Download presentation
Presentation is loading. Please wait.

1
IN THE NAME OF GOD

2
CASE PRESENTATION

3
HISTORY A 31 years Old female from Chatroud kerman with complaints of cough, moderate hemoptysis, was hospitalized for 3 days. The patient complained of weakness and fatigue earlier than a year ago. Than a few months ago with sparseness palpitations, chest pain,mild dyspnea. Patient also complained of a dry mouth, sore tongue,weight loss 15kg over last year,. Patient had recently mild dysphagia to solids intermitant.

4
past history she did not have any previous history of known illness, except admission for lobectomy becase swelling parotid years ago.patologyreport: 1-intra parotid lymphoid tissue with dailated duct. 2-lymph node,post auricular resection reactive hyperplasia.

5
Drug history 1-tab ferrus sulfate daily for 3 month ago. 2-tab folic acid 1mg daily. 3-tab alprazolam 0/25mg QHS perevious 10day. 4-tab propranolol 20mgBID.

6
Family History There was no significant point.Her husband died due to seizures, 8 months ago and SHe was living with her 12 year old daughter. Personal and Social History: -She was not smoker and opium addict.

7
PHYSICAL EXAMINATION. Patient is ayoung age female, awake and oriented, with distress, she was thin and pale. Vital Sign: PR:100RR:22 BP:90/60AxilaryT:38

8
PHYSICAL EXAMINATION The conjectiva is paile-Trachea and thyroid were normal- No adenopathy. Chest examination: decrease of sound in basal of left side and fine Crackle in 1/3 lower left side.heart exam was normal. Abdomen: There was no distention, tenderness, hepatomegaly, splenomegaly and ascites. Upper and lower extremitie was normal.

9
LABORATORY TEST CBC was 2 months ago: WBC:4000 RBC:4300000 HG:10.8 HCT:34.7 MCV:80 MCH:25.1 MCHC:31.3 Plat:108,000

10
LABORATORY TEST BMA was normal ECHOCARDIOGRAPGY: EF:60 % PAP:40 mild pericardial effiusion.

11
LABORATORY TEST Normal range C3:90 70-196 ANA: NEGATIVE C4:17 10-40 PANCA: NORMAL CH50:100 101-300 AntiGBM:13.9 (<25) AntidsDNA:9.4(<25) CANCA: NORMAL
 AntidsDNA:9.4(<25) CANCA: NORMAL")
12
LABORATORY TEST CBC: WBC:5400 RBC:4,180,000 HG:10.5 PLT:143,000 HCT:33.9 MCV:81.1 MCH:25.1 MCHC:31

13
Biochemistry BS:100 Na:146 K:4.7 Urea:51 Creat:1.4 Ca:4.2 ESR:73 U/A:NORMAL PT:16 PTT:30 INR:1.4 AST:72 ALT:53 ALP:147 Bil Total:0.4 Bil Diect:0.2

19
CHEST CTSCAN a mass lesion in the middle mediastinum with is seen that for better evaluation ct scan with contrast is recommended.wall thickening of esophagus is seen that endoscopy is recommended. Left plural effiusion is vesible.

21
ABDOMINOPELVICE SONOGRAPHY Liver, biliary tract, pancreas and urinary tract Were normal. Size spleen 140mm and mild plural effiusion in left hemithorax

22
Problem list Moderate hemoptysis Cough& dyspnea Fever Chest pain Palpitation Intermitant dysphagia weight loss weakness and fatigue Bicytopenia Pap:40 & mild p.e ESR:73 AST:72 & ALT:53 Middle mediastinal mass Mild P.E

