Download presentation
Presentation is loading. Please wait.

1
Neuroimaging in the Neonate
Debra B. Selip, MD Fetal and Neonatal Medicine Center and Division of Neonatology Rush University Medical Center March 4, 2011

2
Neuroimaging in the Neonate
Wide array of imaging modalities readily available Expanding and rapidly changing body of literature examining appropriate imaging methods and prognostic applications

3
Neuroimaging Modalities
Xray Ultrasound CT scan MRI T1 T2 DWI / DTI / FA / Tractography MR Spectroscopy NM Scans SPECT PET

4
Why Image? 2 Roles: Diagnose brain injury in at risk newborns
Improve and provide acute medical management/interventions Detect lesions associated with long-term neurodevelopmental disability Appropriate prognosis/predictions Appropriate tx: Brain cooling Phenobarb? Bumetanide? Redirection? Approp prognosis: Cognitive Motor Psych Neurosensory

5
Prognostic Concerns Clinical evaluation insufficient for prognostication Cerebral Palsy? School Performance? Neurocognitive & neurodevelopmental disabilities Behavioral disabilities Role for neuroimaging?

6
2 Types of Neonates Preterm Infants Periventricular Leukomalacia
Intraventricular Hemorrhage Post-hemorrhaghic Hydrocephalus Periventricular Hemorrhagic Infarction Intraparenchymal Hemorrhage Cortical and Deep Gray Matter Injury

7
2 Types of Neonates Full term Infant Stroke Intracerebral Hemorrhage
Periventricular Leukomalacia Intraventricular Hemorrhage Congenital Anomalies Cortical and Deep Gray Matter Injury

8
Outline Preterm infant: ELGAN / VLBW Term Epidemiology
Neuroimaging modalities Indications for use Findings and clinical correlates Conclusions Term Not late preterm infant. Focus on ELGA / VLBW Late preterm – not lots info on imaging on these infants – I suspect most their difficulties are cognitive and we’re still trying to figure out their deficits and then ultimatley how to identify them early.

9
The brain is a wonderful organ; it starts working the moment you get up in the morning and does not stop until you get into the office Robert Frost

11
Epidemiology: Preterm Infant
ELGAN/ VLBW: number preterm infants and survival: For babies less than 32 wks Greater than 2% of all live births Up to greater than 85% survival Emphasis on Outcomes: Improvement in ND outcomes Infants less than 26 wks: Approximately 15% with CP At 11 yrs: 25% severe ND disability 35% moderate ND disability 20% mild ND disability Outcomes: no sense in saving these babies if we can’t give them a good chance “normal” life Marlow et al. NEJM 2005 Anderson et al. JAMA 2003 Epicure, 2005

12
Epidemiology: Preterm Infants
Emphasis on Outcomes: Infants less than 30 wks 25 – 50% cognitive, behavioral, social difficulties requiring special ed. intervention 5 – 15% cerebral palsy, severe neuro-sensory impairment or both Overall: At 8 years of age 50% children BW less than 1 kg in special education 20% children BW less than 1 kg repeat a grade 10 -15% children BW less than 1 kg with spastic motor CP Marlow et al. NEJM 2005 Anderson et al. JAMA 2003

13
Typical Injury Patterns: ELGA / VLBW
IVH Ventriculomegaly White matter injury PHH Gray matter injury Hemorrhage Hypoxia Ischemia LEADS TO Volpe, Neurology of the Newborn, 2008 Follett et al, JNeurosci, 2001, 2004 Deng et al, PNAS, 2006

14
Evolution of Injury: ELGA / VLBW
Local necrosis with congestion or hemorrhage Echo-lucent cysts in periventricular white matter Echolucent cysts – tissue dissolution – 1-3 wks Ventriculomegaly – 2-3 months Ventriculomegaly, cysts disappear, deficient myelin and/or gliosis with collapse of cysts, echo-densities

