Download presentation
Presentation is loading. Please wait.

1
Acute Tonsillopharyngitis
Dr Rajesh 16/04/08

2
Definitions tonsillitis: inflammation of pharyngeal tonsils
tonsillopharyngitis: inflammation extending from tonsils to the adenoids and lingual tonsils recurrent tonsillitis: 7 episodes in 1 year, 5 infections in 2 consecutive years, or 3 infections each year for 3 years consecutively chronic tonsillitis: chronic sore throat, halitosis, tonsillitis, and persistent tender cervical nodes for greater than 4 weeks quinsy: Greek term used for inflammation of throat and tonsils, historically used for peritonsillar abscess

3
Epidemiology most cases occur in school-age children
uncommon in the first 2 years of life 5-7 URIs per child per year GAS is found in 35% of children with pharyngitis 45,000 cases of PTA per year or 30 cases per 100,000 people per year

4
Causes of Tonsillopharyngitis
• Beta hemolytic streptococcal infection — 22 percent • Mycoplasma pneumoniae — 9.4 percent • Chlamydia species strain TWAR — 8.4 percent • Viruses — 25.5 percent Huovinen, et al 1995

6
CLINICAL DIAGNOSIS The "classic" presentation of GAS tonsillopharyngitis is a sore throat associated with fever, tonsillopharyngeal erythema and exudate, swollen and tender anterior cervical adenopathy, and an elevated white blood cell (WBC) count without rhinorrhea or cough. However, even when this constellation of clinical symptoms is present, the likelihood of GAS infection does not exceed 60 to 70 percent in children, and 20 to 30 percent in adults. Tonsillopharyngitis due to GAS cannot be clinically diagnosed with accuracy in most patients [5,6,7,8,9,10].
 count without rhinorrhea or cough. However, even when this constellation of clinical symptoms is present, the likelihood of GAS infection does not exceed 60 to 70 percent in children, and 20 to 30 percent in adults. Tonsillopharyngitis due to GAS cannot be clinically diagnosed with accuracy in most patients [5,6,7,8,9,10].")
7
Is it truly Group A beta hemolytic Streptoccal tonsillopharyngitis?
From many studies, it would appear that the presence or absence of a GAS pharyngitis cannot be accurately diagnosed with clinical examination alone in most patients. It is somewhat easier to identify a subset of children (approximately 20 percent of cases) and adults (approximately 67 percent of cases) who are unlikely to have GAS. These patients have sore throats with accompanying rhinorrhea, cough, and hoarseness. Fever is often absent. They have mild tonsillopharyngeal erythema without exudate, and slight or no cervical lymphadenitis. It has been suggested that the throat culture is not reproducible in some cases, perhaps explaining the occurrence of both false positive and negative results. However, discordance is actually quite uncommon, occurring in only 1 to 10 percent of cases. As an example, in a study in which three simultaneous throat cultures were obtained in consecutive patients between the ages of 2 and 20 years, concordance of positive or negative culture on all three swabs was seen in 102 of 103 (99 percent) patients [15]. False positive throat cultures usually are due to the misclassification as GAS of other beta-hemolytic organisms including streptococci (groups B, C, F, or G) or Staphylococcus aureus. The overall incidence of false positive cultures is less than 5 percent but can exceed 50 percent during an epidemic of group C streptococcal infection in a college setting. The bacitracin disk sensitivity test is used to make a presumptive identification of GAS: 95 to 100 percent of GAS have a zone of inhibition around the disk (0.04 units of bacitracin), while 83 to 97 percent of non-GAS do not exhibit inhibition [16]. As long as there are sufficient numbers of GAS in the area of the disk, the test can be interpreted on a primary blood agar plate. Between 3.6 and 17 percent of children with a sore throat develop an antibody rise to GAS antigens despite negative throat cultures [17,18]; there are no corresponding data in adults but the rate is likely to be much lower. Explanations for false negative throat cultures include: • Poor culture technique • Occult antibiotic therapy • Faulty bacteriology practices These patients most likely have a sore throat as part of a viral upper respiratory infection and do not require a diagnostic test or treatment.
 and adults (approximately 67 percent of cases) who are unlikely to have GAS. These patients have sore throats with accompanying rhinorrhea, cough, and hoarseness. Fever is often absent. They have mild tonsillopharyngeal erythema without exudate, and slight or no cervical lymphadenitis. It has been suggested that the throat culture is not reproducible in some cases, perhaps explaining the occurrence of both false positive and negative results. However, discordance is actually quite uncommon, occurring in only 1 to 10 percent of cases. As an example, in a study in which three simultaneous throat cultures were obtained in consecutive patients between the ages of 2 and 20 years, concordance of positive or negative culture on all three swabs was seen in 102 of 103 (99 percent) patients [15]. False positive throat cultures usually are due to the misclassification as GAS of other beta-hemolytic organisms including streptococci (groups B, C, F, or G) or Staphylococcus aureus. The overall incidence of false positive cultures is less than 5 percent but can exceed 50 percent during an epidemic of group C streptococcal infection in a college setting. The bacitracin disk sensitivity test is used to make a presumptive identification of GAS: 95 to 100 percent of GAS have a zone of inhibition around the disk (0.04 units of bacitracin), while 83 to 97 percent of non-GAS do not exhibit inhibition [16]. As long as there are sufficient numbers of GAS in the area of the disk, the test can be interpreted on a primary blood agar plate. Between 3.6 and 17 percent of children with a sore throat develop an antibody rise to GAS antigens despite negative throat cultures [17,18]; there are no corresponding data in adults but the rate is likely to be much lower. Explanations for false negative throat cultures include: • Poor culture technique • Occult antibiotic therapy • Faulty bacteriology practices. These patients most likely have a sore throat as part of a viral upper respiratory infection and do not require a diagnostic test or treatment.")
8
Why antibiotics Treatment of GABHS pharyngitis is important
To prevent complications of infection, particularly rheumatic fever suppurative complications To speed recovery To prevent spread of the infection

