Download presentation
Presentation is loading. Please wait.

1
HEPATITIS B

2
EPIDEMIOLOGY Highly endemic in Southeast Asia
Materno-fetal transmission in these areas 90% transmission if E antigen positive as opposed to 15-20% if E antibody positive Low incidence since routine screening of blood donors since 1970 In U.S , high risk sexual behaviour and IV drug use No source of infection in 15%

3
Natural course of infection
Fulminant hepatits in 1% Only 20% survival in fulminant hepatitis, in the absence of liver transplantation HBV carriers: Normal lfts, asymptomatic 1-5% become chronically infected 30% of above will develop cirrhosis 85% , five year survival for compensatec cirrhosis 15% , five survival with decompensation

4
MOLECULAR BIOLOLGY OF HEP B VIRUS
DNA virus Genotypes A-H ( A has best response to IFN ) Genotype A is predominant in the U.S Replication E- Antigen RT core surface X Protein Polymerase Carcinogenesis Surface Antigen
 Genotype A is predominant in the U.S. Replication. E- Antigen. RT. core. surface. X Protein. Polymerase. Carcinogenesis. Surface Antigen.")
5
MOLECULAR BIOLOGY OF HEPATITIS B VIRUS
Hepatitis Surface antigen mutation After liver transplantation With chronic Hepatitis Immune globulin administraton Result in recurrence of infection Hep Surface Antigen Neg Surface antibody pos (from vaccination) DNA PCR positive
 DNA PCR positive.")
6
MOLECULAR BIOLOGY OF HEPATITIS B VIRUS
Hepatitis B Pre-Core mutation Loss of E antigen Can cause fulminant hepatitis May reduce response to Interferon Surface antigen pos E antigen negative E antibody negative PCR positive Hepatitis B Polymerase mutation Seen with treatment with polymerase inhibitors like lamivudine, adefovir etc Called YMDD mutation

7
Hepatitis B virus: Clinical Features and Diagnosis
Chike Anusionwu, M.D GI Fellow, PGY 4 09/23/09

8
Clinical Features Incubation period: few wks-6mths (60-90days)
Factors that reduce the IP Coinfection: HCV, HDV, HIV Underlying liver disease IP depends on the amount of replicating virus in the inoculum

9
Clin Features of Acute infection
Acute infections are heralded by a serum sickness-like prodrome of fever, arthralgias/arthritis, and rash, which is most commonly maculopapular or urticarial, in 10% to 20% of patients. This prodrome results from circulating HBsAg-anti-HBs complexes that activate complement and are deposited in the synovium and walls of cutaneous blood vessels. These features generally abate before the manifestations of liver disease and peak serum aminotransferase elevations are observed. Jaundice develops in only about 30% of patients.

10
CF of Acute Infections/Labs
Clinical symptoms and jaundice generally disappear after 1-3mths, but some pts have prolonged fatigue even after serum ALT levels return to nml. Elev serum ALT levels and serum HBsAg titers decline and disappear together, and in approximately 80% of cases, HBsAg disappears by 12wks after the onset of illness. In 5-10% of cases, HBsAg is cleared early and is no longer detectable by the time the patient first presents to a healthcare provider. Persistence of HBsAg after 6mths implies development of a carrier state, with only a small likelihood of recovery during the next 6-12 mths. Delayed clearance of HBsAg has been reported to be preceded by a decline in HBsAg titers.

11
Labs Serum aminotransferase levels of 1000 to 2000 U/L are typical, with ALT being higher than AST levels. In patients with icteric hepatitis, the rise in serum bilirubin levels often lags behind that in ALT levels. The peak ALT level does not correlate with prognosis, and the PT is the best indicator of prognosis. After clinical recovery from acute hepatitis B and HBsAg seroconversion, HBV DNA often remains detectable in serum as determined by a PCR assay.

