Download presentation
Presentation is loading. Please wait.

1
Kulić M., Mujičić E., Šošević A., Gorani D.*, Tahirović E., Spužić M.
PROLONGED SPASM OF THE LEFT ANTERIOR DESCENDING CORONARY ARTERY (case report) Kulić M., Mujičić E., Šošević A., Gorani D.*, Tahirović E., Spužić M. Heart center, KCU Sarajevo Cardiology Clinic, KC Priština* 5th Congress of Cardiologists and Angiologists of Bosnia and Herzegovina Sarajevo, May, 2010,.Hotel Radon Plaza
 Kulić M., Mujičić E., Šošević A., Gorani D.*, Tahirović E., Spužić M. Heart center, KCU Sarajevo. Cardiology Clinic, KC Priština* 5th Congress of Cardiologists and Angiologists of Bosnia and Herzegovina Sarajevo, May, 2010,.Hotel Radon Plaza.")
2
SPASM OF THE CORONARY ARTERY
Definition Pathophysiology Frequency Treatment Case report Conclusion Kulić M, Mujičić E, Šošević A et al. Prolonged spasm of the LAD

3
Kulić M, Mujičić E, Šošević A et al. Prolonged spasm of the LAD
DEFINITION In 1959, Prinzmetal et al described a syndrome of chest pain at rest associated with ST-segment elevation In 1959, Prinzmetal et al described a syndrome of chest pain at rest secondary to myocardial ischemia associated with ST-segment elevation.1 Exercise tolerance was characteristically normal in these individuals, who experienced a cyclical pain pattern with most episodes occurring in the early morning hours. This syndrome, known as Prinzmetal or variant angina, is due to focal coronary artery vasospasm and may be associated with acute myocardial infarction (MI), serious ventricular arrhythmias, and sudden death. Kulić M, Mujičić E, Šošević A et al. Prolonged spasm of the LAD
, serious ventricular arrhythmias, and sudden death. Kulić M, Mujičić E, Šošević A et al. Prolonged spasm of the LAD.")
4
Kulić M, Mujičić E, Šošević A et al. Prolonged spasm of the LAD
PATHOPHYSIOLOGY Coronary spasm is caused primarily by vascular smooth muscle cell hypercontraction Prinzmetal angina is caused by focal coronary artery vasospasm, and a generalized abnormality of coronary artery vasomotor reactivity is not present. Focal coronary artery spasm typically occurs at the site of or adjacent to a fixed stenosis. A substantial number of patients have seemingly normal coronary angiogram results, many within this subgroup have evidence of early atherosclerosis demonstrated by intravascular ultrasonographic examination Kulić M, Mujičić E, Šošević A et al. Prolonged spasm of the LAD

