Download presentation
Presentation is loading. Please wait.

1
Developing an ASHP Approved Residency Program
Janet Teeters, M.S., R.Ph. Director of Accreditation Services American Society of Health System Pharmacists

2
Objectives Provide examples of action you can take to develop a residency program. Describe three factors that will help make your residency program a success. Summarize the steps to have your residency program become accredited.

3
Questions to ask yourself?
Why do you want to start a residency? What does your site have to offer? Are you & your staff ready for a major commitment to the program? This is more than just taking pharmacy students on rotation….

4
Residency vs Experiential Training
Experience vs exposure Integrating knowledge, skills, abilities & attitudes to gain confidence in practice Repetition to reinforce development Ability to develop skills progressively Self selected group of individuals desiring to advance their skills

5
Residencies are the bridge between Education and Practice
Helping to develop clinical & professional maturity

6
How to begin? Initial assessment Costs of the program
Support for program Justification Program Design Individuals Role Recruitment Accreditation

7
Initial assessment Philosophy Organization Department
Staff (experience, interest, commitment) Services (scope & depth) Resources available Costs
 Services (scope & depth) Resources available. Costs.")
8
Costs of a residency program
Preceptor and program directors time Space and equipment Salaries and benefits of residents Travel Recruitment expenses Training of Preceptors Accreditation Fees

9
Gathering support Pharmacy Physicians Administration Nursing

10
Justification Patient care services Projects & programs
Medicare Pass through for post graduate medical education (if accredited) Recruitment and retention of staff Keeps the department contemporary Enhance credibility within an institution
 Recruitment and retention of staff. Keeps the department contemporary. Enhance credibility within an institution.")
11
Program Design Purpose # residents Structure
College affiliation, teaching opportunities Utilization of outside experiences

12
Program Design Use a systematic approach Understand instruction
Focus on assessment & feedback Roles & responsibilities

13
Systematic Approach to Training
Outcomes, Goals & Objectives Assessment Program Design Instruction

14
ASHP Residency Learning System “RLS”
Model for a systematic approach to training Maximize learning experiences Builds upon past experiences Focuses on improving instruction & feedback Provides consistency in assuring outcomes

15
Outcomes, Goals & Objectives
Outcomes: What resident graduate should be capable of doing Goals: What resident should learn to do Objectives: Observable, measurable behavior Criteria: Detail to evaluate performance related to the objectives Outcomes Goal Goal Obj Obj Obj C C C C C C C C C

16
Goal: Document patient care activities appropriately
Outcome: Provide patient centered care Goal: Document patient care activities appropriately Objective: Appropriate selection of activities Objective Effectively document appropriate information Objective: Explain exemplary documentation Criteria: Written in time to be useful Criteria: Follows Hospital Policy Criteria: Legible Criteria: Only pertinent information included Criteria: Accurate interpretation

17
Outcomes, G&O Selection Tips:
Include required outcomes, goals & objectives Limit the total number of outcomes

18
Design Learning Experiences (rotations) Areas of expertise
Determine length, type, electives Identify goals that match the experience Identify goals to be evaluated during the experience Identify learning activities to meet G&O

19
Design Tips: Only offer rotations - good role models and adequate patient #s Focus on the strengths of the site Strong role models for early experiences Limit the number of goals evaluated per rotation Don’t repeat the evaluation of the same goals with every rotation if goal has been obtained Develop effective communications between preceptors to avoid duplication of efforts

20
Provide Instruction Stage of Learning
Bloom’s – level of cognitive learning Methods of Instruction Foundation Knowledge, skills Knowledge Comprehension Reading, lecture Guided discussion Interactive lecture Practical Application Application Analysis Synthesis Case presentation Case based teaching Simulation Practice based teaching Integration Evaluation Practice based facilitation

21
Preceptors Role Residents Learning
Facilitating Culmination & integration Coaching Practical Application Modeling Direct Instruction Foundation Skills & Knowledge

22
Instruction Tips Educate preceptors on how resident training varies from student training Provide forum for preceptors to discuss effective methods they have used to learn from each other Provide development for preceptors

23
Assessment & Feedback Effectively “diagnose”
Provide effective guidance - criteria Constructive criticism Maximize residents progress Improve programs performance

24
Assessment & Feedback Tips
Key area of focus Can use a variety of methods to document feedback Use tools already developed

25
“ You are unaware of the effect you have on others.”
Chinese fortune cookie

26
Residency Program Director Preceptors All staff
Key Individuals Residency Program Director Preceptors All staff

27
Residency Program Director Role
Overall Champion for the program Initial assessment of entering resident Development of resident plan Monitoring of resident over time Assess preceptors & be a preceptor Assess program performance Improvement of the program

28
Preceptors Role Responsible for their experiences/rotation Instruction
Feedback Formative - constructive ongoing use snap shots/ criteria based checklists Summative – at the end of an experience Attainment of G&O assigned Receive Improve effectiveness Communicate to other preceptors

