Download presentation
Presentation is loading. Please wait.

1
Mental Health Option Unit 4
A WEEK WITH DEPRESSION Mental Health Option Unit 4

2
Core Symptoms Persistent sadness over a long period of time AND anhedonia (getting no pleasure from formerly pleasurable activities)
")
3
Depressed Mood A person may report feeling "sad" or "empty" or may cry frequently. Children and adolescents may exhibit irritability.

4
Decreased Interest or Pleasure
A person may show markedly diminished interest or pleasure in all, or almost all, daily activities.

5
Weight Changes Significant changes in weight when not attempting to gain or lose (a gain or loss of 5% or more in a month) may be indicative of depression. In children, this may also present as a failure to make expected weight gains.
 may be indicative of depression. In children, this may also present as a failure to make expected weight gains.")
6
Sleep Disturbances Insomnia or sleeping too much may be a symptom of depression.

7
Psychomotor Agitation or Retardation
The person may be observed to be either agitated and restless, or physically slowed down in their movements.

8
Fatigue Deep fatigue or a loss of energy is a symptom of depression.

9
Feelings of Worthlessness or Guilt
A depressed person may feel that they have no value or they may feel inappropriately guilty about things they have no control over.

10
Brain Fog A depressed person may have a diminished ability to think, concentrate or make decisions.

11
Thoughts of Death A depressed person may have recurring thoughts of death, especially thoughts of suicide, with or without a specific plan.

12
From Oxford Psychology Units 3&4

13
Depressive Symptoms Mnemonic: “Space Drags”
S leep disturbance P leasure/interest (lack of) A gitation C oncentration E nergy (lack of)/fatigue D epressed mood R etardation movement A ppetite disturbance G uilt, worthless, useless S uicidal thought
 A gitation. C oncentration. E nergy (lack of)/fatigue. D epressed mood. R etardation movement. A ppetite disturbance. G uilt, worthless, useless. S uicidal thought.")
14
Diagnosis: Dimensional or Categorical
Symptoms CORE: Prolonged sadness (at least 2 weeks for most if not all of the day Anhedonia for most if not all activities for most if not all of the day OTHER Loss of energy / fatigue Inappropriate guilt / self-blame Thoughts of death / suicide Difficulty concentrating Sleep disorder Appetite change State of agitated or psychological and/or physical activity ICD-10 adds one more loss of confidence or self-esteem may only need 3 of the symptoms may only experience symptoms that last a few hours Impairment an impairment in the person’s day-to-day functioning Diagnosis Must have: At least ONE core symptom At least FIVE of the nine symptoms Impairment in day-to-day functioning Distinguishing characteristics between minor (no clinical treatment recommended) and major depression Do not think it is valid to distinguish between minor and major depression Treatment should simple be based upon the distress and impairment the person is experiencing Uncovering Psychology page 509
 and major depression. Do not think it is valid to distinguish between minor and major depression. Treatment should simple be based upon the distress and impairment the person is experiencing. Uncovering Psychology page 509.")
15
Biopsychosocial Model
A Focus for Causes and Treatments

16
FOCUS Treatment options depend on view of causes – if we accept the interactive nature of the biopsychsocial framework, then a holistic approach to treatment will be most successful. [Help is available]

17
Biopsychosocial Model
A general model that states that biological, psychological, and social factors, all play a significant role in human functioning in the context of disease or illness. 1. Biological - the genetic code of an individual. 2. Psychological - focus on cognitive, emotional, personality, perceptual, spiritual, and related factors that affect the development of an individual. 3. Socio-cultural - focus on how an individual interacts with their environment - the effects that culture, societal, interpersonal interactions, and ethnic variations have on an individual.

18
The model for the phobia connects nicely to Depression:

19
Biological Sociocultural Psychological
Depression Neurotransmitter imbalance that can excite or inhibit brain responses; genetic factors increase risk Biological Sociocultural Family and social networks Psychosocial Stress Social Isolation Poverty Abuse Cognitive and behavioural changes Pessemistic explanitory style Psychological Learned helplessness

20
Symptoms of Depression Psychological Factors Sociocultural Factors
Excessive or persistent dejected mood Dimished interest and pleasure in activities Prolonged feelings of despair and hopelessness Cognitive and behavioural changes Pessemistic explanitory style Psychological Factors Learned helplessness Sociocultural Factors Family and social networks Psychosocial Stress Social Isolation Poverty Abuse Neurotransmitter imbalance Genetic predisposition Biological Factors

21
Biological Factors role of genes in contributing to the risk of developing major depression role of neurotransmitters serotonin and noradrenaline in major depression the function of antidepressant medication in management

22
Genetics

23
Genetics A family history of depression does not necessarily mean children or other relatives will develop major depression. However, those with a family history of depression have slightly higher chances of becoming depressed at some stage in their lives. There are several theories to explain this phenomenon.