9
Treatment approach based on clinical findings (Komarof, et al)
• Empirically treat patients with the constellation of a tonsillar exudate, tender cervical adenopathy, and a temperature >37.8º C. • Obtain throat cultures in patients with only one or two of the above findings and treat based upon those results. • Do not obtain cultures or treat patients with none of the above findings.

10
The nonsuppurative complications of GAS tonsillopharyngitis
Acute rheumatic fever Scarlet fever Streptococcal toxic shock syndrome Acute glomerulonephritis PANDAS (Pediatric Autoimmune Neuropsychiatric Disorder Associated with Group A Streptococci)
")
11
Suppurative complications
Tonsillopharyngeal cellulitis or abscess Otitis media Sinusitis Necrotizing fasciitis

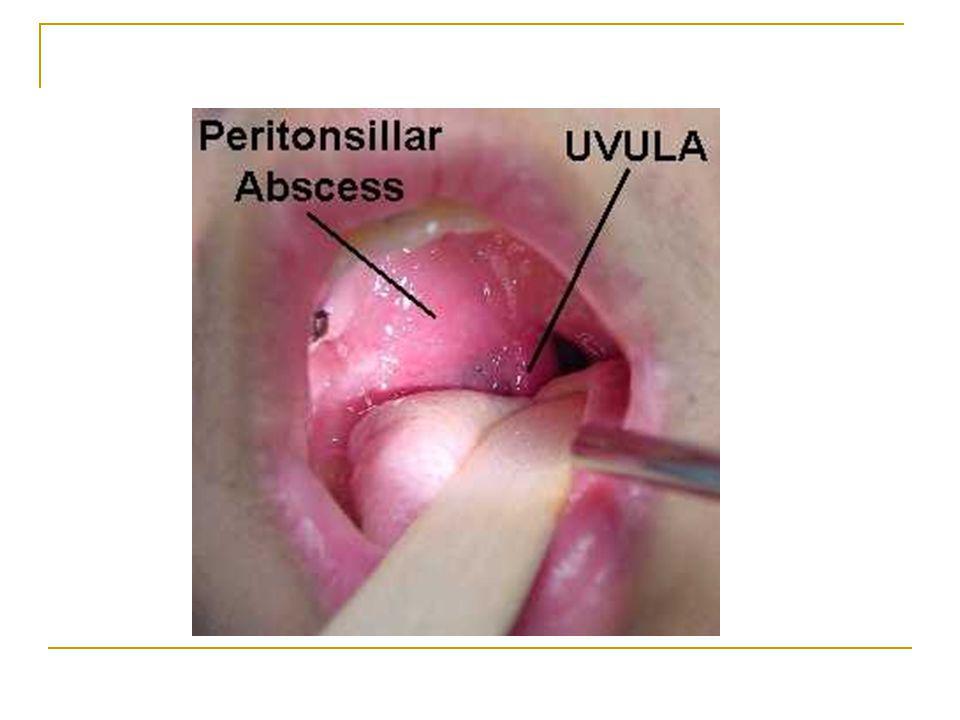
16
Peritonsillar abscess

17
Mononucleosis epstein-barr virus (EBV
indolent onset, gray tonsillar exudate, tender cervical, axillary and/or inguinal lymphadenopathy, low grade fever, weight loss, myalgias, fatigue, hepatosplenomegaly atypical lymphocytes in peripheral smear positive monospot or heterophil Ab test rash with penicillin illness lasts more than 7-10 days

18
Intraoral Ultrasound highly accurate ultrasound
can exclude peritonsillar cellulitis, abscess and retropharyngeal abscess determination of abscess volume, location and relationship to carotid artery

19
CT neck with contrast indications: spread to deep neck structures
inferior pole abscess high risk for drainage procedures (coagulopathy) to guide drainage of PTA after unsuccessful surgical attempt patient unable to open mouth due to trismus
 to guide drainage of PTA after unsuccessful surgical attempt. patient unable to open mouth due to trismus.")
20
complicated PTA with rupture into carotid space

21
Airway Obstruction nasal airway humidified oxygen corticosteroids
monitored observation intubation cricothyroidotomy tracheostomy

22
Recommendations on the Management of Acute and Chronic Tonsillitis
Adequate supportive care Use of analgesics, oral anesthetics, and antiseptics Antibiotics