5
Kulić M, Mujičić E, Šošević A et al. Prolonged spasm of the LAD
PATHOPHYSIOLOGY Abnormalities of NO production Activated platelets - releases thromboxane A2 Low levels of intracellular magnesium and vitamin E as well. Hyperinsulinemia and insulin resistance are probable risk factors for variant angina Activated platelets are responsible for the release of several potent vasoconstrictors, including thromboxane A2. Abnormalities of nitric oxide synthase and reduced bioavailability of nitric oxide may result in increased basal vascular tone, vasoconstriction, vasospasm, and in activation, adhesion, and aggregation of platelets with release of additional vasoconstrictors. Elevated serum low-density lipoprotein (LDL) cholesterol, especially the oxidized form of this lipid moiety, is responsible for the decreased production of nitric oxide due to down-regulation of endogenous nitric oxide synthase and the oxidative inactivation of nitric oxide by oxygen free radicals Kulić M, Mujičić E, Šošević A et al. Prolonged spasm of the LAD
 cholesterol, especially the oxidized form of this lipid moiety, is responsible for the decreased production of nitric oxide due to down-regulation of endogenous nitric oxide synthase and the oxidative inactivation of nitric oxide by oxygen free radicals. Kulić M, Mujičić E, Šošević A et al. Prolonged spasm of the LAD.")
6
Kulić M, Mujičić E, Šošević A et al. Prolonged spasm of the LAD
FREQUENCY 2-3% of all patients undergoing diagnostic cardiac catheterization in the USA In Italy, the incidence of variant angina is approximately 10%. A Japanese type of variant angina (termed vasospastic angina) with 20-30% of patients who undergo coronary angiography. Estimates are that 2-3% of all patients undergoing diagnostic cardiac catheterization for chest pain in the United States will subsequently be classified as having variant angina. In Italy, where rigorous inpatient electrocardiographic monitoring is frequently used, the incidence of variant angina in patients admitted with chest pain is approximately 10%. Variant angina is particularly common in Japan with 20-30% of patients who undergo coronary angiography for chest pain assigned a diagnosis of vasospastic angina. Of these patients, 40-80% have angiographically normal coronary arteries. Kulić M, Mujičić E, Šošević A et al. Prolonged spasm of the LAD
 with 20-30% of patients who undergo coronary angiography. Estimates are that 2-3% of all patients undergoing diagnostic cardiac catheterization for chest pain in the United States will subsequently be classified as having variant angina. In Italy, where rigorous inpatient electrocardiographic monitoring is frequently used, the incidence of variant angina in patients admitted with chest pain is approximately 10%. Variant angina is particularly common in Japan with 20-30% of patients who undergo coronary angiography for chest pain assigned a diagnosis of vasospastic angina. Of these patients, 40-80% have angiographically normal coronary arteries. Kulić M, Mujičić E, Šošević A et al. Prolonged spasm of the LAD.")
