Download presentation
Presentation is loading. Please wait.

1
SPAN Networking and the National Picture: Where are We and Where are We Going? Dr. Lee B. Jordan Lead Clinician for SPAN Consultant Pathologist, NHS Tayside Scottish Pathology Network

2
SPAN Networking, Quality and All That Jazz…

3
SPAN Just what is Networking and who is this Barnes chap anyway?

4
SPAN Overview What is SPAN? – Context, History, Structure. What have WE done? – Achievements to date. What are WE doing? – Current and future objectives. Quality & Performance – Kings Mill, Barnes, etc.

5
SPAN Mission Statement To improve pathology services by creating and developing a Scotland wide Managed Diagnostic Network (MDN) which will steer modernisation, including service change and redesign, improve quality, ensure provision of an effective pathology service which anticipates and responds to user needs, future requirements, national guidelines and meets Clinical Pathology Accreditation Standards'
 which will steer modernisation, including service change and redesign, improve quality, ensure provision of an effective pathology service which anticipates and responds to user needs, future requirements, national guidelines and meets Clinical Pathology Accreditation Standards")
6
SPAN What is SPAN? 10 Boards supplying cellular pathology services across 12 laboratory sites.

7
SPAN What is SPAN? Formed 2005 – Derek Bishop & Frank Carey (NHS Tayside). SPAN Steering Group – All Lead Clinicians from all departments/Boards. – All Cell Path Managers/Lead BMS. – Others: Scottish Cervical Cytopathology Consortia. Cell Path Managers Group. Postgraduate education, academia, PathAlba, NSD.

8
SPAN What is SPAN? Funding – Initially pump primed for 2 years by Scottish Government. – SPAN recurrent funding direct from Boards as agreed with Chief Executives on an NRAC formula from 2007 to 2013. – 2013/14 onwards funding from Boards provided via NSD. – NHS Tayside was host Board until end 2013/14.