12
Fulminant Hep B Fulminant hepatitis occurs in <1% of cases.
Fulminant hepatitis B generally occurs within 4wks of the onset of symptoms and is associated with encephalopathy, multiorgan failure, and a high mortality rate (>80%) if not treated by liver transplantation. Patients >40 years appear to be more susceptible than younger persons to "late-onset liver failure," in which encephalopathy, renal dysfunction, and other extrahepatic complications of severe liver insufficiency become manifest over the course of several months. The pathogenic mechanisms of fulminant hepatitis are poorly understood but are presumed to involve massive immune-mediated lysis of infected hepatocytes. This proposed mechanism may explain why many patients with fulminant hepatitis B have no evidence of HBV replication in serum at presentation.
 if not treated by liver transplantation. Patients >40 years appear to be more susceptible than younger persons to late-onset liver failure, in which encephalopathy, renal dysfunction, and other extrahepatic complications of severe liver insufficiency become manifest over the course of several months. The pathogenic mechanisms of fulminant hepatitis are poorly understood but are presumed to involve massive immune-mediated lysis of infected hepatocytes. This proposed mechanism may explain why many patients with fulminant hepatitis B have no evidence of HBV replication in serum at presentation.")
13
Chronic Hep B Hx of acute infection is often lacking Asymptomatic
Commons sxs: fatigue, poor appetite and malaise. RUQ pain may occur but is low grade. When superimposed on cirrhosis, reactivation of HBV infection may be assoc with jaundice and signs of liver failure. Features of decompensated cirrhotic Hep B include; spider angiomata, ascites, peripheral edema,hypoAlb, prolonged PT, AST>ALT

14
Extrahepatic manifestations
Pathogenesis is unclear but likely involves an aberrant immunologic response to extrahepatic viral proteins. Often in assoc with circulating immune complexes that activate serum complement. Examples: Arthritis Dermatitis Polyarteritis nodosa Glomerulonephritis Essential mixed cryoglobulinemia Type II(polyclonal IgG and monoclonal IgM) Type III (polyclonal IgG and RF)
 Type III (polyclonal IgG and RF)")
15
Histopathologic Features
Chr HBV infxn mononuclear cell infiltration in the portal triads NO steatosis Ground glass hepatocytes Chr Hep C has steatosis

16
Diagnosis HBsAg appears in serum 2-10wks after HBV exposure, before sxs or labs changes. In self limiting acute hepatitis, HBsAg disappears in 4-6mths. Persistence of HBsAg >6mths Chr HBV Several weeks later, anti-HBs appears persists for life and provide longterm immunity Coexistence of HBsAg and anti-HBs occurs in 25%. Implies chronic HBV and not acute HBV

17
Diagnosis Window period (several wks-mths)– b/w disappearance of HBsAg and appearance of anti-HBs. Check IgM anti-HBc Anti-HBc is detectable in acute and chronic infective states. In an acute infection,anti-HBc can linger in serum up to 4-6mths.

18
Clinical significance of isolated anti-HBc
Isolated anti-HBc has a prevalence of 1-4%, in nonendemic areas. Clinical scenarios: during the window period of acute hepatitis B, when anti-HBc is predominantly of the IgM class many years after recovery from acute hepatitis B, when anti-HBs has fallen to undetectable levels as a false-positive serologic test result after many years of chronic infection, when the HBsAg titer has fallen below the level of detection in persons who are coinfected with HCV and, rarely, as a result of varying sensitivity of HBsAg assays. Evidence for coinfection with HCV has been demonstrated in up to 60% of persons in whom anti-HBc is the only marker of HBV

19
Isolated anti-HBc PCR testing of sera with isolated anti-HBc have shown HBV DNA in 0-30% As a result, the patients are infective. E.g, anti-HBc testing of blood donors prevents some cases of post-transfusion hepatitis B. The risk of transmission of HBV infection from a liver donor with isolated anti-HBc has been found to be as high as 50-70% in some series.

20
HBeAg A viral protein found in serum early furing acute infection.
HBeAg reactivity usually disappears at or soon after the peak in serum aminotransferase levels persistence of HBeAg 3 or more months after the onset of illness indicates a high likelihood of transition to chronic HBV infection. HBeAg in serum of an HBsAg carrier indicates greater infectivity high level of viral replication the need for antiviral therapy.

21
HBeAg Most HBeAg-positive patients have active liver disease.
The exceptions are HBeAg-positive children young adults with perinatally acquired HBV infxn, who usually have normal serum ALT levels and minimal inflammation of the liver. Seroconversion from HBeAg to anti-HBe is assoc with reduction in serum HBV DNA levels of 3 log10 copies/mL or greater remission of liver disease. Some patients, however, continue to have active liver disease and detectable HBV DNA in serum because of low levels of wild-type virus or the selection of precore or core promoter mutations that impair HBeAg secretion.