23
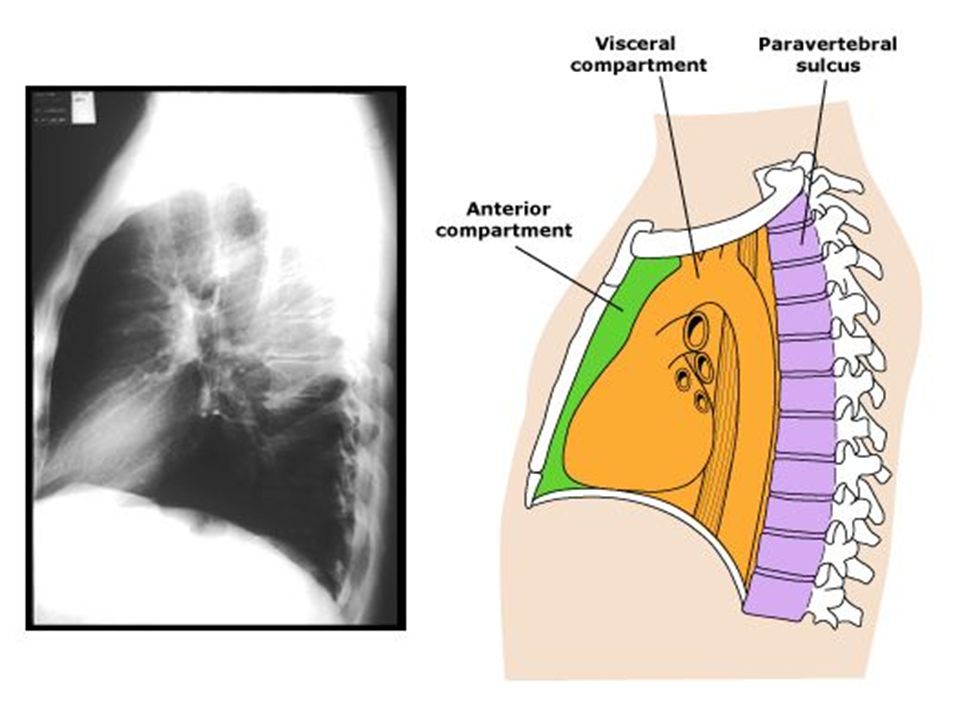
mediastinum The mediastinum extends from the thoracic inlet to the diaphragm, and contains many vital structures, including the heart and great vessels, and esophagus.

25
anterior mediastinum The anterior compartment (also referred to as the anterosuperior compartment or retrosternal space) is anterior to the pericardium and includes the thymus, the extrapericardial aorta and its branches, the great veins, and lymphatic tissue.
 is anterior to the pericardium and includes the thymus, the extrapericardial aorta and its branches, the great veins, and lymphatic tissue.")
26
middle mediastinum The middle compartment is bounded by the pericardium anteriorly, the posterior pericardial reflection, the diaphragm, and the thoracic inlet. This compartment includes the heart, intrapericardial great vessels, pericardium, and trachea.

27
posterior mediastinum The posterior compartment extends from the posterior pericardial reflection to the posterior border of the vertebral bodies and from the first rib to the diaphragm. It includes the esophagus, vagus nerves, thoracic duct, sympathetic chain, and azygous venous system.

28
masse in anterior compartment Thymic tumors (thymomas), thymic carcinomas, thymic carcinoid tumors, and thymolipomas), thymic cysts. germ cell tumors, Hodgkin and non-Hodgkin lymphomas. intrathoracic goiter, thyroid tumors, parathyroid adenomas. connective tissue tumors (eg, lipomas, liposarcomas, lymphangiomas, lymphangiohemangiomas, hemangiomas), and pericardial cyst.
, and pericardial cyst..")
29
Masses of the middle mediastinum thyroid tumor, goiter, tracheal tumors, aortopulmonary paraganglioma (chemodectoma), bronchogenic cysts and lymphomas. A middle mediastinal mass may also represent lymphadenopathy as a result of infectious, malignant (metastatic), and idiopathic (eg, sarcoidosis) etiologies. Thymic masses and pericardial cysts have been reported in the middle mediastinum, however, these lesions generally occur in the anterior mediastinum
, and idiopathic (eg, sarcoidosis) etiologies. Thymic masses and pericardial cysts have been reported in the middle mediastinum, however, these lesions generally occur in the anterior mediastinum.")
30
posterior mediastinum mass neurogenic tumors, esophageal tumors and duplication cysts, hiatus hernia, and neurenteric cysts. Extramedullary hematopoiesis, pancreatic pseudocyst, and achalasia have all been reported as unusual causes of a posterior mediastinal mass. Aneurysms of the aorta may occupy any compartment depending upon their anterior, intrapericardial, or posterior location.