9
SPAN What is SPAN? Accountability – Reported originally to South East & Tayside (SEAT) Regional Planning Group and then to the Diagnostic Steering Group (DSG) now to NSD. – Work Plan agreed with Network Steering Group, DSG and NSD. – Performance reviewed by means of progress reports submitted to NSD biannually and presented to DSG.
 Regional Planning Group and then to the Diagnostic Steering Group (DSG) now to NSD. – Work Plan agreed with Network Steering Group, DSG and NSD. – Performance reviewed by means of progress reports submitted to NSD biannually and presented to DSG..")
10
SPAN (NMDN) SEAT (SGHSCD) DSG STRATEGIC OVERSIGHT NHS Boards/Pathology Departments Historic Administrative Structure for SPAN NHS Boards Network Manager Management Logistics Scientific expertise Specialist expertise Liaison Network Manager Management Logistics Scientific expertise Specialist expertise Liaison Lead Clinician Scientific/Medical expertise Specialist expertise Liaison Lead Clinician Scientific/Medical expertise Specialist expertise Liaison Steering Group Scientific/Medical expertise Specialist expertise Strategic Direction Steering Group Scientific/Medical expertise Specialist expertise Strategic Direction FUNDING WoSPG RCPEs NoSPG Phase 1 Phase 2 ACCOUNTABILITY & STRATEGIC OVERSIGHT NSD ACCOUNTABILITY & FUNDING Phase 3 FUNDING
 SEAT (SGHSCD) DSG STRATEGIC OVERSIGHT NHS Boards/Pathology Departments Historic Administrative Structure for SPAN NHS Boards Network Manager Management Logistics Scientific expertise Specialist expertise Liaison Network Manager Management Logistics Scientific expertise Specialist expertise Liaison Lead Clinician Scientific/Medical expertise Specialist expertise Liaison Lead Clinician Scientific/Medical expertise Specialist expertise Liaison Steering Group Scientific/Medical expertise Specialist expertise Strategic Direction Steering Group Scientific/Medical expertise Specialist expertise Strategic Direction FUNDING WoSPG RCPEs NoSPG Phase 1 Phase 2 ACCOUNTABILITY & STRATEGIC OVERSIGHT NSD ACCOUNTABILITY & FUNDING Phase 3 FUNDING")
11
SEAT NoSPG WoSPG NHS Boards SGHSCD NSS Committee NSD NMCN Management Service WoSCAN Network Office New Administrative Structure Part 1 NMCNs National Cancer MCNs (SGHSCD) DSG NMDNs (incl. SPAN) NMDNs (incl. SPAN) INFORM STRATEGIC OVERSIGHT ACCOUNTABILITY Provides strategic direction to individual networks and links with national and regional planning structures Commissions NMCNs/NMDNs – agreeing objectives, funding and performance management. Accountable to SGHSCD and NHS Boards via NSC
 NMDNs (incl. SPAN) INFORM STRATEGIC OVERSIGHT ACCOUNTABILITY Provides strategic direction to individual networks and links with national and regional planning structures Commissions NMCNs/NMDNs – agreeing objectives, funding and performance management. Accountable to SGHSCD and NHS Boards via NSC.")
12
NSD NMCN Management Service New Administrative Structure Part 2 Management Arm ?29 x AfC band 7 Manage multiple networks No specialty experience Mix of current managers, coordinators, administrators Overlap with logistics as Management Service develops Management Arm ?29 x AfC band 7 Manage multiple networks No specialty experience Mix of current managers, coordinators, administrators Overlap with logistics as Management Service develops (SGHSCD) DSG SPAN (NMDN) STRATEGIC OVERSIGHT ACCOUNTABILITY & FUNDING Logistics Arm Information Management Continuous Quality Improvement/Education Comms/Engagement Clinical Leadership & Specialist Expertise (seconded) Logistics Arm Information Management Continuous Quality Improvement/Education Comms/Engagement Clinical Leadership & Specialist Expertise (seconded) LEAD CLINICIANSCIENTIFIC MANAGER STEERING GROUP NHS Boards/Pathology Departments Proposed by Lead Clinician and accepted by NSD
 DSG SPAN (NMDN) STRATEGIC OVERSIGHT ACCOUNTABILITY & FUNDING Logistics Arm Information Management Continuous Quality Improvement/Education Comms/Engagement Clinical Leadership & Specialist Expertise (seconded) Logistics Arm Information Management Continuous Quality Improvement/Education Comms/Engagement Clinical Leadership & Specialist Expertise (seconded) LEAD CLINICIANSCIENTIFIC MANAGER STEERING GROUP NHS Boards/Pathology Departments Proposed by Lead Clinician and accepted by NSD")
13
KEY DSG = DIAGNOSTIC STEERING GROUP (PART OF SGHSCD) NoSPG = NORTH OF SCOTLAND PLANNING GROUP NSS = NATIONAL SPECIALIST SERVICES NSD = NATIONAL SPECIALIST SERVICES DIVISION MCN = MANAGED CLINICAL NETWORK NMCN = NATIONAL MANAGED CLINICAL NETWORK NMDN = NATIONAL MANAGED DIAGNOSTIC NETWORK RCPEs = REGIONAL PLANNING CHIEF EXECUTIVES GROUP SEAT = SOUTH EAST AND TAYSIDE REGIONAL PLANNING GROUP SGHSCD = SCOTTISH GOVERNMENT HEALTH AND SOCIAL CARE DIRECTORATES WoSCAN = WEST OF SCOTLAND CANCER NETWORK WoSPG = WEST OF SCOTLAND PLANNING GROUP
 NoSPG = NORTH OF SCOTLAND PLANNING GROUP NSS = NATIONAL SPECIALIST SERVICES NSD = NATIONAL SPECIALIST SERVICES DIVISION MCN = MANAGED CLINICAL NETWORK NMCN = NATIONAL MANAGED CLINICAL NETWORK NMDN = NATIONAL MANAGED DIAGNOSTIC NETWORK RCPEs = REGIONAL PLANNING CHIEF EXECUTIVES GROUP SEAT = SOUTH EAST AND TAYSIDE REGIONAL PLANNING GROUP SGHSCD = SCOTTISH GOVERNMENT HEALTH AND SOCIAL CARE DIRECTORATES WoSCAN = WEST OF SCOTLAND CANCER NETWORK WoSPG = WEST OF SCOTLAND PLANNING GROUP")
14
SPAN Achievements Benchmarking Re-design of Cervical Cytology Implementation of Molecular Pathology as a National Service Review of Electron Microscopy Workforce Planning Quality Agenda Digital Imaging Site Visits Facilitating cross Board communication and support