23
Antibiotics Penicillins Cephalosporins Macrolides

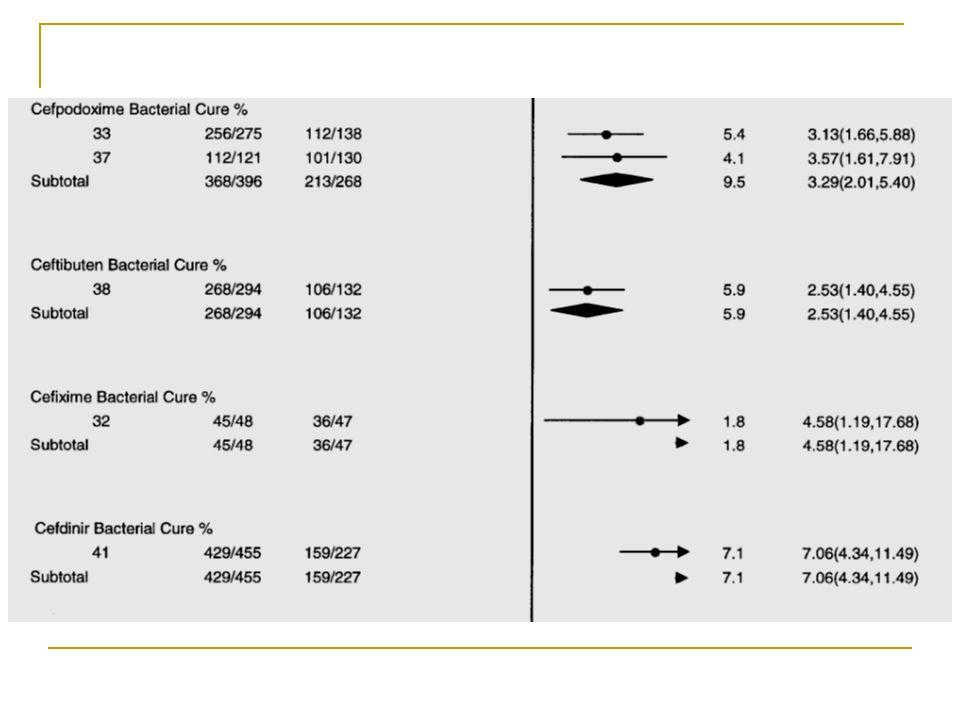
25
Bacteriological cure

28
in the AHA guidelines, prevention of
rheumatic fever as a poststreptococcal complication depends on eradication of GABHS bacteria from the pharynx prevention of rheumatic fever and other nonsuppurative complications of GABHS pharyngitis still occurs when antibacterial therapy is postponed by as many as 9 days after the onset of pharyngitis symptoms

29
Factors influencing antibiotic choice
ability to eradicate GABHS bacteria from the pharynx Ability to resolve signs and symptoms of the infection (bacteriologic and clinical efficacy) adherence (frequency of daily administration, duration of therapy, and palatability), Antibacterial spectrum (narrow versus broad activity), potential treatment-related side effects cost.