15
Factors to Consider When Imaging Critically Ill Infants
Timing Technique Transport Compatibility Availability Sedation Given the modalities readily available to us and the limitations and difficulties we encounter, we’re going to examine the following (next slide)
")
16
Ultrasound: Diagnostic Capabilities
Hemorrhagic Hydrocephalus Periventricular hemorrhaghic infarction Non-hemorrhagic Echodensities Echolucencies Ventricular enlargement Edema Sensitivity much increased with multiple scans Echolucencies – less frequently seen in white matter but much more predicitive of long term clinical morbidity. Most ominous in the first 2 wks of life. Risk for PHH – most prognostic question Late U/S findings with ventricular enlargement, cystic changes in white matter or hydrocephalus – increased risk of CP Later scans more prognostic Echolucencies strongly assoc with CP more so than MR Echodensities freq transient Reasons to change from Papile grading system to descriptions. DeVries et al, JPediatric, 2004

17
El-Dib, M. et al. Am J Perinatol. 2010.

18
Grades of IVH – grade 1 to 4 El-Dib, M. et al. Am J Perinatol

19
El-Dib, M. et al. Am J Perinatol. 2010.

20
Ultrasound: Prognostic Capabilities
Major abnormalities Gr 3 IVH, PHI, Cystic PVL Predictive of CP and NM delay at follow up Predictive of impaired cognitive outcome but with less sensitivity and specificity Mild abnormalities Prediction of CP or cognitive deficits is problematic Not predictive of NORMAL outcome El-Dib, M. et al. Am J Perinatol

21
Ultrasound: Prognostic Capabilities
Diffuse PVL: low sensitivity Misses greater than 50% diffuse white matter injury Hemorrhage conveys less prognostic info than evidence of white matter damage and PHH Cerebellar Injury 30 -60% preemies who develop CP had lesions on US during perinatal period

22
Ultrasound: Prognostic Capabilities
Recent literature gr1 and gr2 IVH in infants <26 GA with poorer ND/NC outcomes Significant assoc. btwn gr 3 – 4 IVH, Cystic PVL, mod- sev ventriculomegaly, and CP at 2 - 9yrs in babies < 1500g Patra, K et al. JPeds, 2006

23
Ultrasound: Prognostic Capabilities
Grade 4 IVH and ventriculomegaly strong assoc with MR and neuropsych disorders at yrs in infants <1500g Odds Ratio: 10 fold increase in adverse outcome with above sonographic findings

24
Ultrasound: Limitations
Poor contrast for lesions of brain parenchyma Limited field of view Insensitive for identification of hemorrhage adjacent to bone Fair cerebellar views Operator dependent

25
Ultrasound: Conclusions ELGAN / VLBW
Routine screening <30 wks Screen btwn days 80% IVH Screen 36 wks PMA White matter injury Diagnostic utility quite good Prognostic role limited to more severe injury patterns Serial HUS may increase predictive abiltiy

26
He who joyfully marches to music in rank and file has already earned my contempt. He has been given a large brain by mistake, since for him the spinal cord would suffice. Albert Einstein

28
MRI: ELGAN / VLBW T1 T2 DWI/ DTI/ FA / tractography / fMRI Volumetrics
Early MRI Corrected term (40 – 42 wks CGA) Utility in preterm brain Utility in term corrected brain Abnormalities of myelination of PLIC correlate very closely with cerebral palsy T1/t2 – subacute injury DTI/DWI – acute injury T.M. O’Shea et al. EarlyHumDev, 2005.
 Utility in preterm brain. Utility in term corrected brain. Abnormalities of myelination of PLIC correlate very closely with cerebral palsy. T1/t2 – subacute injury. DTI/DWI – acute injury. T.M. O’Shea et al. EarlyHumDev,")
29
MRI: ELGAN /VLBW Superior evaluation of: Identifies:
Brain structures Gray / white matter Brain stem / posterior fossa Identifies: More abnl findings 1st wk of life More hemorrhagic lesions More extensive cysts Subtle / Diffuse white matter injury Prognostic benefit: CP Learning disabilities Behavioral problems