7
Kulić M, Mujičić E, Šošević A et al. Prolonged spasm of the LAD
DIAGNOSIS A 12-lead electrocardiograph should be repeated with each episode of chest pain Serial cardiac enzyme assays Holter monitoring Exercise tolerance test Thallium scintigraphy Coronary angiography Electrocardiographic features may include ST-segment elevation or depression. Ambulatory electrocardiography and Holter monitoring may increase the sensitivity of the aforementioned in-hospital evaluation if the diagnosis of variant angina remains elusive. Exercise tolerance was characteristically normal in these individuals, who experienced a cyclical pain pattern with most episodes occurring in the early morning hours. Thallium scintigraphy and coronary angiography may be required for diagnostic, prognostic, and therapeutic reasons. Kulić M, Mujičić E, Šošević A et al. Prolonged spasm of the LAD

8
Kulić M, Mujičić E, Šošević A et al. Prolonged spasm of the LAD
MEDICAL THERAPY Nitrates Calcium channel blockers (CCBs) Statins Medical therapy initially should include intravenous or sublingual nitroglycerin and an oral calcium channel antagonist. Long-acting oral nitrates are appropriate for the prevention of recurrent episodes and may be used in combination with the calcium channel antagonist for long-term prophylaxis. Nitrates and calcium channel blockers (CCBs) are the mainstays of medical therapy for variant angina. Nitroglycerin effectively treats episodes of angina and myocardial ischemia within minutes of administration, and the long-acting nitrate preparations reduce the frequency of recurrent events. Kulić M, Mujičić E, Šošević A et al. Prolonged spasm of the LAD
 Statins. Medical therapy initially should include intravenous or sublingual nitroglycerin and an oral calcium channel antagonist. Long-acting oral nitrates are appropriate for the prevention of recurrent episodes and may be used in combination with the calcium channel antagonist for long-term prophylaxis. Nitrates and calcium channel blockers (CCBs) are the mainstays of medical therapy for variant angina. Nitroglycerin effectively treats episodes of angina and myocardial ischemia within minutes of administration, and the long-acting nitrate preparations reduce the frequency of recurrent events. Kulić M, Mujičić E, Šošević A et al. Prolonged spasm of the LAD.")
9
Kulić M, Mujičić E, Šošević A et al. Prolonged spasm of the LAD
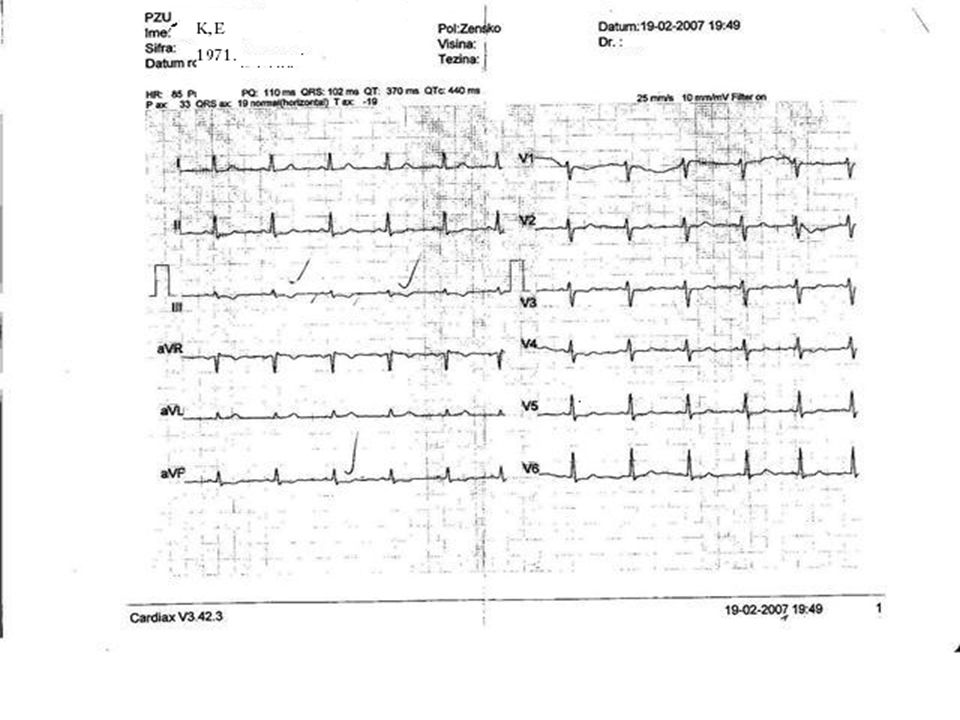
CASE REPORT 39-year old female patient chest pain since february 2007. EKG- SR, fr.: 75/min., neg T in D3, aVF, V1-V3 RR: 120/80mmHg., P: 75/min Lab exam: without abnormalities Kulić M, Mujičić E, Šošević A et al. Prolonged spasm of the LAD