22
HBV DNA Can be measured in serum with qualitative or quantitative assays The clinical utility of testing for serum HBV DNA has been hampered by the absence of a licensed test in the US as well as an accepted international reference standard. A number of non-PCR-based assays are available. are less sensitive than the PCR-based ones their results correlate with clinical response to antiviral therapy several of the currently available antiviral therapies were licensed on the basis of clinical trials in which these assays were used. Use of these less sensitive non-PCR-based assays has several shortcomings Most clinical laboratories use one of several commercially available PCR assays Non-PCR based assays sens: copies/ml PCR asays sens: 102 copies or less/ml

23
HBV DNA Measurement of serum HBV DNA is used
to evaluate a patient's candidacy for antiviral therapy to monitor response during treatment. Pts with high serum HBV DNA levels at baseline respond less to therapy with conventional interferon than pts with low levels. The use of solution hybridization testing, a baseline HBV DNA level of 200 pg/mL (roughly equivalent to 56 million copies/mL on a PCR assay) or greater has been found to be associated with a very low rate of response to standard interferon.
 or greater has been found to be associated with a very low rate of response to standard interferon.")
24
HBV DNA In contrast, baseline serum HBV DNA levels have not been shown to correlate with response to nucleoside analog therapy because of the more potent inhibition of viral replication by these agents. Monitoring of HBV DNA levels during therapy allows one to predict the likelihood of HBeAg clearance. The likelihood of relapse after treatment is discontinued Development of resistance to lamivudine Reappearance of HBV DNA in serum during treatment suggests that drug resistance has occurred.

25
Testing for HBV DNA Qualitative PCR is a more sensitive method of detecting HBV DNA than quantitative PCR. Small amts of HBV DNA can be detected in serum and peripheral mononuclear cells, years after recovery from acute hepatitis B. Even after disappearance of HBsAg and apparent loss of HBV DNA from serum in patients with chronic hepatitis B, small amounts of HBV DNA persist in liver tissue and peripheral mononuclear cells years later. Detection of HBV DNA in serum by a qualitative PCR assay before liver transplantation may identify patients who are at increased risk of apparent de novo hepatitis after transplantation may pinpoint HBV as the cause of liver disease in HBsAg-negative patients. in diagnosing patients with fulminant hepatitis B, who frequently have cleared HBsAg by the time they seek medical attention.

26
In Summary

27
Table summary

28
Hepatitis B Waheed Gul GI Fellow

29
Diagnostic criteria Chronic hepatitis B
1. HBsAg-positive 6 months 2. Serum HBV DNA 20,000 IU/mL, lower values 2, ,000 IU/mL are often seen in HBeAg-negative chronic hepatitis B 3. Persistent or intermittent elevation in ALT/AST levels 4. Liver biopsy showing chronic hepatitis with moderate or severe necroinflammation

30
Diagnostic criteria Inactive HBsAg carrier state
1. HBsAg-positive 6 months 2. HBeAg–, anti-Hbe+ 3. Serum HBV DNA 2,000 IU/mL 4. Persistently normal ALT/AST levels 5. Liver biopsy confirms absence of significant hepatitis

31
Liver Biopsy Role in management in hepatitis B
The purpose of a liver biopsy is to assess the degree of liver damage and to rule out other causes of liver disease. Liver biopsy is most useful in persons who do not meet clear cut guidelines for treatment . Recent studies suggest that the upper limits of normal for ALT and AST should be decreased to 30 U/L for men and 19 U/L for women. HBV infected patients with ALT values close to the upper limit of normal may have abnormal histology and can be at increased risk of mortality from liver disease especially those above age 40.

32
Patients that should be considered for treatment of hepatitis B
Patients with HBeAg-positive ALT greater than 2 times normal or moderate/severe hepatitis on biopsy, and HBV DNA >20,000 IU/mL.