 adherence (frequency of daily administration, duration of therapy, and palatability), Antibacterial spectrum (narrow versus broad activity), potential treatment-related side effects. cost.")
30
Cephalosporins

32
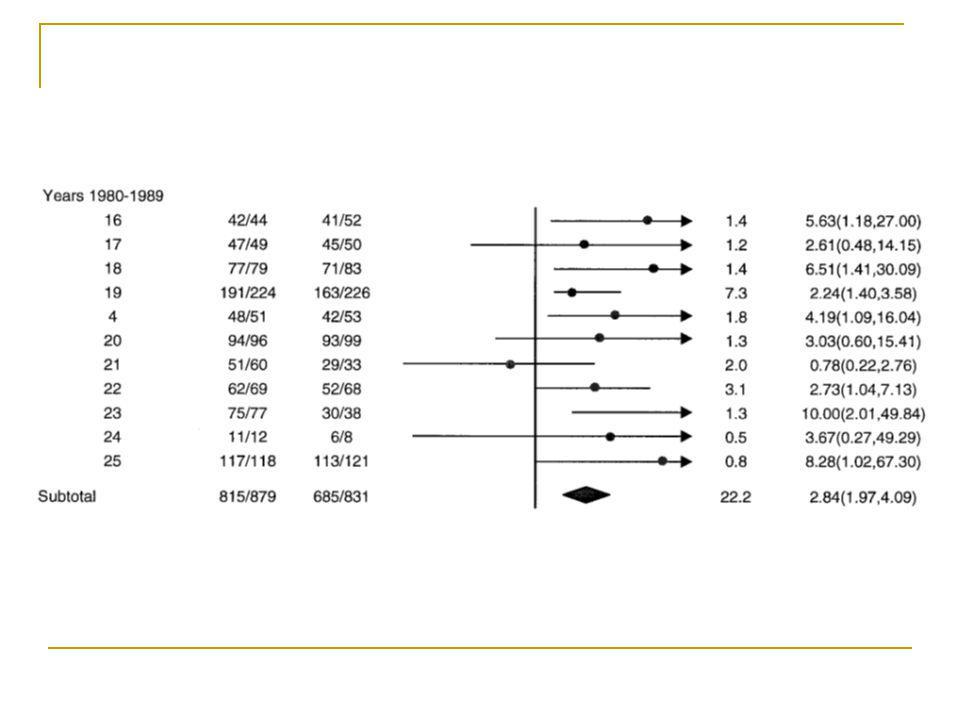
Changing pattern of penicillin sensitivity

35
Clinical cure

39
Short course therapy of AT
Cephalopsorin Azithromycin

41
Clinical pediatrics

42
Penicillin Resistance: Mechanism
It is important to note that no strains of GABHS resistant to penicillin or cephalosporin have ever been reported. Copathogenicity is the most likely explanation for the increasing rate of penicillin treatment failures GABHS susceptible to penicillin are protected by other in vivo, colocalized bacteria that lack the same susceptibility due to beta-lactamase production beta-lactamase producing organisms is more likely to inactivate penicillin

