Download presentation
Presentation is loading. Please wait.

1
การให้ยาระงับความรู้สึกในผู้ป่วยโรคเบาหวานและโรคต่อมไทรอยด์
พญ.รัตนาภรณ์ บุริมสิทธิชัย ภาควิชาวิสัญญีวิทยา โรงพยาบาลจุฬาลงกรณ์

2
การให้ยาระงับความรู้สึกในผู้ป่วยโรคเบาหวาน

3
Criteria for the diagnosis of DM
FPG ≥126 mg/dl (NPO at least 8 h) or Symptoms of hyperglycemia (polyuria, polydipsia and unexplained weight loss) and a casual plasma glucose ≥200 mg/dl (any time) or 2-h plasma glucose ≥200 mg/dl during an OGTT Repeat testing on a different day
 or. Symptoms of hyperglycemia (polyuria, polydipsia and unexplained weight loss) and a casual plasma glucose ≥200 mg/dl (any time) or. 2-h plasma glucose ≥200 mg/dl during an OGTT. Repeat testing on a different day.")
5
Impaired fasting glucose (IFG) Impaired glucose tolerance (IGT)
Fasting plasma glucose levels ≥100 mg/dl but <126mg/dl or 2-h values in the OGTT of ≥140 mg/dl but <200 mg/dl Pre-diabetes Associate with the metabolic syndrome : obesity, dyslipidemia and hypertension

6
Metabolic abnormality
Hyperglycemia Osmotic diuresis, dehydration, electrolyte imbalance Lipolysis Increased serum free fatty acid, ketone Increased low density lipoproteins Protein breakdown Stress cortisol, glucagon, catecholamine, growth hormone

7
Classification of DM Type 1 Type 2 Other Gestational diabetes
Destruction of pancreatic β cells (autoimmune) Absolute insulin deficiency and requirement Type 2 Variable degrees of insulin deficiency and resistance Diet control, oral hypoglycemic drugs, insulin Other Steroid Gestational diabetes
 Absolute insulin deficiency and requirement. Type 2. Variable degrees of insulin deficiency and resistance. Diet control, oral hypoglycemic drugs, insulin. Other. Steroid. Gestational diabetes.")
8
Common insulin preparations
Onset Peak Duration Short acting -Regular -Lispro/Aspart 30-60min 5-15min 2-3h 30-90min 8-10h 4-6h Intermediate acting -NPH/Lente -Glargine 2-4h 4-10h none 12-20h 20-24h Long acting -Ultralente 6-10h 10-16h 24-48h Premixed -Humulin70/30 15-30min 2-12h 18-24h

9
Common preparations of oral hypoglycemic drugs
Duration (h) Adverse effects Sulfonylureas First generation Chlorpropamide (Diabenese) Second generation Glyburide (Glibenclamide, Daonil, Euglucon) Glipizide (Minidiab) 24-72 24 6-12 hypoglycemia cholestatic jaundice agranulocytosis Biguanide Metformin (Glucophage) 7-12 lactic acidosis (elderly, renal insufficiency) Thiazolidinediones Rosiglitazone (Avandia) Pioglitazone (Actos) increased cholesterol level Alpha-glucosidase inhibitor Acarbose 4 dyspepsia
 Adverse effects. Sulfonylureas. First generation. Chlorpropamide (Diabenese) Second generation. Glyburide (Glibenclamide, Daonil, Euglucon) Glipizide (Minidiab) hypoglycemia. cholestatic jaundice. agranulocytosis. Biguanide. Metformin (Glucophage) lactic acidosis (elderly, renal insufficiency) Thiazolidinediones. Rosiglitazone (Avandia) Pioglitazone (Actos) increased cholesterol level. Alpha-glucosidase inhibitor. Acarbose. 4. dyspepsia.")
10
Complications of DM Acute complications Chronic complications
Hypoglycemia Diabetic ketoacidosis (DKA) Hyperosmolar nonketotic coma Chronic complications Macrovascular : atherosclerosis Microvascular : diabetic retinopathy, nephropathy, neuropathy
 Hyperosmolar nonketotic coma. Chronic complications. Macrovascular : atherosclerosis. Microvascular : diabetic retinopathy, nephropathy, neuropathy.")
11
Hypoglycemia Glucose level < 50 mg/dl
Fasting, long-acting insulin/OHD, renal insufficiency Altered mental status, coma and seizure Physiologic responses to catecholamines Diabetic patient may be symptomatic at higher glucose level Anesthetized patient, beta blocker 50 ml of 50% glucose IV

