B.No C.Not sure

68
QUESTION: 11 11. What attribute of DS is most important for you? A.Save time B.Avoid paperwork C.Prepare patients for visit D.Educate patient after the visit E.Help set priorities for the clinic visit F.Reduce liability G.Simplify counseling

69
QUESTION 12. Would you be interested in training in shared decision making? A.Yes B.No C.Not sure

70
QUESTION 13. If you were aware of your patients top 2-3 health concerns just before they walked in the door, would that help you? A.Yes B.No C.Not sure

71
Legal standard: informed patient choice

72
How long before it will be unethical to ask a patient to consent to treatment without using a decision aid? I predict it will not be long—despite the time needed to use aids and the limited availability of good ones. The Ottawa Health Decision Centre is working on this. … it provides a list of decision aids, each scored for quality against an international standard (http://decisionaid.ohri.ca).http://decisionaid.ohri.ca

73
Washington State New Legislation Bill 5930 (May 2007) An act relating to providing high quality, affordable healthcare to Washingtonians based on the recommendations of the blue ribbon commission on health care costs and access if a patient/delegate signs an acknowledgement of shared decision making, such acknowledgement shall constitute evidence that the patient gave his or her informed consent to the treatment administeredif a patient/delegate signs an acknowledgement of shared decision making, such acknowledgement shall constitute evidence that the patient gave his or her informed consent to the treatment administered Acknowledgement of SDM includes:Acknowledgement of SDM includes: –Statement that patient and health care provider have engaged in SDM –Brief description of the services the patient and provider have jointly have agreed to –Brief description of the patient decision aid used –Statement that patient understands risks or seriousness of disease, available treatment alternatives (including non-tx), risks, benefits and uncertainties of treatment alternatives –Statement that patient had opportunity to ask the provider questions and have questions answered to patients’ satisfaction SDM Def’n: process in which the physician or other health care practitioner discusses with the patient or his/her representative the information specified above with the use of a patient decision aid and the patient shares with the provider such relevant personal info as might make one treatment or side effect more or less tolerable than othersSDM Def’n: process in which the physician or other health care practitioner discusses with the patient or his/her representative the information specified above with the use of a patient decision aid and the patient shares with the provider such relevant personal info as might make one treatment or side effect more or less tolerable than others
 An act relating to providing high quality, affordable healthcare to Washingtonians based on the recommendations of the blue ribbon commission on health care costs and access if a patient/delegate signs an acknowledgement of shared decision making, such acknowledgement shall constitute evidence that the patient gave his or her informed consent to the treatment administeredif a patient/delegate signs an acknowledgement of shared decision making, such acknowledgement shall constitute evidence that the patient gave his or her informed consent to the treatment administered Acknowledgement of SDM includes:Acknowledgement of SDM includes: –Statement that patient and health care provider have engaged in SDM –Brief description of the services the patient and provider have jointly have agreed to –Brief description of the patient decision aid used –Statement that patient understands risks or seriousness of disease, available treatment alternatives (including non-tx), risks, benefits and uncertainties of treatment alternatives –Statement that patient had opportunity to ask the provider questions and have questions answered to patients’ satisfaction SDM Def’n: process in which the physician or other health care practitioner discusses with the patient or his/her representative the information specified above with the use of a patient decision aid and the patient shares with the provider such relevant personal info as might make one treatment or side effect more or less tolerable than othersSDM Def’n: process in which the physician or other health care practitioner discusses with the patient or his/her representative the information specified above with the use of a patient decision aid and the patient shares with the provider such relevant personal info as might make one treatment or side effect more or less tolerable than others")
74
QUESTION 14 Choose the statement that is most like you A. It is easy for me to become emotionally close to others. I am comfortable depending on others and having others depend on me. I don't worry about being alone or having others not accept me. B. I am comfortable without close relationships. It is very important to me to feel independent and self-sufficient, and I prefer not to depend on others or have others depend on me. C. I want to be completely emotionally intimate with others, but I often find that others are reluctant to get as close as I would like. I am uncomfortable being without close relationships, but I sometimes worry that others don't value me as much as I value them. D. I am uncomfortable getting close to others. I want emotionally close relationships, but I find it difficult to trust others completely, or to depend on them. I worry that I will be hurt if I allow myself to become too close to others.

75
THANK YOU

76
Design of Randomized Trial 1,450 women notified 300 (21%) responded 67 excluded 7 had breast cancer or heart disease 58 returned packet too late 2 failed to participate 233 randomized WISDOM (117) 107 (91%) returned 2-wk survey Control (116 ) 111 (96%) returned 2-wk survey
 responded 67 excluded 7 had breast cancer or heart disease 58 returned packet too late 2 failed to participate 233 randomized WISDOM (117) 107 (91%) returned 2-wk survey Control (116 ) 111 (96%) returned 2-wk survey")
Similar presentations















>")









