Download presentation
Presentation is loading. Please wait.

1
Exception from Informed Consent for Research in Emergency Settings Marilyn Morris MD, MPH Susan S. Fish, PharmD, MPH

2
Historical Context Regulations and Responsibilities Ethical Gaps and Public Perceptions Defining “community” EFIC in the inpatient setting

3
Historical Framework

4
1949: The Nuremberg Code “The voluntary consent of the human subject is absolutely essential.”

5
Helsinki, Finland, 1964 latest revision, 2000 Emergency research is permissible “…only if the condition that prevents obtaining consent is a necessary characteristic of the research population.” “Consent to remain in the research should be obtained as soon as possible from the individual or a legally authorized surrogate.”

6
The Belmont Report: 1979 Basic ethical principles –Respect for Persons (autonomy) –Beneficence –Justice Minimal risk standard for research without informed consent Potential for surrogate consent
 –Beneficence –Justice Minimal risk standard for research without informed consent Potential for surrogate consent")
7
January 1981 Code of Federal Regulations –Largely based on the Belmont Report –Allows a waiver of informed consent for minimal risk research in emergency settings –No specific mechanism for emergency research posing more than minimal risk

8
Deferred Consent “Is it ok if I borrow your car yesterday?” Brain Resuscitation Clinical Trials 1993: Dear Colleague Letter

9
(J. Am. Med. Assoc. 273, 1283–1287; JAMA April 1995

10
THE FINAL RULE, IRB AND INVESTIGATOR RESPONSIBILITIES

11
Exception from Informed Consent Requirements in Emergency Research 21 CFR 50.24 and 45 CFR 46.101(i) (A) IRB with concurring physician finds and documents 1. Life threatening situation with unproven or unsatisfactory treatment and research is necessary 2. Obtaining informed consent is not feasible 3. Participation in research has prospect of direct benefit because: i. Situation necessitates intervention ii. Science supports potential of direct benefit iii. Risks are reasonable compared to medical condition, risks and benefits of standard therapy, and risks and benefits of proposed intervention

12
4. Research could not practicably be done without waiver 5. Potential therapeutic window is short; attempt to contact subject’s legal representative when possible 6. IRB approves consent procedures and document for subject or legal representative, if feasible; also approves procedures and information for family member Exception from Informed Consent Requirements in Emergency Research 21 CFR 50.24 and 45 CFR 46.101(i)
.")
13
7. Additional protections i. Community consultation ii. Public disclosure prior to study initiation iii. Public disclosure after study completion iv. Independent data monitoring committee v. Attempt to contact family member when possible Exception from Informed Consent Requirements in Emergency Research 21 CFR 50.24 and 45 CFR 46.101(i)
.")
14
Exception from Informed Consent Requirements in Emergency Research 21 CFR 50.24 and 45 CFR 46.101(i) (B)Information provided to subject, legal representative, and/or family as soon as possible (C) IRB documentation kept for at least 3 years * (D) Separate IND/IDE * (E) If IRB does not approve waiver, documentation of reasons to be shared with sponsor, FDA, other researchers, other IRBs * (*FDA regulations only)
 (B)Information provided to subject, legal representative, and/or family as soon as possible (C) IRB documentation kept for at least 3 years * (D) Separate IND/IDE * (E) If IRB does not approve waiver, documentation of reasons to be shared with sponsor, FDA, other researchers, other IRBs * (*FDA regulations only)")
15
IRB RESPONSIBILITIES 21 CFR 50.24 and 45 CFR 46.101(i) 1.Determine if FDA or HHS regulations apply 2.Know state law - is waiver of consent possible? 3. Find and document that criteria are met 4. Determine consent procedures a. Window of opportunity/therapeutic window b. Procedures for attempts at consent c. Advanced directives policy ) 5. Assess possibility of prospective consent (practicability)
 5. Assess possibility of prospective consent (practicability).")
16
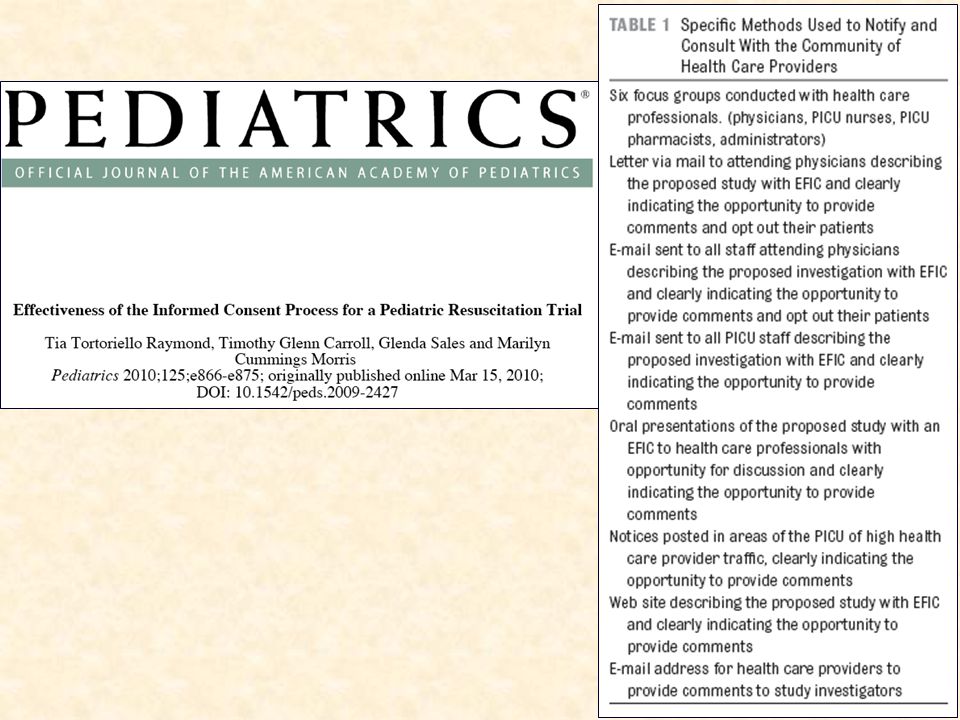
IRB RESPONSIBILITIES 21 CFR 50.24 and 45 CFR 46.101(i) 6. Provide opportunity for community consultation; use results to advise IRB deliberations 7. Assure implementation of public disclosure by investigator; assess adequacy of efforts 8. Consider advice from DMC 9. Ensure information is given to subject, representative, family as soon as appropriate 10. Keep records at least 3 years 11. Document and share deliberations if study not approved

