Download presentation
Presentation is loading. Please wait.

1
The Upper Airway and Cardiopulmonary Exercise Testing Carl Mottram, BA RRT RPFT FAARC Director - Pulmonary Function Labs & Rehabilitation Associate Professor of Medicine - Mayo Clinic College of Medicine Carl Mottram, BA RRT RPFT FAARC Director - Pulmonary Function Labs & Rehabilitation Associate Professor of Medicine - Mayo Clinic College of Medicine

2
Cardiopulmonary Exercise Testing O O 2max) O O 2max) Index of cardiopulmonary fitness (gold standard) Index of cardiopulmonary fitness (gold standard) Cardiovascular response Cardiovascular response Ventilatory limitation and breathing strategies Ventilatory limitation and breathing strategies Gas Exchange Gas Exchange Metabolic calculations and derivatives Metabolic calculations and derivatives O O 2max) O O 2max) Index of cardiopulmonary fitness (gold standard) Index of cardiopulmonary fitness (gold standard) Cardiovascular response Cardiovascular response Ventilatory limitation and breathing strategies Ventilatory limitation and breathing strategies Gas Exchange Gas Exchange Metabolic calculations and derivatives Metabolic calculations and derivatives
 O O 2max) Index of cardiopulmonary fitness (gold standard) Index of cardiopulmonary fitness (gold standard) Cardiovascular response Cardiovascular response Ventilatory limitation and breathing strategies Ventilatory limitation and breathing strategies Gas Exchange Gas Exchange Metabolic calculations and derivatives Metabolic calculations and derivatives O O 2max) O O 2max) Index of cardiopulmonary fitness (gold standard) Index of cardiopulmonary fitness (gold standard) Cardiovascular response Cardiovascular response Ventilatory limitation and breathing strategies Ventilatory limitation and breathing strategies Gas Exchange Gas Exchange Metabolic calculations and derivatives Metabolic calculations and derivatives")
3
Determinates of Exercise Ventilatory Response Ventilatory demand Ventilatory demand Metabolic demand Metabolic demand Neuroregulatory and behavior factors Neuroregulatory and behavior factors Dead space ventilation Dead space ventilation Body weight Body weight Mechanical limitations imposed by lungs and chest wall Mechanical limitations imposed by lungs and chest wall Chest wall deformity Chest wall deformity Ventilatory demand Ventilatory demand Metabolic demand Metabolic demand Neuroregulatory and behavior factors Neuroregulatory and behavior factors Dead space ventilation Dead space ventilation Body weight Body weight Mechanical limitations imposed by lungs and chest wall Mechanical limitations imposed by lungs and chest wall Chest wall deformity Chest wall deformity

4
Determinates of Exercise Ventilatory Response Mechanical limitations imposed by lungs Mechanical limitations imposed by lungs Intrinsic Lung Disease Intrinsic Lung Disease Obstructive pulmonary disease Obstructive pulmonary disease Restrictive disease Restrictive disease Airway tone Airway tone Bronchodilation or bronchoconstriction Bronchodilation or bronchoconstriction Upper airway Upper airway Mechanical limitations imposed by lungs Mechanical limitations imposed by lungs Intrinsic Lung Disease Intrinsic Lung Disease Obstructive pulmonary disease Obstructive pulmonary disease Restrictive disease Restrictive disease Airway tone Airway tone Bronchodilation or bronchoconstriction Bronchodilation or bronchoconstriction Upper airway Upper airway