32
Clinical manifestations Airway compression can lead to recurrent pulmonary infection and/or hemoptysis Esophageal compression can cause dysphagia Involvement of the spinal column can result in paralysis Phrenic nerve damage can present with an elevated hemidiaphragm Hoarseness can occur due to recurrent laryngeal nerve involvement Horner's and superior vena cava syndromes arise due to sympathetic ganglion and superior vena caval involvement, respectively

33
Clinical manifestations

34
Evaluation mediastinal mass

36
BRONCOSCOPy Abnormal mucosa,external pressure and a small masslike lesion in the entrance of LMB&bleeding from LMB. Bleeding controlled with transhexamic acid&BAL and biopsy was performed.

37
Thoracic surgery was consulted, because of stress and lack of patient consent were not candidates for mediastinoscopy.

38
diagnosis The hemoptysis was controlled after the patient re-bronchoscopic and appropriate biopsy was performed. HIV testing was requested. Pathology report : NHL(DLBCL). HIV test:posetive.
. HIV test:posetive..")
39
Lymphoproliferative disorders in immunocompromised patient 1- acquired immune deficiency syndrome (AIDS)- related lymphoma (ARL): (a) usual lymphomas primarily involving the lung, DLBCL and Burkitt lymphoma being the commonest (b) others: primary effusion lymphoma (PEL), plasmablastic lymphoma 2- post-transplantation lymphoproliferative disorder (PTLD), which includes reactive processes, neoplasms and lymphoid proliferations of uncertain nature.
- related lymphoma (ARL): (a) usual lymphomas primarily involving the lung, DLBCL and Burkitt lymphoma being the commonest (b) others: primary effusion lymphoma (PEL), plasmablastic lymphoma 2- post-transplantation lymphoproliferative disorder (PTLD), which includes reactive processes, neoplasms and lymphoid proliferations of uncertain nature.")
40
AIDS-related lymphoma Infection with HIV predisposes to the development of neoplasms, including lymphoma. AIDS-related lymphoma is generally divided into three types: systemic non-Hodgkin lymphoma (NHL) primary central nervous system lymphoma. primary effusion ("body cavity") lymphomas
 primary central nervous system lymphoma. primary effusion ( body cavity ) lymphomas.")
41
AIDS-related lymphoma Patients infected with human immunodeficiency virus (HIV) have a higher risk to develop non Hodgkin’s lymphoma (NHL) with high frequency of extranodal lesions. Lymphoma occurs in 3 to 10% of patients with AIDS and is the second most common malignancy in this group

42
AIDS-related lymphoma This neoplasm is usually of high-grade B-cell type and the most frequent location is in the CNS, GI system, liver, spleen, and bone marrow. Thoracic involvement occurs in < 10% of the cases. A variety of clinical forms of AIDS-related lymphoma in the chest x-ray have been described, including pleural effusion, interstitial and alveolar lung disease, peripheral nodules, and occasionally, hilar and mediastinal adenopathies.

43
AIDS-related lymphoma HIV-associated lymphoma is most commonly diagnosed in patients with advanced HIV, a low CD4 count (often <100/microL), high HIV viral load, and a prior diagnosis of AIDS. Since the introduction of highly antiretroviral therapy, the incidence of HIV-associated lymphoma has declined and the median CD4 count at diagnosis has increased.

44
AIDS-related lymphoma The risk of developing NHL in the setting of HIV increases directly with the level of immune system dysfunction. The incidence, pathology, clinical presentation and course of AIDS-related lymphomas do not seem to be related to the risk factor for the HIV infection itself. Epstein-Barr virus (EBV) coinfection is a risk factor for and involved in the pathogenesis of subtypes of NHL.
 coinfection is a risk factor for and involved in the pathogenesis of subtypes of NHL..")
45
AIDS-related lymphoma systemic lymphoma in the HIV-positive population is characterized by frequent B symptoms (ie, fever, weight loss, night sweats), extranodal disease, involvement of unusual locations.
, extranodal disease, involvement of unusual locations.")
46
TREATMEN Survival without treatment in patients with aggressive NHL, such as DLBCL, can be measured in months. With the advent of combination chemotherapy with cyclophosphamide, doxorubicin, vincristine, and prednisone (CHOP). cyclophosphamidedoxorubicinvincristineprednisone Survival has been further improved with the addition of rituximab to standard CHOP-based therapy (R-CHOP).rituximab
. cyclophosphamidedoxorubicinvincristineprednisone Survival has been further improved with the addition of rituximab to standard CHOP-based therapy (R-CHOP).rituximab.")
Similar presentations











>")







>")