17
INVESTIGATOR RESPONSIBILITIES 21 CFR 50.24 and 45 CFR 46.101(i) 1. Identify how criteria are met a. Life threatening situation b. Clinical equipoise exists c. This research is needed now (basic science and animal work are supportive) d. Consent is not feasible e. Benefit:Risk assessment f. Study with consent not practicable
 d. Consent is not feasible e. Benefit:Risk assessment f. Study with consent not practicable.")
18
INVESTIGATOR RESPONSIBILITIES 21 CFR 50.24 and 45 CFR 46.101(i) 2. Document in protocol a. Therapeutic window b. How to attempt consent 3.Write documents a. Informed consent form b. Information form

19
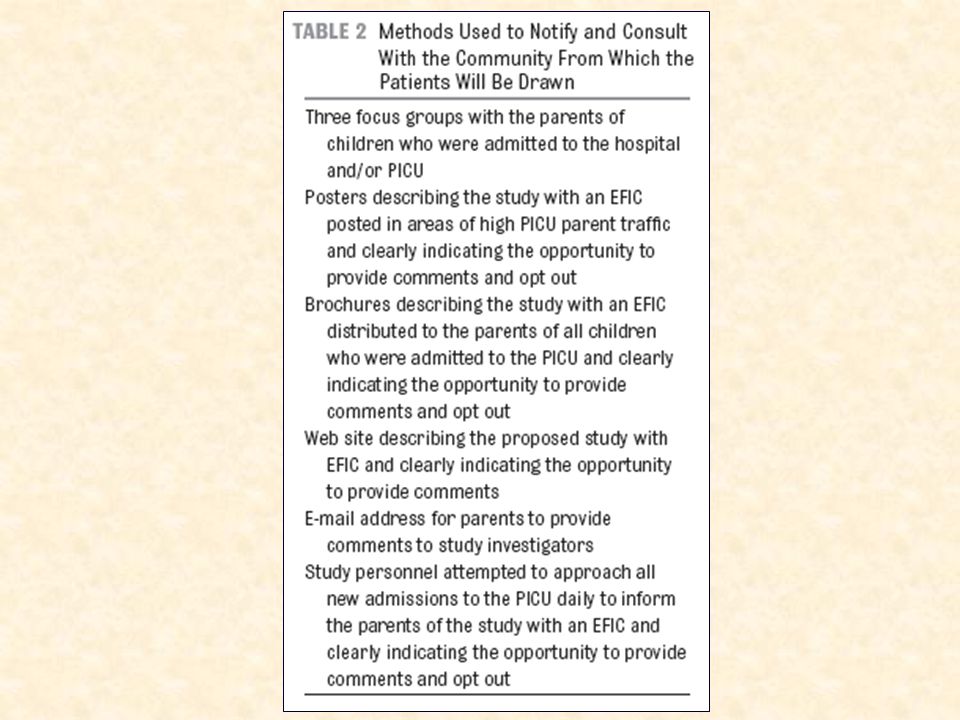
INVESTIGATOR RESPONSIBILITIES 21 CFR 50.24 and 45 CFR 46.101(i) 4. Define (in conjunction with IRB) a. Community b. Methods of community consultation c. Methods of public disclosure 5. Submit/obtain IND/IDE (FDA regulations only) 6. Submit information for continuing review 7. Provide data to DMC 8. Inform subject, representative, family
 a. Community b. Methods of community consultation c. Methods of public disclosure 5. Submit/obtain IND/IDE (FDA regulations only) 6. Submit information for continuing review 7. Provide data to DMC 8. Inform subject, representative, family.")
20
What do people think of EFIC? It depends who (and how) you ask.
 you ask.")
21
Nov 15, 1996 “The Return of Joseph Mengele” “The Food and Drug Administration (FDA) this month reversed 50 years of medical ethics by freeing researchers to experiment on patients without consent. New and improved life-saving therapies supposedly will result. But nothing is gained if the most basic of human rights is the price of progress.”