29
Overall challenges of design & implementation
Understanding the systematic approach RPh have not been trained in educational design Focusing on paperwork vs concept Need to involve all preceptors in design Takes time Everyone needs to be educated New staff CQI

30
If you build it they will come…….

31
not exactly…. Recruitment
Market yourselves! ASHP Midyear Mtg Students, Staff Other residency programs in your area Un-matched candidates post MATCH (March) State, regional, college presentations Brochures/ web pages Seeking accreditation
 State, regional, college presentations. Brochures/ web pages. Seeking accreditation.")
32
“ If you always do what you have always done, you’ll always get what you always got.” anonymous

33
Accreditation Acts as a catalyst to promote change and provide consistency in training A voluntary process to show a program meets national standards A means of self-regulation, using peer review

34
Why accreditation? Credibility Consistency Funding Recognition
Consumer protection Fosters continuous improvement Public relies on accreditation for Credibility Consistency Funding Recognition

35
What’s involved from the accreditation side?
Standard development Measuring compliance Review process Education

36
What’s involved from your side?
Program development Resident recruitment Application/ Reapplication Survey visits and reports Meeting & keeping current with standards Constantly improving your program Keeping your information up to date with ASHP

37
Accreditation application process
Read the standards & regulations Must have a resident Fees begin as soon as you apply Application includes program director information Information goes live on web site Site visit (after 9 months) Accreditation is retroactive to application date On going reports
 Accreditation is retroactive to application date. On going reports.")
38
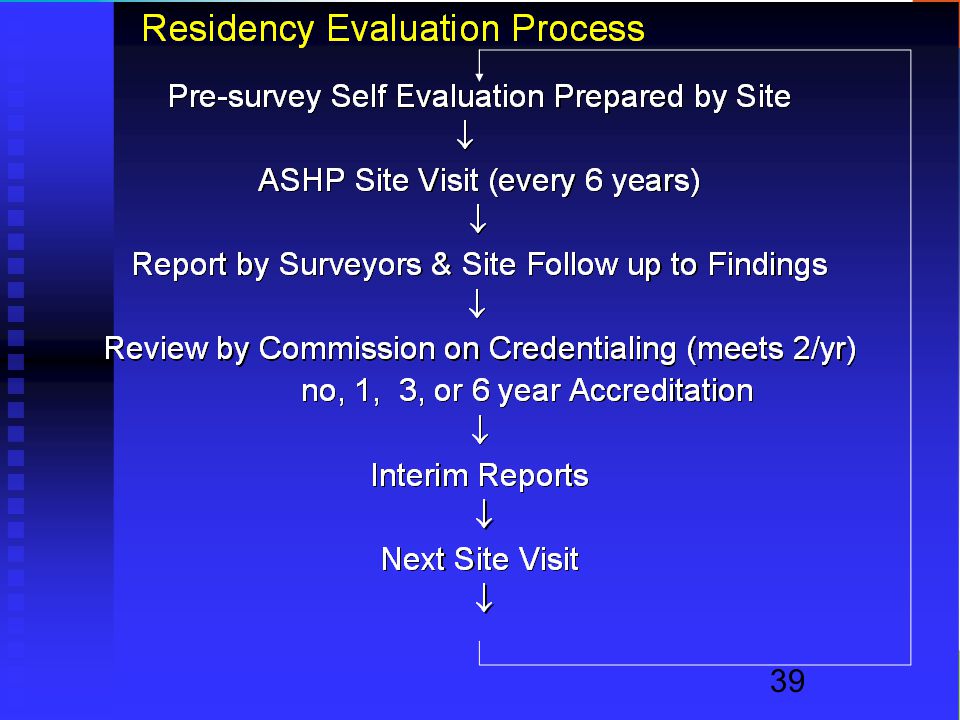
What to expect after application
Set Survey date Self- assessment Site survey Correspondence in response to report ASHP Commission on Credentialing ASHP Board of Directors

40
TOP Areas of Partial/Non-compliance in Pharmacy Practice
Residency training issues: Preceptors’ Contribution to Profession 56% 67% 58% ---- Individualized Plan for Resident 50% 54% 47% 55% Assessment of the Resident 44% 51% 44% 61% Resident Self Evaluations 41% 44% 56% 61% Progress over Time & Feedback % 44% 55% Document/plan for leave & impact 59% Based on 3/03, 3/04, 3/05, 3/06 COC

41
TOP Areas of Partial/Non-compliance in Pharmacy Practice
Pharmacy or service issues: Sterile Products Area 66% 79% 51% 58% Safe Drug System 63% 59% 65% 74% Drug Information 47% 56% 49% 48% Based on 3/03, 3/04, 3/05, 3/06 COC

42
TOP areas of Partial/Non-compliance in Specialized Programs
Residency training issues: Individualized goals/objectives 67% 56% 97% 63% Evaluations not routinely done 48% 52% 81% ---- Individual plan & monitored 52% 44% 94% 56% Resident has not completed PGY1 54% 44% 32% 50% Resident self evaluation % % 44% Based on 3/03 , 3/04, 3/05, 3/06 COC