31
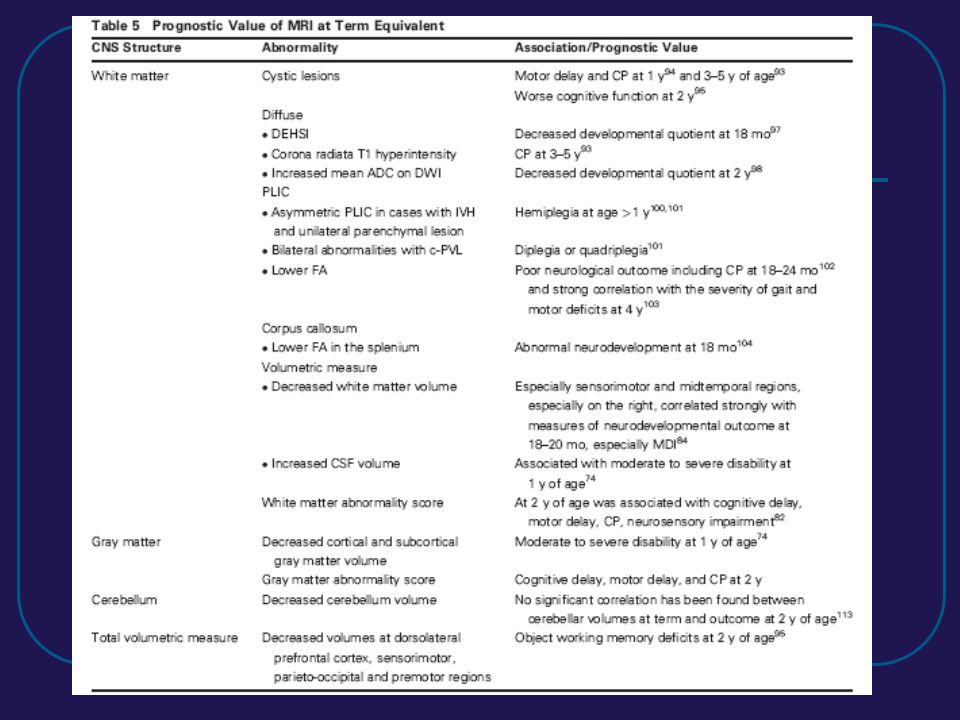
MRI : Prognostic Capabilities
Woodward et al. Neonatal MRI to Predict Neurodevelopmental Outcomes in Preterm Infants. NEJM, August 2006. 167 infants < 30 wks At 2 yrs 17 % severe cognitive delay 10 % severe psychomotor delay 10% CP 11% neurosensory impairment 21% moderate – severe cerebral white matter injury Attempt to correlate clinical outcomes from children 2 yrs and MRI findings at term (PMA) New Zealand and Australia
 New Zealand and Australia.")
32
Woodward et al. NEJM. Aug 2006

33
MRI: Prognostic Capabilities Cont…d
Majority of preemies have Loss of volume Cystic abnormality Enlarged ventricles Thinning of the corpus callosum Delayed myelination Can these term findings be associated with definitive outcomes at 2yr, 4yrs, 6yrs, etc

34
Study Results 28% no white matter injury 5% mild white matter injury
17% moderate white matter injury 6% severe white matter injury Correlation of MRI at term with outcome at 2 yrs of age (corrected) More signif the white matter injury, the greater the neuro dev impairment Normal or mild MRI result = free of severe impairments at 2yrs. Mod –severe MRI white matter injury – severe neurodev deficits Most common impairment noted severe cognitive delay (approx 20% of kids scored more than 6mo below corrected age)
 More signif the white matter injury, the greater the neuro dev impairment. Normal or mild MRI result = free of severe impairments at 2yrs. Mod –severe MRI white matter injury – severe neurodev deficits. Most common impairment noted severe cognitive delay (approx 20% of kids scored more than 6mo below corrected age)")
35
The chief function of the body is to carry the brain around.
Thomas A. Edison

37
CT Scan: ELGAN / VLBW Good imaging modality Limited use due to:
Hemorrhage Cerebral volume / Ventricles / Extra-axial space Bones Limited use due to: Ionizine radiation / risk of future malignancy Cognitive impairment Correlations btwn clinical outcome and image results weak Ionizing radiation – o.1% risk life long fatal malignancy from head CT at age 12 months estimated Risk of development of brain tumor found to be 10 fold higher in infants exposed to cranial irradiation under 5 mo. In comparison to over 7 mo.