22
April 22, 2002

23
VOICES Focus groups, 25 women, 17 men Drawn from NYC communities in which the PAD trial took place Resistance to the need for EFIC Disconnect between theory and specific examples. Richardson 2008

24
Biros 2009 Survey of 1901 people at a “popular public venue”

25
Survey of 530 people in ER waiting room 49% believed enrolling patients without prior consent in an emergency situation would be acceptable 70% would not object to be entered into such a study without providing prospective informed consent. McClure 2003

26
Survivors of SCD Dickert 2009

27
“Would you ask that your child be excluded?” 10%43% p < 0.01 Paragraph format Bullet format

28
Random Digit Dialing Used in proposed hypertonic resuscitation fluid study (Bulger 2009)
")
29
WHAT IS A COMMUNITY FOR THE PURPOSES OF EFIC RESEARCH?

30
Community Consultation …consultation (including, where appropriate, consultation carried out by the IRB) with representatives of the communities in which the research will be conducted and from which the subjects will be drawn;
 with representatives of the communities in which the research will be conducted and from which the subjects will be drawn;")
31
Federal Register: 9/21/95 The proposed rule recognizes that subjects who are candidates for emergency research will not meet the condition of being fully competent. In many cases, they will be totally incompetent. Such potential subjects, if they are to be enrolled in research, must be provided with special additional protections. The special protections proposed in this rule for subjects of emergency research include prior FDA and community consultation on the research, public disclosure, and careful mandatory oversight of the welfare of subjects by a data and safety monitoring board.

32
com·mu·ni·ty a unified body of individuals: a : state, commonwealth b : the people with common interests living in a particular area; broadly : the area itself c : an interacting population of various kinds of individuals (as species) in a common location d : a group of people with a common characteristic or interest living together within a larger society e : a group linked by a common policy f : a body of persons or nations having a common history or common social, economic, and political interests g : a body of persons of common and especially professional interests scattered through a larger society Merriam- Webster.com
 in a common location d : a group of people with a common characteristic or interest living together within a larger society e : a group linked by a common policy f : a body of persons or nations having a common history or common social, economic, and political interests g : a body of persons of common and especially professional interests scattered through a larger society Merriam- Webster.com")
33
Merchant RM, Rubright JD, Pryor HP, Karlawish JHT.

34
EFIC in the inpatient setting

35
What constitutes impracticability? – To what extent is prospective consent possible? Who comprises the community? – Setting specific rather than geographic? – Who are the community leaders?

36
Themes from an inpatient community consultation Pre-consent –Burden on families –Validity of consent Need for some communication Importance of verbal over written communication Discomfort with randomization Discomfort with “control” arm

37
The inpatient community Parents of children hospitalized in an intensive care unit – 91/91 reported that parents of critically ill children represent the most important community – 75/91 (82%) felt that the inpatient community represents the entire relevant community Morris 2006
 felt that the inpatient community represents the entire relevant community Morris 2006")
38
Trial of a brochure to inform parents of an ongoing EFIC trial

39
“Is this a good way to communicate with parents about a research study?”

40
“Would you have read this if someone gave it to you when your child was admitted?”

41
“Do you think this study should take place?”

46
Evaluation of Public Disclosure 75/93 parents interviewed were aware of the study 76/93 remembered seeing the brochure – 26% did not read, – 39% read quickly, and – 35% read carefully 37/93 remembered seeing the poster – 51% did not read, – 32% read quickly, and – 17% read carefully

47
Evaluation of Public Disclosure Would you want your child to participate in the study? – 67% yes – 9% no – 24% undecided. Of the 7 parents who did not want to participate, 3 had opted out and 4 were unaware that they could opt out.

48
“Let us not forget that progress is an optional goal, not an unconditional commitment.... Let us also remember that a slower progress in the conquest of disease would not threaten society, grievous as it is to those who have to deplore that their particular disease be not conquered, but that society would indeed be threatened by the erosion of those moral values whose loss, possibly caused by too ruthless a pursuit of scientific progress, would make its most dazzling triumphs not worth having.” -Hans Jonas

49
RESOURCES REGULATIONS: www.fda.gov GUIDANCE: www.fda.gov IMPLEMENTATION: Biros MH, Fish SS, Lewis RJ. Acad Emerg Med 1999;6:1272- 1282. (www.aemj.org)

53
SUMMARY Rare use Important research Vulnerable population Special protections Respect for persons

Similar presentations





 is a review committee established to help protect the rights and welfare of human research subjects.>")




>")
 593-5468>")








>")