5
Determining Ventilatory Limitation Ventilatory Capacity ( Ecap ) Ventilatory Capacity ( Ecap ) Maximal Voluntary Ventilation (MVV) Maximal Voluntary Ventilation (MVV) FEV 1 FEV 1 Flow limitation Flow limitation FV loops during exercise FV loops during exercise End-exercise PaCO 2 End-exercise PaCO 2 Ventilatory Capacity ( Ecap ) Ventilatory Capacity ( Ecap ) Maximal Voluntary Ventilation (MVV) Maximal Voluntary Ventilation (MVV) FEV 1 FEV 1 Flow limitation Flow limitation FV loops during exercise FV loops during exercise End-exercise PaCO 2 End-exercise PaCO 2
 Ventilatory Capacity ( Ecap ) Maximal Voluntary Ventilation (MVV) Maximal Voluntary Ventilation (MVV) FEV 1 FEV 1 Flow limitation Flow limitation FV loops during exercise FV loops during exercise End-exercise PaCO 2 End-exercise PaCO 2 Ventilatory Capacity ( Ecap ) Ventilatory Capacity ( Ecap ) Maximal Voluntary Ventilation (MVV) Maximal Voluntary Ventilation (MVV) FEV 1 FEV 1 Flow limitation Flow limitation FV loops during exercise FV loops during exercise End-exercise PaCO 2 End-exercise PaCO 2")
6
Ventilatory Capacity - MVV MVV – 10 - 12 second maneuver that is extrapolated to a minute ventilation MVV – 10 - 12 second maneuver that is extrapolated to a minute ventilation FEV 1 x 35 or 40 FEV 1 x 35 or 40 Advantages: Advantages: General approximation of ventilatory capacity General approximation of ventilatory capacity Readily and widely available, no analysis needed Readily and widely available, no analysis needed MVV – 10 - 12 second maneuver that is extrapolated to a minute ventilation MVV – 10 - 12 second maneuver that is extrapolated to a minute ventilation FEV 1 x 35 or 40 FEV 1 x 35 or 40 Advantages: Advantages: General approximation of ventilatory capacity General approximation of ventilatory capacity Readily and widely available, no analysis needed Readily and widely available, no analysis needed

7
Ventilatory Capacity - MVV Disadvantages: Disadvantages: Volitional effort Volitional effort Breathing strategy is different Breathing strategy is different MVV is not a sustained maneuver MVV is not a sustained maneuver MVV tested before exercise does not take into account bronchodilation MVV tested before exercise does not take into account bronchodilation Disadvantages: Disadvantages: Volitional effort Volitional effort Breathing strategy is different Breathing strategy is different MVV is not a sustained maneuver MVV is not a sustained maneuver MVV tested before exercise does not take into account bronchodilation MVV tested before exercise does not take into account bronchodilation Johnson BD, Weisman IM, Zeballos RJ, Beck KC. Chest 1999;116:488–503. Freedman S. Resp Physiology (8) 230-244, 1970
 ,")
8
Ventilatory Capacity Ventilatory or Breathing reserve: Ventilatory or Breathing reserve: Ventilatory capacity - Emax Ventilatory capacity - Emax 20-30 liters (10-15 L minimum) 20-30 liters (10-15 L minimum) 20-40% 20-40% “Ventilatory limitation” “Ventilatory limitation” Mottram CD. 10 th Ed. Ruppel’s Manual of Pulmonary Function Testing Chap. 7

9
Ventilatory Limitation

10
Flow-Volume Loop Analysis Quantify flow limitation rather than a pseudo- ventilatory capacity Quantify flow limitation rather than a pseudo- ventilatory capacity Define maximal flow-volume loop (envelope) Define maximal flow-volume loop (envelope) Use IC maneuvers to determine changes in EELV Use IC maneuvers to determine changes in EELV Johnson BD. Weisman IM. Zeballos RJ. Beck KC. Chest. 116(2):488-503, 1999 Aug Quantify flow limitation rather than a pseudo- ventilatory capacity Quantify flow limitation rather than a pseudo- ventilatory capacity Define maximal flow-volume loop (envelope) Define maximal flow-volume loop (envelope) Use IC maneuvers to determine changes in EELV Use IC maneuvers to determine changes in EELV Johnson BD. Weisman IM. Zeballos RJ. Beck KC. Chest. 116(2):488-503, 1999 Aug
: , 1999 Aug Quantify flow limitation rather than a pseudo- ventilatory capacity Quantify flow limitation rather than a pseudo- ventilatory capacity Define maximal flow-volume loop (envelope) Define maximal flow-volume loop (envelope) Use IC maneuvers to determine changes in EELV Use IC maneuvers to determine changes in EELV Johnson BD. Weisman IM. Zeballos RJ. Beck KC. Chest. 116(2): , 1999 Aug.")
11
10 normal subjects 10 normal subjects The major goal of this study was to relate the expiratory pressures during exercise to the pressures associated with flow limitation. 10 normal subjects 10 normal subjects The major goal of this study was to relate the expiratory pressures during exercise to the pressures associated with flow limitation. The Journal of Clinical Investigation Volume 48 1969

12
Flow Volume Loop Profiles Normal Flow (L/sec) 10 8 6 4 2 0 2 4 6 8 Severe COPD 1234512345 Rest Ex Mottram CD. 10 th Ed. Ruppel’s Manual of Pulmonary Function Testing Chap. 7