15
SPAN Cervical Snippets Managed Service Contract Imager Consortia Model Workload distribution Workforce modelling Screening Programme changes Primary HR-HPV testing? – Tim Palmer’s talk…

16
SPAN

17
Molecular Pathology Snippets NSD adminstered, centrally funded service – Boards top-sliced Four core centres – Aberdeen, Dundee, Edinburgh, Glasgow Known repertoire ‘Free’ at the point of use Structure for evaluation and introduction of new tests – MPEP & MPCSG http://www.nsd.scot.nhs.uk/services/specserv/molpath.html

18
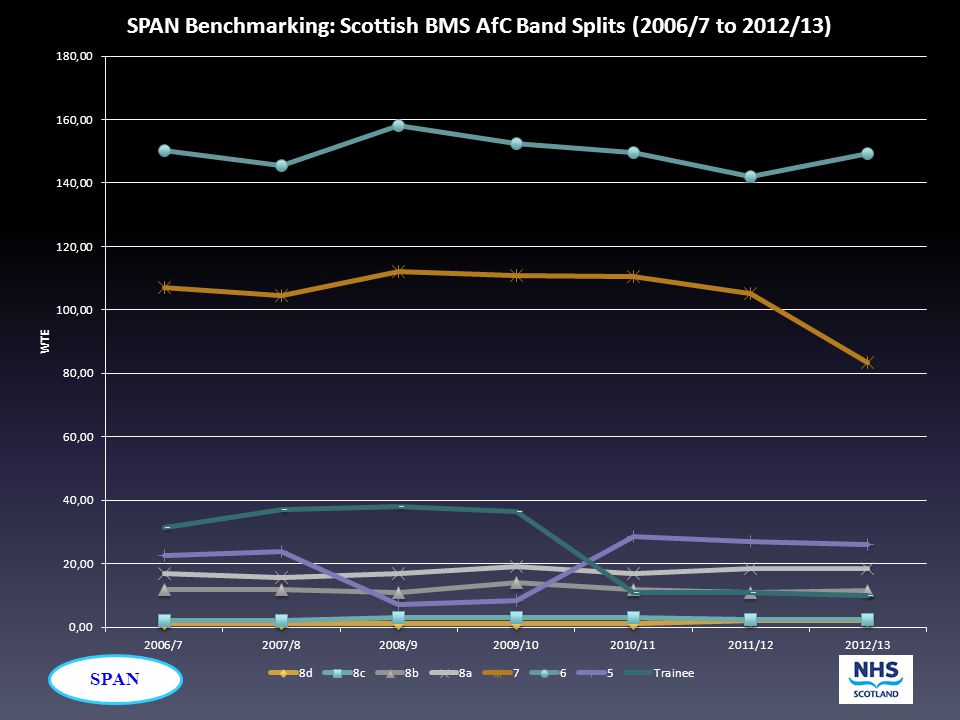
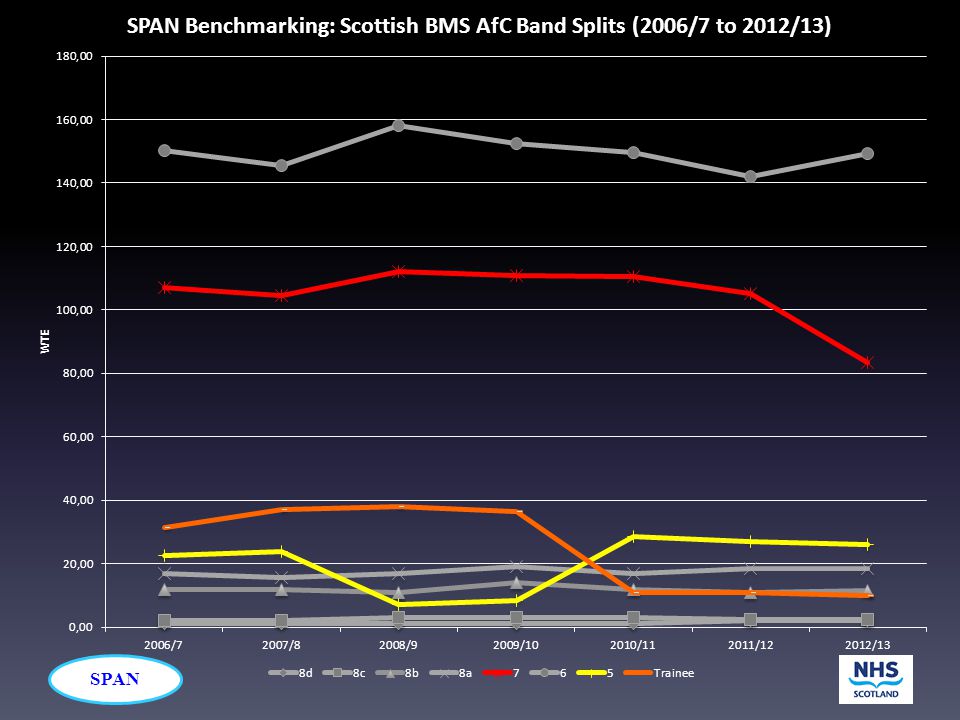
SPAN Benchmarking Snippets