24
Family Studies Having a first degree relative (parent or sibling) with depression appears to be a risk factor for depression. Family studies select people who already have depression. If there is a genetic link for this disorder, relatives should show a higher rate of depression compared to the rest of the population. Around 20% of such relatives have depression compared with around 10% of the population at large (Harrington et al. 1993).
.")
25
Twin Studies If we assume that the environment shared by twins is roughly the same for both types of twin, any greater similarity between MZ and DZ shows the action of genes. Allen (1976) reported a mean concordance rate of 40% for MZ twins and only an 11% rate for DZ twins.
 reported a mean concordance rate of 40% for MZ twins and only an 11% rate for DZ twins.")
26
Adoption Studies Wender et al. (1986) studied the biological relatives of adopted people who had been hospitalised for severe depression. There was a much higher incidence of severe depression in these relatives than in those of a non-depressed control group.

27
Neurotransmitters

28
Noradrenaline and Seotonin
Two neurotransmitters have been thought to be involved in depression, noradrenaline and serotonin. It has been thought that the low levels of noradrenaline leads to the depression and the high levels to the mania. The serotonin theory suggests that low levels of serotonin produces depression also. (More specifically, noradrenaline is controlled by the levels of serotonin)
")
30
Noradrenaline When a nerve impulse arrives at a noradrenaline nerve terminal, noradrenaline is released from synaptic vesicles into the synaptic cleft. Noradrenaline molecules bind to their receptors on the post-synaptic membrane and the nerve impulse is propagated or inhibited, depending on the specific receptor. Noradrenaline molecules are then released from their receptors and taken back into the nerve terminal via the noradrenaline re-uptake transporter.

31
Serotonin The link between low synaptic serotonin level and depression is supported by the fact that the cerebrospinal fluid in depressed patients contains less of a major serotonin byproduct, signifying lower levels of serotonin in the brain (McNeal, 1986).
.")
32
Anti-depressant Medication

33
Anti-depressant Medication

34
Anti-depressant Medication
The biology of serotonergic antidepressants: When neurotransmitters are released by the pre-synaptic neuron into the synaptic gap, they travel to the post-synaptic neuron. Any excess neurotransmitters are ‘taken back’ or ‘reabsorbed’ into the pre-synaptic neuron in a process known as reuptake. The sequence shown in (a) depicts the normal reuptake of excess neurotransmitters, in this case, serotonin; (b) shows how serotonergic medication actively blocks the reuptake of serotonin, meaning that the excess serotonin remains in the synaptic gap, which has a mood-enhancing effect.
 depicts the normal reuptake of excess neurotransmitters, in this case, serotonin; (b) shows how serotonergic medication actively blocks the reuptake of serotonin, meaning that the excess serotonin remains in the synaptic gap, which has a mood-enhancing effect.")
35
Anti-depressant Medication
5-HT is one of the primary neurotransmitters implicated in depression. Most neural serotonin is synthesized by cells in the raphe nuclei of the brainstem. Serotonergic cells in the raphe nuclei send projections that innervate and affect many brain regions associated with symptoms of depression . Serotonergic function is thought to be reduced in depressed patients; selective serotonin reuptake inhibitors (SSRIs) and serotonin norepinephrine reuptake inhibitors (SNRIs) are widely used in attempts to restore that function.
 and serotonin norepinephrine reuptake inhibitors (SNRIs) are widely used in attempts to restore that function.")
36
Video Link Dr Tim Johnson

37
A genetic predisposition alone, however, is unlikely to cause depression. Other factors, such as traumatic childhood or adult life events, may act as triggers. The onset of depression may also be influenced by what we learn as children. Some people may have been exposed to the depressive symptoms of their parents and have learned this as a way of reacting to certain problems. As adults, they may go on to use these strategies to deal with their own life stressors.

38
Psychological Factors
learned helplessness stress the use of psychotherapies in management including cognitive behavioural therapy and psychodynamic psychotherapy

39
Psychological Factors
Psychological factors influencing depression include characteristic negative patterns of thinking, deficits in coping skills, judgment problems, and impaired emotional intelligence (the ability to perceive, understand, and express emotions) that depressed people tend to exhibit.
 that depressed people tend to exhibit.")
40
The cognitive distortions experienced by depression sufferers cannot be treated by medication, so CBT is used to modify the distortions.

41
Psychological Factors
Personality style, and the way you deal with problems, may contribute to the onset of depression. If you are the type of person who has a low opinion of yourself and worries a lot, if you are overly dependent on others, if you are a perfectionist and expect too much from yourself or others, or if you tend to hide your feelings, you may be at greater risk of becoming depressed.