13
Flow-Volumes Loop Analysis Suspicion of flow limitation Suspicion of flow limitation Obstruction Obstruction Restriction Restriction Intra or extra-thoracic obstruction Intra or extra-thoracic obstruction Vocal chord dysfunction (VCD) Vocal chord dysfunction (VCD) Other pseudo-asthma - severe obesity Other pseudo-asthma - severe obesity Breathing kinetics Breathing kinetics Location of tidal breathing on the absolute lung volume scale Location of tidal breathing on the absolute lung volume scale EEVL/TLC EEVL/TLC Suspicion of flow limitation Suspicion of flow limitation Obstruction Obstruction Restriction Restriction Intra or extra-thoracic obstruction Intra or extra-thoracic obstruction Vocal chord dysfunction (VCD) Vocal chord dysfunction (VCD) Other pseudo-asthma - severe obesity Other pseudo-asthma - severe obesity Breathing kinetics Breathing kinetics Location of tidal breathing on the absolute lung volume scale Location of tidal breathing on the absolute lung volume scale EEVL/TLC EEVL/TLC
 Vocal chord dysfunction (VCD) Other pseudo-asthma - severe obesity Other pseudo-asthma - severe obesity Breathing kinetics Breathing kinetics Location of tidal breathing on the absolute lung volume scale Location of tidal breathing on the absolute lung volume scale EEVL/TLC EEVL/TLC Suspicion of flow limitation Suspicion of flow limitation Obstruction Obstruction Restriction Restriction Intra or extra-thoracic obstruction Intra or extra-thoracic obstruction Vocal chord dysfunction (VCD) Vocal chord dysfunction (VCD) Other pseudo-asthma - severe obesity Other pseudo-asthma - severe obesity Breathing kinetics Breathing kinetics Location of tidal breathing on the absolute lung volume scale Location of tidal breathing on the absolute lung volume scale EEVL/TLC EEVL/TLC")
14
Twenty-four prepubescent children Thirteen sportive children (10.8 + 1.1 y.o.) Eleven untrained children (10.5 + 1.0 y.o.) Twenty-four prepubescent children Thirteen sportive children (10.8 + 1.1 y.o.) Eleven untrained children (10.5 + 1.0 y.o.) J Appl Physiol 99: 1912–1921, 2005
 Eleven untrained children ( y.o.) Twenty-four prepubescent children Thirteen sportive children ( y.o.) Eleven untrained children ( y.o.) J Appl Physiol 99: 1912–1921, 2005")
15
20 asthmatics in a stable condition and aged 32+13 yrs with a FEV1 of 101+ 21% pred. Conclusion: Conclusion: In asthmatics with exercise-induced tidal expiratory flow limitation, the exercise capacity is reduced as a result of dynamic hyperinflation. 20 asthmatics in a stable condition and aged 32+13 yrs with a FEV1 of 101+ 21% pred. Conclusion: Conclusion: In asthmatics with exercise-induced tidal expiratory flow limitation, the exercise capacity is reduced as a result of dynamic hyperinflation. Eur Respir J 2004; 24: 378–384

16
22 years-old female Cough, chest tightness and wheezing Diagnosed with EIB with no response to BD Normal flow volume curve at rest Sawtooth Pattern