11
Kulić M, Mujičić E, Gorani D et al. Prolonged spasm of the LAD
SADA PRIKAZATI EKG 2007/2008 Kulić M, Mujičić E, Gorani D et al. Prolonged spasm of the LAD

12
EKG 2009.

13
Exercise tolerance test was characteristically normal
slika ergometrije

14
Kulić M, Mujičić E, Šošević A et al. Prolonged spasm of the LAD
CASE REPORT Echocardiography was also normal with EF: 72%, without valvular abnormalities She was planed for MSCT or for coronary angiography Exercise tolerance was characteristically normal in these individuals, who experienced a cyclical pain pattern with most episodes occurring in the early morning hours. Kulić M, Mujičić E, Šošević A et al. Prolonged spasm of the LAD

15
Kulić M, Mujičić E, Šošević A et al. Prolonged spasm of the LAD
CASE REPORT Patient desided to performe directly coronary angiogram without MSCT Patient came from Montenegro in our cath.lab She also demanded coronary angiography by radial approach Exercise tolerance was characteristically normal in these individuals, who experienced a cyclical pain pattern with most episodes occurring in the early morning hours. Kulić M, Mujičić E, Šošević A et al. Prolonged spasm of the LAD

16
Kulić M, Mujičić E, Šošević A et al. Prolonged spasm of the LAD

17
Kulić M, Mujičić E, Šošević A et al. Prolonged spasm of the LAD

18
Kulić M, Mujičić E, Šošević A et al. Prolonged spasm of the LAD

19
Kulić M, Mujičić E, Šošević A et al. Prolonged spasm of the LAD

25
Kulić M, Mujičić E, Šošević A et al. Prolonged spasm of the LAD

26
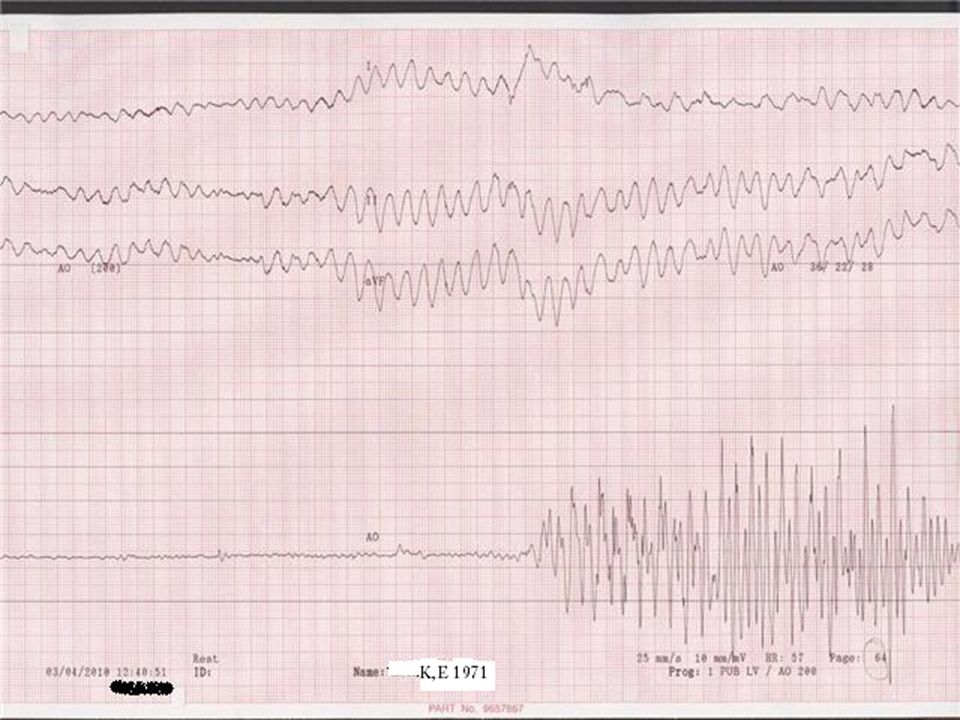
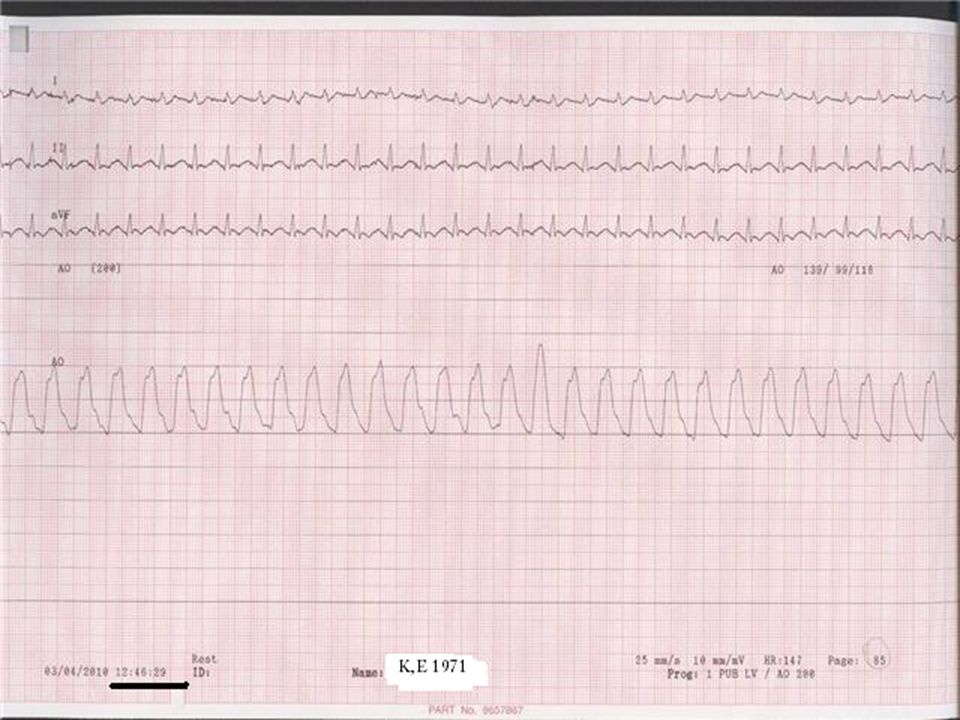
Conclusion Spasm of coronary arteries is sometimes a life-threatening condition The complete team, consisting of interventional cardiologist, intensivist/anesthesiologist and others, is necessery to be preasent for positive outcome of tretment of these patients. Kulić M, Mujičić E, Šošević A et al. Prolonged spasm of the LAD

27
Thank you

Similar presentations