42
Learned Helplessness Seligman’s research

43
Seligman’s Research Seligman (1975) found that when dogs were restrained in an apparatus and given electric shocks, they failed to initiate escape behaviour when the restraints were removed. Moreover, they exhibited some of the symptoms of depression found in humans (lethargy, sluggishness, and appetite loss).
 found that when dogs were restrained in an apparatus and given electric shocks, they failed to initiate escape behaviour when the restraints were removed. Moreover, they exhibited some of the symptoms of depression found in humans (lethargy, sluggishness, and appetite loss).")
44
Seligman proposed that depression results from a tendency to give up passively in the face of unavoidable stressors. The sufferer does not believe desirable outcomes are achievable, but that undesirable outcomes are probable, and that their own actions won’t affect the outcome.

45
Stress

47
Stress Depression can start with stress.
It is also associated with loss. Sometimes it is a very real loss like the death of a loved one, or the loss of a job. It can also be an internal loss, like a loss of self-esteem. Stress is not the same for two people. An event that one person might find to be hugely stressful might cause no stress to another. It all depends about how the situation is viewed.

48
Two Salesmen You have two salesmen and neither of them closes a particular sale. The one salesman says ‘Oh, darn it, I’m useless as a salesman, I’ll never make it, I may as well just give up’. How is this man going to feel? Without a doubt he will feel down in the dumps. Whereas the other salesman who didn’t close the deal might say ‘Well I can learn from that experience. I think I need to polish up on some of my selling techniques so I can do better the next time’. These thoughts won’t pull him into depression.

49
The Phone Call You phone an acquaintance, leave a message for him to phone you and he doesn’t return your call. What goes on in your mind? Maybe thoughts like ‘what did I do wrong? He can’t like me if he doesn’t bother to return my call and if he can’t be bothered to phone me – well I won’t bother with him any more!’ These thoughts will lead to a loss of self-esteem and make you feel down. On the other hand your thoughts may go along these lines. ‘I wonder if he got my message, or maybe he’s forgotten as he’s busy. Anyway, let me give him a ring to find out.’ These thoughts won’t lead to depression and internal stress as they are grounded in reality.

50
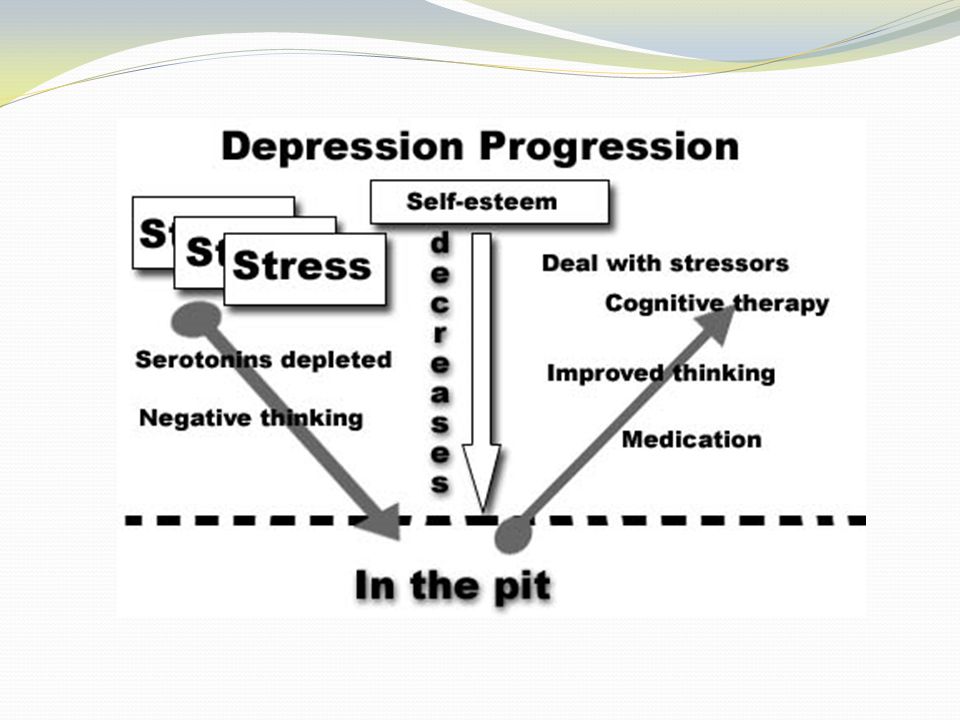
Stress Leads to Decreased Serotonin
Thoughts are transmitted in the brain by travelling as an electrical impulse along one nerve and across the synapse to the next nerve. A chemical messenger (serotonin) facilitates this move. This chemical gets depleted if the person is subject to an excessive amount of stress with no time for the chemical to naturally replenish itself between the stressful events. A symptom of this chemical being depleted is the negative thoughts that are a symptom of depression. Basically the thinking process short-circuits and the thoughts are not transferred properly. The negative thinking is a symptom that there is a physical illness and the person needs medical treatment to restore the chemical level.
 facilitates this move. This chemical gets depleted if the person is subject to an excessive amount of stress with no time for the chemical to naturally replenish itself between the stressful events. A symptom of this chemical being depleted is the negative thoughts that are a symptom of depression. Basically the thinking process short-circuits and the thoughts are not transferred properly. The negative thinking is a symptom that there is a physical illness and the person needs medical treatment to restore the chemical level.")
51
Psychotherapies Cognitive Behavioural Therapy Psychodynamic Therapy