17
Breathing Kinetics: FVL Analysis Normal

18
Flow limitation

19
Breathing Kinetics: FVL Analysis Inappropriate Shift

20
Breathing Kinetics: FVL Analysis Vocal Cord Dysfunction

21
Breathing Kinetics: FVL Analysis Pseudo – Asthma “type 2”

22
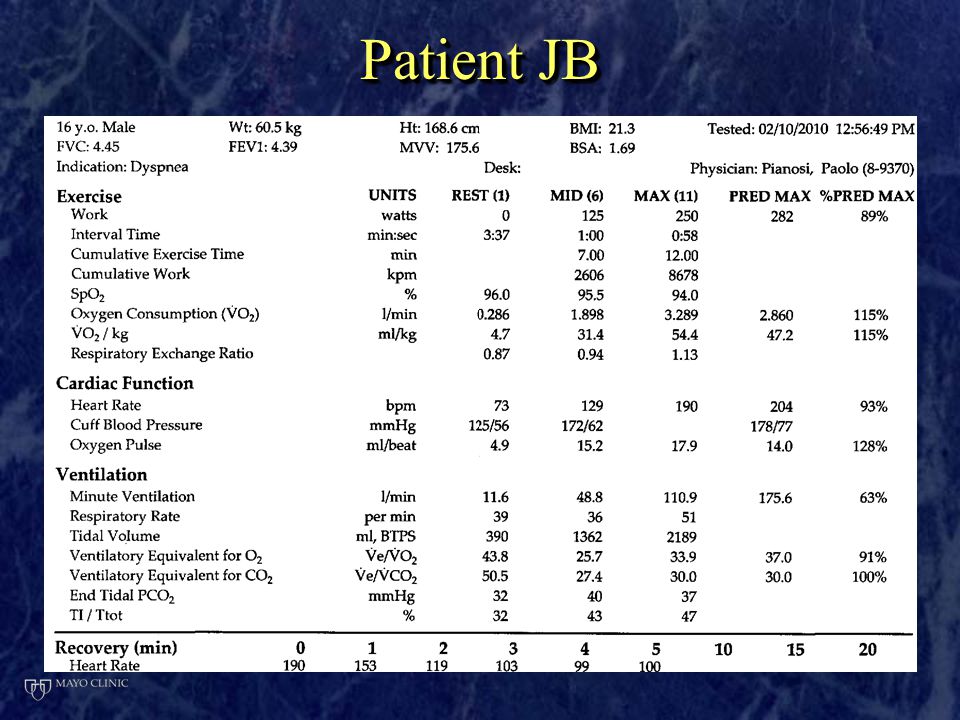
Patient JB 16 y.o. male with a chief complaint of exertional dyspnea 16 y.o. male with a chief complaint of exertional dyspnea Evaluation of suspected asthma Evaluation of suspected asthma Wrestling and cross-country Wrestling and cross-country Meds: Flovent, singulair, Xopenex Meds: Flovent, singulair, Xopenex 16 y.o. male with a chief complaint of exertional dyspnea 16 y.o. male with a chief complaint of exertional dyspnea Evaluation of suspected asthma Evaluation of suspected asthma Wrestling and cross-country Wrestling and cross-country Meds: Flovent, singulair, Xopenex Meds: Flovent, singulair, Xopenex

23
Patient JB

26
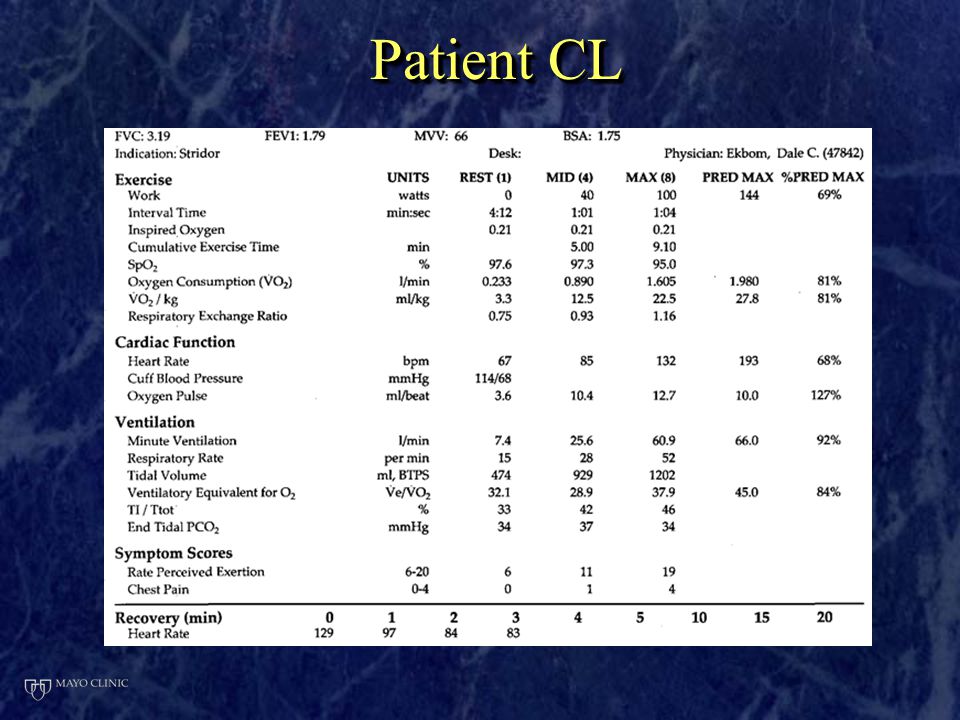
Patient CL 27 yo female with chief complaint of exertional dyspnea 27 yo female with chief complaint of exertional dyspnea PMH: Tetralogy of Fallot with absent pulmonary valve syndrome status post complete repair PMH: Tetralogy of Fallot with absent pulmonary valve syndrome status post complete repair CPET ordered to evaluate cardiac versus pulmonary CPET ordered to evaluate cardiac versus pulmonary 27 yo female with chief complaint of exertional dyspnea 27 yo female with chief complaint of exertional dyspnea PMH: Tetralogy of Fallot with absent pulmonary valve syndrome status post complete repair PMH: Tetralogy of Fallot with absent pulmonary valve syndrome status post complete repair CPET ordered to evaluate cardiac versus pulmonary CPET ordered to evaluate cardiac versus pulmonary