19
SPAN

21
Note these are SPAN figures not SCSP figures

22
SPAN

23
49% 76%

24
SPAN 34% 12%

25
SPAN RCPath KPI 6.4 Cellular Pathology Reporting Turnaround Times – Reported, confirmed and authorised within 7 and 10 calendar days of the procedure – 80% (7 Days) – 90% (10 Days) – [Cases requiring prolonged decalcification (not bone marrow trephines) are excluded, as are cases requiring molecular tests.]
![SPAN RCPath KPI 6.4 Cellular Pathology Reporting Turnaround Times – Reported, confirmed and authorised within 7 and 10 calendar days of the procedure – 80% (7 Days) – 90% (10 Days) – [Cases requiring prolonged decalcification (not bone marrow trephines) are excluded, as are cases requiring molecular tests.]](http://images.slideplayer.com/9/2544663/slides/slide_25.jpg "SPAN RCPath KPI 6.4 Cellular Pathology Reporting Turnaround Times – Reported, confirmed and authorised within 7 and 10 calendar days of the procedure – 80% (7 Days) – 90% (10 Days) – [Cases requiring prolonged decalcification (not bone marrow trephines) are excluded, as are cases requiring molecular tests.]")
26
SPAN

30
[Excluding Capital Charges, Whole Sample Mean]
![[Excluding Capital Charges, Whole Sample Mean]](http://images.slideplayer.com/9/2544663/slides/slide_30.jpg "[Excluding Capital Charges, Whole Sample Mean]")
31
SPAN

32
[Excluding Capital Charges, Whole Sample Mean]
![[Excluding Capital Charges, Whole Sample Mean]](http://images.slideplayer.com/9/2544663/slides/slide_32.jpg "[Excluding Capital Charges, Whole Sample Mean]")
33
SPAN

34
Key Objectives Appoint a Network Scientific Manager Consolidating/reinforcing existing activity – Cervical Cytology – Molecular Pathology New activity – Paediatric & Perinatal Pathology Services Review – Quality & Performance

35
SPAN Key Objectives Appoint a Network Scientific Manager Consolidating/reinforcing existing activity – Cervical Cytology – Molecular Pathology New activity – Paediatric & Perinatal Pathology Services Review – Quality & Performance