52
B. Cognitve Behaviour Therapy
An essential part of any treatment program for major depression Psychotherapies Insight / Inward oriented A. Psychodynamic B. Cognitve Behaviour Therapy Outcome / External oriented

53
Cognitive Behavioural Therapy
This is therapy that is structured and focuses on current, rather than childhood, issues. In interpersonal therapy, people examine their depression in the context of relationships that may be contributing to their mood difficulties. Cognitive behavioural therapy helps people examine how they interpret events around them, and how negative thoughts contribute to and maintain a depressed mood.

54
Psychotherapy Psychotherapy is often used along with medication to treat depression. Psychotherapy is a general term used to describe a form of treatment that is based on “talking work” done with a therapist. The aim is to relieve distress by discussing and expressing feelings, to help change attitudes, behaviour and habits that may be unhelpful, and to promote more constructive or adaptive ways of coping.

55
Socio-cultural Factors
Abuse Poverty Social Isolation Psychosocial Stress Support factors including family and social networks and recovery groups

56
Risk Factors Abuse Poverty Social Isolation Psychosocial Stress

57
Risk Factors Some studies suggest that early childhood trauma and losses, such as the death or separation of parents, or adult life events, such as the death of a loved one, divorce, the loss of a job, retirement, serious financial problems, and family conflict, can lead to the onset of depression.

58
Risk Factors Suffering several severe and prolonged difficult life events increases a person’s chances of developing a depressive disorder. Once depressed, it is common for a person to remember earlier traumatic life events, such as the loss of a parent, or childhood abuse, which make the depression worse.

59
Risk Factors Living with chronic family problems can also seriously affect a person’s mood and lead to depressive symptoms.

60
Risk Factors People living in emotionally abusive or violent relationships can feel trapped, both financially and emotionally, and feel hopeless about their future. This is particularly true of mothers with young children. The ongoing stress and social isolation associated with these family circumstances can lead to depressive symptoms.

61
Risk Factors People can also become depressed as a result of social factors such as: experiencing traumatic situations, early separation, lack of social support, or harassment (bullying). Research has shown that stressful social events are capable of serving as triggers for turning genes on and off, causing changes in brain functioning.
. Research has shown that stressful social events are capable of serving as triggers for turning genes on and off, causing changes in brain functioning.")
62
Social Factors Depressed people tend to be more socially isolated than other people, and the relationship between the lack of social support and depression is likely to be two-way. People with poor social skills may be more likely to develop depression. Once people are depressed, they tend to be unpleasant company, causing social rejection that further reduces their social support. An awareness that your social skills are deficient can further contribute to depression.

63
Support Factors Including family and social networks and recovery groups

64
Support Groups Therapy can also be provided in a group context.
Meeting with eight to 12 other people who are struggling with similar issues can help reduce a person’s sense of isolation. The kind of support, understanding and feedback found in group therapy may not be available within a person’s own natural social network.

65
Interactive Nature Biopsychosocial Model

66
Interactive Nature In a general sense, depression is caused by an imbalance in chemical messengers in the brain called neurotransmitters; however, a variety of factors - including your genetic makeup, your environment, your physical condition and your psychological coping resources - interact together to determine whether you will develop depression.

67
Interactive Nature A genetic predisposition alone, however, is unlikely to cause depression. Other factors, such as traumatic childhood or adult life events, may act as triggers. The onset of depression may also be influenced by what we learn as children. Some people may have been exposed to the depressive symptoms of their parents and have learned this as a way of reacting to certain problems. As adults, they may go on to use these strategies to deal with their own life stressors.

69
Depression: A Primer

70
ASSESSMENT IDEA Media Response

Similar presentations







 (presentation adapted from medschool.umaryland.edu/minimed/ powerpoint/rachbeisel.ppt.>")