27
Patient CL

30
Patient EW 12 y.o. female referred for prolong QT syndrome and exercise intolerance 12 y.o. female referred for prolong QT syndrome and exercise intolerance HPI: HPI: Sports physical triggered and ECG which was read as borderline prolonged QT. Sports physical triggered and ECG which was read as borderline prolonged QT. Chest pain and wheezing with exercise Chest pain and wheezing with exercise PE: Unremarkable PE: Unremarkable 12 y.o. female referred for prolong QT syndrome and exercise intolerance 12 y.o. female referred for prolong QT syndrome and exercise intolerance HPI: HPI: Sports physical triggered and ECG which was read as borderline prolonged QT. Sports physical triggered and ECG which was read as borderline prolonged QT. Chest pain and wheezing with exercise Chest pain and wheezing with exercise PE: Unremarkable PE: Unremarkable

31
Patient EW ECHO: normal ECHO: normal Spirometry: FVC 3.17 (95%), FEV1 2.78 (97%), ratio 87.7% Spirometry: FVC 3.17 (95%), FEV1 2.78 (97%), ratio 87.7% Normal spirometry Normal spirometry CPET with FV Loops ordered to r/o EIB or vocal chord dysfunction CPET with FV Loops ordered to r/o EIB or vocal chord dysfunction ECHO: normal ECHO: normal Spirometry: FVC 3.17 (95%), FEV1 2.78 (97%), ratio 87.7% Spirometry: FVC 3.17 (95%), FEV1 2.78 (97%), ratio 87.7% Normal spirometry Normal spirometry CPET with FV Loops ordered to r/o EIB or vocal chord dysfunction CPET with FV Loops ordered to r/o EIB or vocal chord dysfunction
, FEV (97%), ratio 87.7% Spirometry: FVC 3.17 (95%), FEV (97%), ratio 87.7% Normal spirometry Normal spirometry CPET with FV Loops ordered to r/o EIB or vocal chord dysfunction CPET with FV Loops ordered to r/o EIB or vocal chord dysfunction ECHO: normal ECHO: normal Spirometry: FVC 3.17 (95%), FEV (97%), ratio 87.7% Spirometry: FVC 3.17 (95%), FEV (97%), ratio 87.7% Normal spirometry Normal spirometry CPET with FV Loops ordered to r/o EIB or vocal chord dysfunction CPET with FV Loops ordered to r/o EIB or vocal chord dysfunction")
32
Patient EW Normal sinus rhythm, normal ECG Normal sinus rhythm, normal ECG

33
Patient ID: EW816 Interpretation: Normal exercise tolerance, evidence of VCD

35
Laryngoscope, 109:136-139,1999

36
To compare laryngoscopically observed changes in the larynx during exercise in persons (2) with exercise-induced laryngomalacia (EIL) with changes in asymptomatic control subjects (8).
 with exercise-induced laryngomalacia (EIL) with changes in asymptomatic control subjects (8).")
37
12 normal subjects and 4 patients with DOE and noisy breathing 12 normal subjects and 4 patients with DOE and noisy breathing Conclusion: Continuous laryngoscopy with exercise was easy to perform and well tolerated 12 normal subjects and 4 patients with DOE and noisy breathing 12 normal subjects and 4 patients with DOE and noisy breathing Conclusion: Continuous laryngoscopy with exercise was easy to perform and well tolerated Laryngoscope, 116:52–57, 2006

38
Laryngoscope, 119:1776–1780, 2009

39
Respiratory Medicine (2009) 103, 1911-1918 151 of 166 patients with inspiratory distress during exercise 151 of 166 patients with inspiratory distress during exercise
 103, of 166 patients with inspiratory distress during exercise 151 of 166 patients with inspiratory distress during exercise")
40
The aims of this study were to establish a scoring system for laryngeal obstruction as visualized during the CLE-test as well as to assess reliability and validity of this scoring system. Eur Arch Otorhinolaryngol (2009) 266:1929–1936
 266:1929–1936.")
41
Conclusion: The CLE-test scoring system is a reliable and valid method that can be used to assess degree of laryngeal obstruction in patients with symptoms of EIIS