36
SPAN Quality & Performance IQA QMS UKAS/CPA –> ISO 15189 RCPath KPI SPAN Benchmarking Keele Benchmarking QPIs (Cancer Specific) Targets (Cancer & General) Pathology Quality Assurance Review (Barnes)
 Targets (Cancer & General) Pathology Quality Assurance Review (Barnes)")
37
SPAN Quality & Performance IQA QMS UKAS/CPA –> ISO 15189 RCPath KPI SPAN Benchmarking Keele Benchmarking QPIs (Cancer Specific) Targets (Cancer & General) Pathology Quality Assurance Review (Barnes)
 Targets (Cancer & General) Pathology Quality Assurance Review (Barnes)")
38
SPAN Barnes Report… England! 28 th January 2014 To understand Barnes One must understand Kings Mill! (Not the loaf)
.")
39
SPAN Kings Mill

40
SPAN Kings Mill (1) “inadequate assurance processes at Sherwood Forest Hospitals NHS Foundation Trust, which subsequently resulted in inappropriate care for a number of women with breast cancer”. What happened? ER +ve breast cancers were called negative denying patients treatment.

41
SPAN Kings Mill (2) CQC found: – Histopathology services had poor communication and feedback with the local trust board. – Equipment in use at the time had been outdated. – Recruitment issues around medical staffing and medical leadership. – No robust internal quality audit programme in place.

42
SPAN Kings Mill (3) RCPath found: – Kings Mill was NOT an outlier on ER results as the sample size was too small for statistical analysis. – Samples were NOT misreported, there was no medical/interpretative error. – There were problems with IHC service, these were flagged and the service outsourced. – Issues around governance and culture – finance had overridden service planning and provision

43
SPAN Kings Mill (4) RCPath found: – EQA scheme for ER did NOT identify any problems. – EQA scheme did NOT provide any benchmark comparison for the Kings Mill histopathology service to relate to. – External monitoring, peer review, accreditation and QA systems did NOT identify any problem.

44
SPAN Kings Mill (5) In summary: – Specific local issues had been found at Kings Mill: small screening centre small workload behind in technological terms – National issues Quality assurance Communication Monitoring of quality Applicable beyond Kings Mill…
 In summary: – Specific local issues had been found at Kings Mill: small screening centre small workload behind in technological terms – National issues Quality assurance Communication Monitoring of quality Applicable beyond Kings Mill…")
45
SPAN

46
Pathology QA Review (1) Key positives: – Underwrites 80% of patient interactions. – Compare favourably with Europe and others. – High quality services. – High clinician confidence. – Skilled workforce. – Good IQA and QMS. – Mature EQA. – Forefront of QA (in the world). – Overall = safe, reliable and effective.
. – Overall = safe, reliable and effective..")
47
SPAN Pathology QA Review (2) Key negatives: – Relies almost entirely on professionalism and goodwill. – Setup to provide assurance to laboratories and not public or patients. – Systems focussed on minimal acceptable standards. – No identification, incentivisation or reward for excellence. – Little sanction or support if performance falls below acceptable standards.

48
SPAN Recommendation 1 “A systematic approach should be taken to educating, training and developing the skills of the pathology workforce in quality management systems and quality improvement methodology, in ways appropriate to professional group, role and grade. This process should be led by HEE [Higher Education England].” “HEE should work with the professional bodies and regulators to ensure that quality management and assurance can be recognised as an essential requirement in CPD [Continuing Professional Development], and in individual appraisal requirements.”

49
SPAN Implication – R1 If Scotland were to adopt: – NHS Education for Scotland (NES) would be the surrogate for HEE ? – Medical deaneries and other parties? – Educational mechanisms (appraisal, PDRs, CPD, eKSF, etc.). – Could be beneficial for ALL of the Pathology Team.
. – Could be beneficial for ALL of the Pathology Team..")
50
SPAN Recommendation 2 (1) “The membership, role and function of the JWGQA [Joint Working Group for Quality Assurance] should be revised and expanded. It should set consistent standards and performance criteria for all schemes across pathology and work with UKAS [UK Accreditation Service] to ensure their implementation in the scheme accreditation process. The JWGQA should advise on publication of performance data. The National Medical Director has confirmed that he will ask the RCPath to lead this work.”
![SPAN Recommendation 2 (1) The membership, role and function of the JWGQA [Joint Working Group for Quality Assurance] should be revised and expanded.](http://images.slideplayer.com/9/2544663/slides/slide_50.jpg "It should set consistent standards and performance criteria for all schemes across pathology and work with UKAS [UK Accreditation Service] to ensure their implementation in the scheme accreditation process. The JWGQA should advise on publication of performance data. The National Medical Director has confirmed that he will ask the RCPath to lead this work. .")
51
SPAN Recommendation 2 (2) “Further consideration must be given to the ways in which individual performance can be assessed, monitored and competence-assured. The National Medical Director will ask the professional bodies, led by RCPath, to review these issues and report back within twelve months on their findings.”