33
Medications for hepatitis B treatment
First-line oral antiviral medications -tenofovir (viread) mg -entecavir, (baraclude) 0.5mg -interferon (for patients without cirrhosis) Second-line oral antiviral medications. -adeofovir (hepsera) 10mg -lamividine (epivir, 3TC) 100mg -telbivudine (tyzeka) 600mg Other: Emtricitabine (Emitriva, FTC) and Truvada (in combination with tenofovir, approve for HIV treatment
 300 mg. -entecavir, (baraclude) 0.5mg. -interferon (for patients without cirrhosis) Second-line oral antiviral medications. -adeofovir (hepsera) 10mg. -lamividine (epivir, 3TC) 100mg. -telbivudine (tyzeka) 600mg. Other: Emtricitabine (Emitriva, FTC) and Truvada (in combination with tenofovir, approve for HIV treatment.")
34
Serum HBV DNA levels of 20,000 IU/mL and elevated ALT levels :
-entecavir, tenofovir, or peginterferon alfa-2a might be considered as first-line options; High levels of serum HBV DNA and/or normal levels of ALT: -given that response to interferon-based therapy is low in this population, however, entecavir or tenofovir would be preferred

35
Emtricitabine (emtriva, FTC)
It is a potent inhibitor of HIV and hep B It approved for HIV treatment as emtriva and as Truvada (in combination with tenofovir as a single pill)
")
36
Duration of treatment ● IFN-alpha: 16 weeks ● PegIFN-alpha: 48 weeks ● LAM/ADV/ETV/LdT/TDF: minimum 1 year, continue for at least 6 months after HBeAg seroconversion

37
Important points about Duration of treatment
Hbe Ag-positive patients continue to be treated after HBeAg seroconversion as long as HBV DNA levels are decreasing and until the HBV DNA levels are undetectable by PCR. Treatment then should be continued for an additional 12 months. In patients who undergo HBeAg seroconversion but who still have detectable but stable HBV DNA levels, treatment should be continued for 6 months; seroconversion should be documented again, and then consideration should be given to stopping treatment in patients without cirrhosis. Patients who relapse can be re-treated. HBeAg-positive patients who fail to lose HBeAg should be treated long-term because the chance of HBeAg seroconversion increases with time, and there is a high risk of recurring viremia if therapy is stopped in the absence of HBeAg seroconversion.

38
End-point of treatment
Seroconversion from HBeAg to anti-HBe

39
Patients who failed to achieve primary response
Patients who failed to achieve primary response as evidenced by <2 log decrease in serum HBV DNA level after at least 6 months of NA therapy should be switched to an alternative treatment or receive additional treatment.

40
Recommendations for Treatment: HBeAg-Positive CHB
HBV DNA ALT Treatment strategy <20,000 Normal No treatment Monitor every 6–12 mo Consider therapy if significant histologic disease, even if low level replication

41
Recommendations for Treatment: HBeAg-Positive CHB
HBV DNA ALT Treatment strategy >20,000 Normal Consider liver biopsy particularly if patient is 35–40 y; treat if disease; in the absence of biopsy examination, observe increase in ALT levels

42
Recommendations for Treatment: HBeAg-Positive CHB
HBV DNA ALT Treatment strategy >20, Elevated Entecavir, tenofovir, or peginterferon alfa-2a preferred

43
Duration of therapy HBeAg-positive patients continue to be treated after HBeAg seroconversion as long as HBV DNA levels are decreasing and until the HBV DNA levels are undetectable by PCR. Treatment then should be continued for an additional 12 months. In patients who undergo HBeAg seroconversion but who still have detectable but stable HBV DNA levels, treatment should be continued for 6 months then consideration should be given to stopping treatment in patients without cirrhosis. Patients who relapse can be re-treated.

44
Duration of therapy HBeAg-positive patients who fail to lose HBeAg should be treated long-term because the chance of HBeAg seroconversion increases with time, and there is a high risk of recurring viremia if therapy is stopped in the absence of HBeAg seroconversion

45
Recommendations for Treatment: HBeAg-Negative CHB
HBV DNA ALT Treatment strategy <2000 Normal No treatment; majority are inactive HBsAg carriers Monitor every 6–12 mo Consider therapy if significant histologic disease, even if low level replication

46
Recommendations for Treatment: HBeAg-Positive CHB
HBV DNA ALT Treatment strategy >2000 Normal Consider liver biopsy particularly if patient is 35–40 y; treat if disease; in the absence of biopsy examination, observe increase in ALT levels

47
Recommendations for Treatment: HBeAg-Positive CHB
HBV DNA ALT Treatment strategy > Elevated Entecavir, tenofovir, or peginterferon alfa-2a preferred Long-term treatment required for oral agents