43
New Residency Accreditation Standards

44
Factors related to release of new Residency Accreditation Standards
IOM reports JCAHO Roundtable/conference Future of Residency Training Conference ACCP/ASHP Partnership Open Hearings & comment periods ACPE standards

45
IOM - Core competencies for all health professionals
Patient-centered Interdisciplinary teams Evidence-based practice Utilize informatics Apply quality improvement

46
Residency Stakeholders Conference
Accreditation by one national body that includes key stakeholders All residencies should be accredited Residencies help develop innovative practices Colleges provide knowledge; residencies are becoming necessary to integrate knowledge into practice

47
Residency Stakeholder Conference
↑ need for residency trained individuals by 2015 ↑ need for community residencies PGY1 & PGY2 is appropriate model Terms and vision need to be consistent, defined, endorsed and embraced by the profession Specialization in the profession needs clarity

48
New Standards: PGY1 Pharmacy Residency
Replaces Pharmacy Practice (2001) PGY2 Pharmacy Residency Replaces Specialized Pharmacy Practice (1994) and all supplemental standards (Goals & objectives remain) Standards not altered at this time: Managed Care Pharmacy Practice Managed Care Systems Residency Pharmacy Practice (with emphasis in Community Care)
 PGY2 Pharmacy Residency. Replaces Specialized Pharmacy Practice (1994) and all supplemental standards. (Goals & objectives remain) Standards not altered at this time: Managed Care Pharmacy Practice. Managed Care Systems Residency. Pharmacy Practice (with emphasis in Community Care)")
49
Generalist Focused Practitioner Advanced Practitioner
PharmD Graduate Broad Patient/Practice FOCUS Narrow A PGY1 Generalist Wide variety of patients & diseases PGY B Generalist Focused Practitioner Wide variety of diseases may be in a unique setting or population (e.g., pediatrics, geriatrics, ambulatory, managed care) C PGY2 Advanced Practitioner More experience, skill and ability developed in a broad set of patients (e.g., pharmacotherapy) PGY D More experience, skill, and ability developed in a focused area of practice (e.g., oncology, critical care) Basic DEPTH of knowledge, skills, abilities, experience Advanced
 C PGY2. Advanced Practitioner. More experience, skill and ability developed in a broad set of patients. (e.g., pharmacotherapy) PGY2 D. More experience, skill, and ability developed in a focused area of practice (e.g., oncology, critical care) Basic. DEPTH of. knowledge, skills, abilities, experience. Advanced.")
50
Principles of accreditation
Resident’s qualifications Environment for learning Resident’s responsibilities Training program (systematic approach) Residency Program Director & Preceptors Organization Pharmacy
 Residency Program Director & Preceptors. Organization. Pharmacy.")
51
New Standards PGY1/PGY2 General training vs. advanced depth of training Incorporates IOM core competencies Duty hours Participation in the match

52
PGY1 - 6 Core Competencies
Medication use process Quality Improvement IOM Patient-centered care IOM Interdisciplinary Teams IOM Evidence Based Practice IOM Leadership and management Project management Education/training Medical informatics IOM

53
PGY2 Residency Program Directors
PGY2 Residency & 3 years or 5 years of experience in the area BPS - Board Certification Nuclear Nutrition Oncology Psychiatry Pharmacotherapy + added qualifications Infectious Diseases Cardiology

54
Why is accreditation important to a resident?
Think of the residents expectations they are giving up a year of full salary, with college loans to do this program. Accelerates development of their practice skills Competitive advantage in the market place Mentorship Networking opportunities Career planning Shows that the site is committed to excellence Ensures they are not used as cheap labor

55
Why is accreditation important to a site?
Funding – where applicable Commitment to excellence Means of self regulation CQI Helps advance the practice of pharmacy Recruit and retain staff & residents Enhanced credibility

56
Seek advice from others:
Other Residency Programs & preceptors ASHP – Accreditation Services ASHP Midyear Clinical Meeting – new and prospective residency program workshops and town hall meeting ASHP National Residency Preceptors Conference ASHP Residency Learning System – training programs Colleges of pharmacy

57
STARTING YOUR RESIDENCY PROGRAM

58
Objective 1 Actions you can take to develop a residency
Assessment Identify Costs Justification Learn about systematic approach Design Program Train & educate Strategy for recruitment Review ASHP accreditation standards

59
Objective 2 Factors to help make your residency program a success
Champion & commitment Thorough education and preparation Involve as many individuals as possible Must realize this is about education and may need to learn new principles different then how you were taught Realize this is not a short term process – it improves with time and continuous improvement This involves the entire department, not just a few

60
Objective 3 Steps to have residency become accredited
Read standards & regulations Begin design based on standards Seek advise from others Attend training programs (RLS, new programs, NRPC/MCM) Design program with involvement of many Recruit a resident Apply!
 Design program with involvement of many. Recruit a resident. Apply!")
61
Just do it!

Similar presentations














 Grants Chapter 6.>")