43
Recurrence risk Symptomatic bacteriologic recurrence within 30 days of initial diagnosis occurred in 37% of patients treated with penicillin V, 25% of patients treated with amoxicillin, 18% of patients treated with cephalexin or cefadroxil, 7% of patients treated with amoxicillin-clavulanate or a second-generation or third-generation cephalosporin

44
Children Less Than Three-Years-Old With Pharyngitis Are Group A Streptococci Really That Uncommon Clinical pediatrice , 1986 During a 15-month period, 148 infants and children less than 3-years-old who presented with signs and/or symptoms of pharyngitis were monitored in a private pediatric practice. Clinical signs included fever (95 or 64%), tonsillar exudate (16 or 11%), and cervical adenopathy (5 or 3%). Beta-hemolytic streptococci (BHS) from group A were isolated from throat swabs in 37 (25%) instances. These isolations were more common among children months old than among children less than 2 years old (35% vs. 19%, p < 0.05), and were significantly more likely when overnight anaerobic culture techniques were used rather than conventional aerobic methods (23 % vs. 11%, p < 0.01).
, tonsillar exudate (16 or 11%), and cervical adenopathy (5 or 3%). Beta-hemolytic streptococci (BHS) from group A were isolated from throat swabs in 37 (25%) instances. These isolations were more common among children months old than among. children less than 2 years old (35% vs. 19%, p < 0.05), and were significantly more likely when. overnight anaerobic culture techniques were used rather than conventional aerobic methods (23 % vs. 11%, p < 0.01).")
45
Recurrent tonsillitis
Recurrent tonsillitis is diagnosed when an individual has 7 episodes in 1 year, 5 infections in 2 consecutive years, or 3 infections each year for 3 years consecutively.

46
Microbiology of recurrent tonsillitis
A polymicrobial flora consisting of both aerobic and anaerobic bacteria is observed in core tonsillar cultures from cases of recurrent pharyngitis. Streptococcus pneumoniae, Staphylococcus aureus, and Haemophilus influenzae are the most common bacteria isolated in recurrent tonsillitis. Bacteroides fragilis is the most common anaerobic bacterium isolated in recurrent tonsillitis. A polymicrobial bacterial population is observed in most cases of chronic tonsillitis, with alpha- and beta-hemolytic streptococcal species, S aureus, H influenzae, and Bacteroides species identified. One study, based on bacteriology of the tonsillar surface and core in 30 children undergoing tonsillectomy, suggests that antibiotics prescribed 6 months before surgery do not alter the tonsillar bacteriology at the time of tonsillectomy.7 A relationship between tonsillar size and chronic bacterial tonsillitis is believed to exist. This relationship is based on both the aerobic bacterial load and the absolute number of B and T lymphocytes. H influenzae is the bacterium most often isolated in hypertrophic tonsils and adenoids. With regard to penicillin resistance or beta-lactamase production, the microbiology of tonsils removed from patients with recurrent GABHS pharyngitis is not significantly different from the microbiology of tonsils removed from patients with tonsillar hypertrophy.

47
Treatment for recurent / chronic tonsillitis
Clindamycin: mg/kg PO divided tid for 10 d not to exceed 300 mg/dose + Rifampin: 10 mg/kg/dose bid for 4 days Amoxy-clav for 4-6 weeks

48
Prophylaxis (5 strep infections in 6 months)
Penicillin V Potassium (Kaypen)40 mg/kg/day PO bid, max 3 gm/day
40 mg/kg/day PO bid, max 3 gm/day.")
49
Tonsillectomy: Absolute Indications
Tonsillar hypertrophy causing obstruction to respiration or deglutition Obstructive sleep apnea

50
Relative Indications Chronic tonsillitis
Tonsillitis resulting in febrile convulsions Peritonsillar abscess Diphteria carrier Suspected tonsillar malignancy Hypertrophy causing malocclusion Failure to thrive Systemic disease secondary to Beta hemolytic streptococcal infection Chronic halitosis

Similar presentations















 Lawrence Pike.>")












>")