12
Diabetic ketoacidosis (DKA)
Type 1 DM Metabolism of free fatty acid Glucose mg/dl, increased anion gap metabolic acidosis Dehydration, osmotic diuresis, Kussmaul breathing, fruity breath, nausea and vomiting, abdominal pain, ileus, leukocytosis and elevated amylase level Precipitating factors : infection, surgical stress, trauma, lack of insulin therapy

13
Management of diabetic ketoacidosis
Identify and treat precipitating causes RI 10 unit IV bolus followed by an infusion at blood glucose/150 unit/hr NSS infusion : vital signs and urine output Potassium replacement when urine output > 0.5 ml/kg/hr Add 5%dextrose infusion when glucose decreased to 250 mg/dl Serial glucose and electrolyte level Hemodynamic monitoring

14
Hyperosmolar nonketotic coma
Type 2 DM under stress Glucose level > 600 mg/dl Profound dehydration, confusion, coma and seizures Intravascular thrombosis Volume resuscitation : NSS Rapid correction of hyperosmolarity leading to cerebral edema

15
Preoperative evaluation
Preoperative glucose level control Fasting blood glucose HbA1c < 7 mg/dl End organ dysfunction Atherosclerosis Coronary artery disease : myocardial ischemia/infarction Cardiomyopathy Peripheral vascular disease Cerebrovascular disease

16
End organ dysfunction Diabetes nephropathy Diabetic retinopathy
40-50% of DM patients Albuminuria ACEIs, ARB Diabetic retinopathy Diabetic stiff joint syndrome 40% in DM type1 Difficult laryngoscopy : decrease mobility of atlanto-occipital and tempero-mandibular joint Prayer sign Peripheral neuropathy : pressure injury

17
End organ dysfunction Diabetic autonomic neuropathy
ANS reflex dysfunction Old age, DM > 10 year, CAD and beta-blocker Limited compensation for intravascular volume changes Predispose to cardiovascular instability Exaggerated pressor response to tracheal intubation Postinduction hypotension Sudden cardiac death Intraoperative hypothermia

18
Clinical signs of diabetic autonomic neuropathy
Hypertension Silent myocardial ischemia/infarction Orthostatic hypotension Lack of HR variability Reduced HR response to atropine and propranolol Resting tachycardia Gastroparesis Neurogenic bladder Lack of sweating Impotence

19
Anesthetic management
Avoid hypoglycemia Signs and symptoms of hypoglycemia will be masked by GA, beta-blocker RA and peripheral nerve block Monitoring Blood glucose Invasive monitoring NPH vs protamine sulfate Severe bradycardia : epinephrine

20
Perioperative glycemic control
Anesthetic agents : modulation of SNS Association between hyperglycemia and increased morbidity and mortality Type, severity of DM and extent of surgery Hold short acting agents on the day of surgery, long acting agents 2-3 days prior Cardiopulmonary bypass, pregnancy, neurological surgery Goal mg/dl

21
Perioperative insulin regimen
Bolus administration ½ of the usual intermediate-acting insulin subcutaneously on the morning Regular insulin 1 unit reduce blood glucose 30 mg/dl Insulin infusion Separate IV line Regular insulin 10 unit in NSS 100 ml (1u/h=10ml/h) Blood glucose/150 = insulin unit/h 5%dextrose infusion ml/h Serial blood glucose every 1-2 h
 Blood glucose/150 = insulin unit/h. 5%dextrose infusion ml/h. Serial blood glucose every 1-2 h.")
22
Postoperative management
Continue glucose level control Osmotic diuresis Infection Poor wound healing Lactate-containing fluid Rising in blood glucose level hr postoperatively