42
CPET with FV loops and Direct Laryngoscopy

43
Patient AJ 18 year-old athletic female complaining of dyspnea and wheezing with exertion HPI: HPI: Inspiratory wheezing, epigastric pain and tight feeling around the shoulders and neck with exertion Inspiratory wheezing, epigastric pain and tight feeling around the shoulders and neck with exertion Symptoms start after a minute or so of sprinting or 5-10 min. of regular exercise Symptoms start after a minute or so of sprinting or 5-10 min. of regular exercise Symbicort, Singulair and Xopenex x 1 year with no improvement 18 year-old athletic female complaining of dyspnea and wheezing with exertion HPI: HPI: Inspiratory wheezing, epigastric pain and tight feeling around the shoulders and neck with exertion Inspiratory wheezing, epigastric pain and tight feeling around the shoulders and neck with exertion Symptoms start after a minute or so of sprinting or 5-10 min. of regular exercise Symptoms start after a minute or so of sprinting or 5-10 min. of regular exercise Symbicort, Singulair and Xopenex x 1 year with no improvement

46
ENT and speech path consult Laryngoscopy: Thick secretions Thick secretions Normal mobility of the true vocal folds with full abduction and complete adduction Normal mobility of the true vocal folds with full abduction and complete adduction The subglottis was clear The subglottis was clear No paradoxical vocal fold when she attempted to mimic her dyspneic episodes No paradoxical vocal fold when she attempted to mimic her dyspneic episodes

48
Patient AJ

50
Diagnosis: Arytenoid collapse (laryngeal dysfunction) Diagnosis: Arytenoid collapse (laryngeal dysfunction) Patient was seen again by ENT and underwent arytenoidectomy Patient was seen again by ENT and underwent arytenoidectomy Diagnosis: Arytenoid collapse (laryngeal dysfunction) Diagnosis: Arytenoid collapse (laryngeal dysfunction) Patient was seen again by ENT and underwent arytenoidectomy Patient was seen again by ENT and underwent arytenoidectomy
 Diagnosis: Arytenoid collapse (laryngeal dysfunction) Patient was seen again by ENT and underwent arytenoidectomy Patient was seen again by ENT and underwent arytenoidectomy Diagnosis: Arytenoid collapse (laryngeal dysfunction) Diagnosis: Arytenoid collapse (laryngeal dysfunction) Patient was seen again by ENT and underwent arytenoidectomy Patient was seen again by ENT and underwent arytenoidectomy")
51
Patient TB 14 y.o. female with a chief complaint of dyspnea on exertion 14 y.o. female with a chief complaint of dyspnea on exertion PMH PMH Asthma “wheezing with colds” Asthma “wheezing with colds” Mother described “breathing attacks” Mother described “breathing attacks” CXR: Normal CXR: Normal Meds: Symbicort, Xopenex Meds: Symbicort, Xopenex 14 y.o. female with a chief complaint of dyspnea on exertion 14 y.o. female with a chief complaint of dyspnea on exertion PMH PMH Asthma “wheezing with colds” Asthma “wheezing with colds” Mother described “breathing attacks” Mother described “breathing attacks” CXR: Normal CXR: Normal Meds: Symbicort, Xopenex Meds: Symbicort, Xopenex

52
Patient TB

55
Baseline Immediate Post- Exercise

56
SummarySummary Flow volume loop analysis is beneficial in defining flow limitation and other breathing abnormalities during exercise Flow volume loop analysis is beneficial in defining flow limitation and other breathing abnormalities during exercise Continuous video laryngoscopy is a well tolerated procedure that can assist in characterizing structural abnormalities of the upper airway. Continuous video laryngoscopy is a well tolerated procedure that can assist in characterizing structural abnormalities of the upper airway. Flow volume loop analysis is beneficial in defining flow limitation and other breathing abnormalities during exercise Flow volume loop analysis is beneficial in defining flow limitation and other breathing abnormalities during exercise Continuous video laryngoscopy is a well tolerated procedure that can assist in characterizing structural abnormalities of the upper airway. Continuous video laryngoscopy is a well tolerated procedure that can assist in characterizing structural abnormalities of the upper airway.

57
Questions?

Similar presentations







: ITC3-1. * For Best Viewing: Open in Slide Show Mode Click on icon or From the View.>")











 1.3 breathing reserve < 20% (N=20-40%)>")






>")