52
SPAN Implication – R2 (1) Scottish impact (1): – JWGQA is UK wide. ?devolved nation representation. – Laboratory (technique) EQA: Little/no objection in Scotland for transparency. Output unlikely to be informative to the public. Unlikely to be understandable without review.
 EQA: Little/no objection in Scotland for transparency. Output unlikely to be informative to the public. Unlikely to be understandable without review..")
53
SPAN Implication – R2 (2) Scottish impact: – Interpretative EQA (individual performance): Much more concern here. Developed from informal slide clubs, internal learning and professional development perspective. Currently (mostly) voluntary, performance output is linked anonymised. Each scheme differs – own scoring/exclusion/answering/marking/analysis/result reporting processes. Not all are CPA accredited.
 voluntary, performance output is linked anonymised. Each scheme differs – own scoring/exclusion/answering/marking/analysis/result reporting processes. Not all are CPA accredited..")
54
SPAN Implication – R2 (3) Scottish impact: – Interpretative EQA (individual performance): Not reflective of practice or in-service performance. Schemes prohibit consultation and consensus, which are key aspects to service delivery and QA in labs. Review states that attempts at collusion should be a matter of professional probity. EQA responses are a matter of opinion. English use for commissioning. Current EQA is not fit for R2 purpose?

55
SPAN Recommendation 3 “The quality and governance systems of pathology providers must be integrated with trust governance and quality structures. This should include the measurement of appropriate quality assurance indicators and the identification of an accountable board member within the organisation. CQC and the Chief Inspector of Hospitals have indicated that robust information on the quality of pathology services could contribute to the overall assessment of quality under the new hospital inspection model.”

56
SPAN Implication – R3 For Scotland: – There should be some input into any development of KPIs or KAIs that may impact Scotland. – How to achieve that? – Should we develop our own? – Should we simplify matters?

57
SPAN Recommendation 4 “Existing guidance on the standardisation and transparent reporting of errors from pathology services must be rigorously followed, including the reporting of all incidents that could have, or did lead to patient harm, to the NRLS [National Reporting and Learning System]. Pathology services should be encouraged to share information and data about clinical risks, ‘lessons learnt’ and good practice, in order to contribute to education and quality improvements nationally. The Trust Development Agency (TDA) and Monitor/CQC should encourage trusts to improve their adherence to existing guidance.”
![SPAN Recommendation 4 Existing guidance on the standardisation and transparent reporting of errors from pathology services must be rigorously followed, including the reporting of all incidents that could have, or did lead to patient harm, to the NRLS [National Reporting and Learning System].](http://images.slideplayer.com/9/2544663/slides/slide_57.jpg "Pathology services should be encouraged to share information and data about clinical risks, ‘lessons learnt’ and good practice, in order to contribute to education and quality improvements nationally. The Trust Development Agency (TDA) and Monitor/CQC should encourage trusts to improve their adherence to existing guidance. .")
58
SPAN Implication – R4 For Scotland: – Already have local mechanisms for reporting. – Part of QMS and Board mechanisms. – Part of UKAS/CPA review. – Should there be sharing beyond host organisations? – Do we need another system?