23
การให้ยาระงับความรู้สึกในผู้ป่วยโรคต่อมไทรอยด์

25
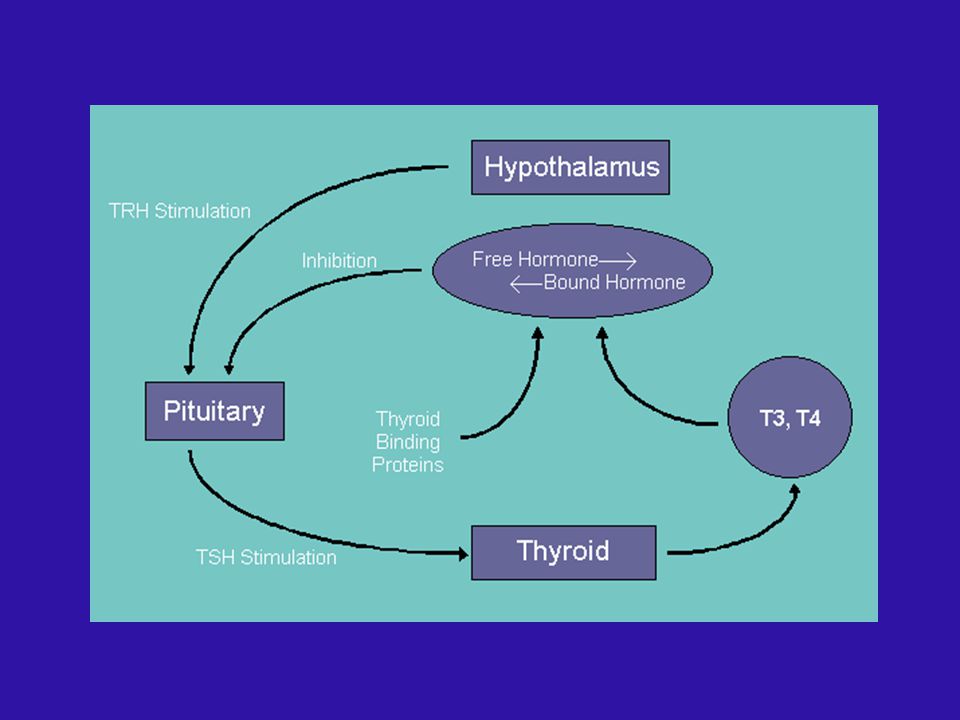
Normal plasma T4 5-12 mcg/dl
Thyroid function test Total serum triiodothyronine (T3) and thyroxine (T4) Free T3 and T4 Thyroid hormone binding rate (THBR) Thyroid stimulating hormone (TSH) Normal plasma T mcg/dl Normal plasma T ng/dl Normal THBR 30-40% Normal TSH 8 µIU/ml
 and thyroxine (T4) Free T3 and T4. Thyroid hormone binding rate (THBR) Thyroid stimulating hormone (TSH) Normal plasma T mcg/dl. Normal plasma T ng/dl. Normal THBR 30-40% Normal TSH 8 µIU/ml.")
26
Test of thyroid gland function
TSH THBR Hyperthyroidism Primary hypothyroidism Secondary hypothyroidism Pregnancy

27
Hyperthyroidism

28
Hyperthyroidism Pituitary tumor Grave’s disease Thyroid adenoma
Toxic multinodular goiter Thyroiditis Iatrogenic Exogenous iodide

29
Manifestations of hyperthyroidism
Weight loss, diarrhea, skeletal muscle weakness, hyperactive reflexes, warm and moist skin, heat intolerance, diaphoresis, nervousness Tachycardia, high CO, elevated SBP, decrease DBP, heart failure, atrial fibrillation Aggravate myocardial ischemia Increased beta receptor sensitivity

30
Manifestations of hyperthyroidism
Mild anemia, thrombocytopenia Fine tremor, exophthalmos, goiter Bone resorption and hypercalcemia

31
Hyperthyroidism Treatment Medical treatment Radioactive iodine
Antithyroid drugs : propylthiouracil, methimazole Beta adrenergic blocking agent Inorganic iodide Corticosteroid Radioactive iodine Surgical treatment Failed medical therapy, cancer, symptomatic goiter, cosmetic

32
Mechanism of action of antithyroid drugs
PTU MMI LiCO3 SSKI β blocker steroid Block Iodine uptake - ++ Block T4 synthesis +++ Block T4 release Block peripheral conversion T4 to T3 +

33
Preoperative evaluation
Euthyroid state before surgery antithyroid drugs 6-8 wk Controlled hyperdynamic CVS resting heart rate < 90 bpm Inorganic iodide : reduce size Continue medications Side effects of antithyroid drugs Rash, fever, nausea, agranulocytosis, hepatitis, arthralgia, hypothyroidism

34
Preoperative evaluation
Emergency surgery Esmolol mcg/kg/min Dexamethasone 8-12 mg/d Airway obstruction Substernal goiter X-ray neck CT Premedication Benzodiazepine Anticholinergic

35
Tracheal comprssion

36
Tracheal compression

37
Anesthetic management
Regional anesthesia General anesthesia Adequate depth of anesthesia Reinforced ETT Avoid meds that stimulate SNS Ketamine, pacuronium, indirect-acting vasopressor Thiopental : antithyroid activity