38
MRI vs Ultrasound vs CT in the ELGAN/VLBW: Conclusion
Ultrasound Early MRI Later Ultrasound early MRI later Forget the CT Scan

39
Imaging the Term Infant
Hypoxic Ishcemic Encephalopathy Neonatal Stroke Arterial Ischemic Stroke Cerebral Venous Thrombosis Intracerebral Hemorrhage Periventricular Leukomalacia Intraventricular Hemorrhage Congenital Anomalies

40
Ultrasound: Term Infant
Not ubiquitously helpful Poor parenchymal evaluation Poor anatomic views Poor for stroke Good for IVH evaluation Doppler views Vascular Hydrocephalus vs Ventriculomegaly RI = (systolic ACA blood flow – diastolic ACA blood flow) diastolic ACA blood flow Marker of acute edema, increased ICP
 diastolic ACA blood flow. Marker of acute edema, increased ICP.")
41
CT Scan: Term Infant Significant findings Global picture of injury
Calcifications Hemorrhage Low attenuation in basal ganglia and thalamus Global picture of injury Extremely fast Emergent situation Limited use due to: Risk of future malignancy Risk of future cognitive impairment Usu in infant with midline shift on HUS who needs emergent neurosurg intervention

42
MRI: Term Infant No ionizing radiation Multi-planar imaging
More sensitive and specific for CNS evaluation than CT or US Grey matter White matter Modality of choice

43
MRI: Hypoxic Ischemic Encephalopathy
Water and the brain T1 – 7 days T2 – 7 days DWI: one of the earliest indicators of tissue injury (within hours) – best 2 – 4 days No ionizing radiation Volumetric data of sensorimotor and mid-temporal cortices are assoc with full scale verbal and performance IQ scores PLIC most reliable region compared to histopath Evolving patterns of injury over time MR Spect: functional eval - creatinine and lactate peaks >50% basal ganglia and thalamic region injury
 – best 2 – 4 days. No ionizing radiation. Volumetric data of sensorimotor and mid-temporal cortices are assoc with full scale verbal and performance IQ scores. PLIC most reliable region compared to histopath. Evolving patterns of injury over time. MR Spect: functional eval - creatinine and lactate peaks. >50% basal ganglia and thalamic region injury.")
44
MRI: Pattern of Brain Injury
2 main types Basal Ganglia-Thalamus Acute near total asphyxia CP / cognitive injury readily apparent Watershed Predominant Prolonged partial asphyxia Ant – Mid cerebral artery Post –Mid cerebral artery Childhood symptoms / Deficits at 30 mo.

45
MRI: HIE Prognostic Capabilities
Neurodevelopmental handicap at 1-2 yrs of age if: Basal ganglia or thalamic abnormality 50 – 94% with CP, mental retardation, seizure disorder Well established

46
I was taught that the human brain was the crowning glory of evolution so far, but I think it's a very poor scheme for survival. Kurt Vonnegut

48
MR Spectroscopy: Term Infant
Non-invasive in vivo biochemical analysis Cellular metabolic information Detection of biochemical changes before morphological changes apparent NAA Lactate Creatine Choline Prognosis Early H-MRS studies promising

49
Summary Appropriate modality for particular investigation
Pre-term Imaging US MRI MR Spect? Full-term Imaging CT

Similar presentations








 and cervical neurofibroma removal (7/09) MRI studies showed an enhancing.>")




 II: Evaluation of Long-term Neurocognitive Development in Pediatrics U.S. Food and Drug Administration.>")


 Sensitive indicator of perfusion Diagnosis and prognosis of.>")



 Report of the Quality Standards Subcommittee of the American Academy of.>")