59
SPAN Recommendation 5 “The continued development of the NLMC [National Laboratory Medicines Catalogue] to ensure consistency of data and information across the NHS in England should remain a priority. Ministers and NHS England have confirmed that this task, undertaken by HSCIC [Health & Social Care Information Centre], with support from professional bodies and others, must continue at scale and pace. The professional bodies, the IVD [in vitro Diagnostics] manufacturers and others should work towards minimising the differences between analytical processes, requesting and reporting.”
![SPAN Recommendation 5 The continued development of the NLMC [National Laboratory Medicines Catalogue] to ensure consistency of data and information across the NHS in England should remain a priority.](http://images.slideplayer.com/9/2544663/slides/slide_59.jpg "Ministers and NHS England have confirmed that this task, undertaken by HSCIC [Health & Social Care Information Centre], with support from professional bodies and others, must continue at scale and pace. The professional bodies, the IVD [in vitro Diagnostics] manufacturers and others should work towards minimising the differences between analytical processes, requesting and reporting. .")
60
SPAN Implication – R5 For Scotland: – Already committed for NLMC. More impact for non-Cell Path labs.

61
SPAN Recommendation 6 “In order that patients and clinicians can rely on accreditation status as shorthand for a quality assured service, the accreditation of pathology services must be updated showing clearly which laboratories are meeting minimum requirements, and which are excelling to provide first-rate service quality. UKAS has agreed to undertake this work.”

62
SPAN Implication – R6 (1) For Scotland: – Particular risks for Scotland: CPA/UKAS is often a struggle and a rush. ISO 15189 is proving challenging, esp. Test Validation. May see labs accredited minus aspects of their current repertoire. Introduction of random, unannounced visits. – Does inspection improve standards? Too late? Need to embed Continuous Quality Improvement.

63
SPAN Implication – R6 (2) For Scotland: – Overlap with R2 and EQA elements. – “4.80 - UKAS should work with the professional bodies and JWGQA to facilitate an assessment of the minimum number of specimens per annum required to quality assure an individual test.” Kings Mill reports suggest minimum numbers of ER tests at any one site. Minimum limits on reporting size and duties for reporters.

64
SPAN Recommendation 7 “In order to support commissioners in the next planning round, the PSCT [Pathology Commissioning Services Toolkit] should be updated. The National Clinical Director (NCD) for Pathology, with the NCD for Diagnostics and the Chief Scientific Officer, will lead this project, working in conjunction with local commissioners and professional bodies. When the NICE QS is published, it should be included in the PSCT. Commissioners should follow the MHRA guidelines when commissioning POCT.”
![SPAN Recommendation 7 In order to support commissioners in the next planning round, the PSCT [Pathology Commissioning Services Toolkit] should be updated.](http://images.slideplayer.com/9/2544663/slides/slide_64.jpg "The National Clinical Director (NCD) for Pathology, with the NCD for Diagnostics and the Chief Scientific Officer, will lead this project, working in conjunction with local commissioners and professional bodies. When the NICE QS is published, it should be included in the PSCT. Commissioners should follow the MHRA guidelines when commissioning POCT. .")
65
SPAN Implication – R7 For Scotland: – No impact? Commissioning has no role in NHS Scotland at present. – Monitoring tools suggested could be of use? Kent & Medway tools covered in the QA Review document.

66
SPAN Recommendation 8 “A high level, system-wide Oversight Group should be created with responsibility for steering the improvements in quality assurance frameworks and governance mechanisms outlined in this report. NHS England has confirmed that it will facilitate this group.” “The Oversight Group should also develop a Pathology Quality Assurance Dashboard, which draws transparent and meaningful information from existing data sources to provide a national picture of quality improvement across England, to enable trend analysis and the identification of opportunities for development of the system.”

67
SPAN Implication – R8 For Scotland: – Concept of a live Dashboard could be useful in the Scottish context. How to feed in to the process?

68
SPAN

69
Quality & Performance IQA QMS UKAS/CPA –> ISO 15189 RCPath KPI SPAN Benchmarking Keele Benchmarking QPIs (Cancer Specific) Targets (Cancer & General) Pathology Quality Assurance Review (Barnes)
 Targets (Cancer & General) Pathology Quality Assurance Review (Barnes)")
70
SPAN Quality & Performance Is there a simpler way forward? (September)
")
Similar presentations
















>")




 for Responsible Officers and Revalidation Ahead of the Curve RO conference 4 June 2014.>")