38
Anesthetic management
Chronic hypovolemia and vasodilation Exaggerated hypotension postinduction Unchanged MAC Eyes protection Maintain body temperature Myasthenia gravis

39
Thyrotoxic crisis (Thyroid storm)
Undiagnosed/uncontrolled hyperthyroid with surgical stress or illness 6-18 hr postoperative Tachycardia, dysrhythmia, CHF, MI, dehydration, shock, hyperthermia, agitation Differential diagnosis Pheochromocytoma Malignant hyperthemia Neuroleptic malignant syndrome Light anesthesia

40
Treatment of thyrotoxic crisis
Precipitating causes Cooled crystalloid solution Sodium iodide 250 mg PO or IV q 6 h PTU mg PO or NGT q 6 h Hydrocortisone mg IV q 6 h Propranolol mg PO q 4-6 h or 1-2 mg IV or esmolol infusion mcg/kg/min Cooling blanket, acetaminophen and meperidine mg IV q 4-6 h to prevent shivering Digoxin if AF with RVR

41
Post-thyroidectomy complication
Recurrent laryngeal nerve injury Unilateral bilateral Tracheal compression Hematoma Tracheomalacia Hypoparathyroidism Hypocalcemia h postoperatively Inspiratory stridor, laryngospasm

42
Hypothyroidism

43
Hypothyroidism Etiology Primary hypothyroidism
Thyroid gland dysfunction : Hashimoto’s thyroiditis, previous subtotal thyroidectomy, RIA, irradiation of the neck Thyroid hormone deficiency : antithyroid drugs, dietary iodine deficiency Secondary hypothyroidism Hypothalamic dysfunction Anterior pituitary dysfunction

44
Clinical manifestations
Reduction in metabolic activity Weight gain, lethargy, slow mental functioning, cold intolerance, slow movement Cardiovascular Bradycardia, decreased contractility, CO Increased SVR, diastolic hypertension Pericardial fluid Angina pectoris, CHF

45
Clinical manifestations
Respiratory Depressed ventilatory responsiveness to hypoxia and hypercarbia, pleural effusion Sleep apnea Renal Decreased renal blood flow, hyponatremia Anemia, coagulopathy Delayed gastric emptying, constipation

46
Clinical manifestations
Hypothermia Cool, dry and mottled extremities Blunted stress response and adrenal depression Dull facial expression, depression

47
Myxedema coma Stupor or coma, hypoventilation, hypothermia, hypotension, hyponatremia Mortality 25-50% Infection, surgery, trauma Life-threatening surgery IV thyroid hormone Precipitate myocardial ischemia Acute primary adrenal insufficiency Stress dose hydrocortisone

48
Management of myxedema
Tracheal intubation & controlled ventilation Levothyroxine mcg IV over 5-10 min then 100 mcg IV q 24 h Hydrocortisone 100 mg IV then 25 mg IV q 6 h Fluid and electrolyte therapy Warming blanket

49
Preoperative evaluation
Postpone elective surgery in severe hypothyroidism (T4 < 1 mcg/dl) Mild/moderate hypothyroidism Preoperative thyroid hormone replacement vs ischemic heart disease Difficult intubation : large tongue Premedication Sedative, thyroid hormone, steroid
 Mild/moderate hypothyroidism. Preoperative thyroid hormone replacement vs ischemic heart disease. Difficult intubation : large tongue. Premedication. Sedative, thyroid hormone, steroid.")
50
Anesthetic considerations
Increased sensitivity to depressant drugs Slow drug metabolism Decreased cardiac output, cardiac contractility Bradycardia, unresponsive baroreceptor reflexes Decreased catecholamine response Impaired ventilatory responses to arterial hypoxemia or hypercarbia Hypovolemia Hyponatremia Hypoglycemia Hypothermia Delayed gastric emptying Adrenal insufficiency

51
Anesthetic management
Regional anesthesia Decrease dose, prone to toxicity General anesthesia Susceptible to hypotensive effect of anesthetics Ketamine Thiopental Short-acting drugs Maintain normothermia

52
Postoperative care Delayed awakening Hypoventilation Hypothermia

53
Thank you for your attention

Similar presentations




>")



,Triiodothyronine T3 (9%) and rT3 (1%). Reverse T3 (rT3) is biologically inactive.>")






 55 F Graves’ disease diagnosed at 彰基 one year ago Initial presentation: sweating, good appetite, easy nervousness Physical.>")


 is an acute state of hyperthyroidism where all of the signs and symptoms are exaggerated.>")