48
Duration of therapy for HBeAg-negative patients
HBeAg-negative patients who are receiving therapy should be monitored every 6 months. The duration of therapy with peginterferon remains unclear, although longer treatment (12 months) appears to be more beneficial in terms of sustained virologic response off treatment than do shorter periods of treatment. Entecavir, tenofovir, and telbivudine need to be given for the long term;
 appears to be more beneficial in terms of sustained virologic response off treatment than do shorter periods of treatment. Entecavir, tenofovir, and telbivudine need to be given for the long term;")
49
Monitoring Virologic Response and Management of Resistance to Oral Antiviral Therapy
Prolonged antiviral therapy is associated with the development of antiviral resistance. The long term rates of resistance are highest for lamivudine (65%–70% at 4–5 years), intermediate for telbivudine (25% in HBeAg-positive patients and 11% in HBeAg-negative patients at 2 years), lower for adefovir (29% at 5 years),and lowest for entecavir in the absence of prior lamivudine resistance (1.2% at 5 years) and for tenofovir in treatment-naïve patients (0% at 1 year). The development of resistance is associated with loss of initial response and HBV DNA rebound →biochemical breakthrough →reversion of histologic improvement and in some cases, resistance leads to progressive liver disease
, intermediate for telbivudine (25% in HBeAg-positive. patients and 11% in HBeAg-negative patients at 2 years), lower for adefovir (29% at 5 years),and lowest for entecavir in the absence of prior lamivudine resistance (1.2% at 5 years) and for tenofovir in treatment-naïve patients (0% at 1 year). The development of resistance is associated with loss of initial response and HBV DNA rebound →biochemical breakthrough. →reversion of histologic improvement and in some cases, resistance leads to progressive liver disease.")
50
On-Treatment Monitoring
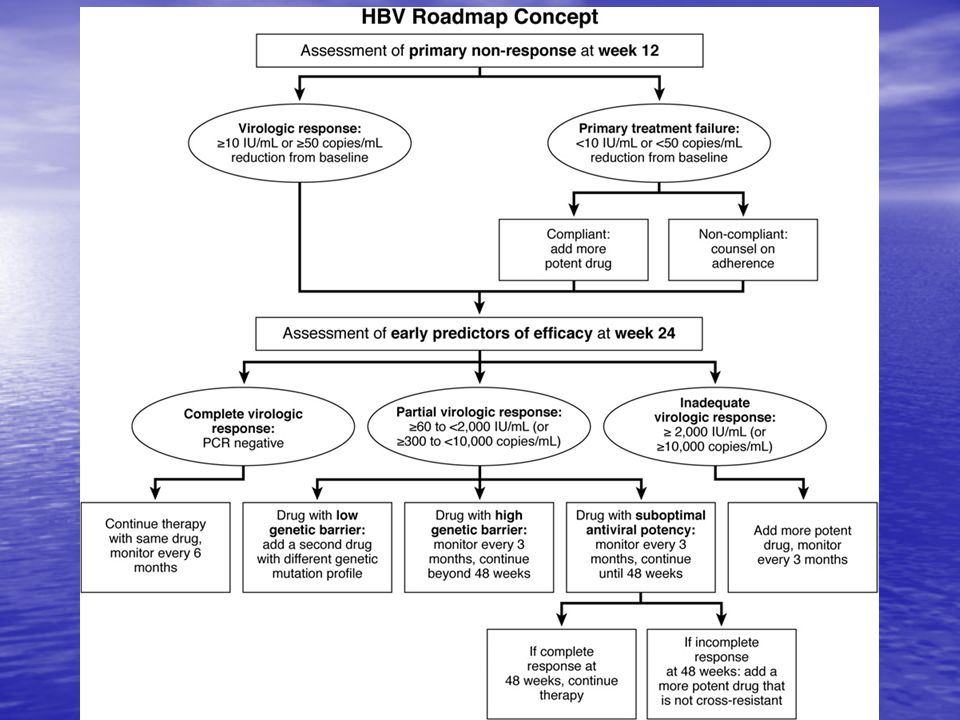
Serum HBV DNA levels should be monitored at 12 weeks to determine primary treatment failure (HBV DNA decline of <1 log10 IU/mL) and at 24 weeks to confirm adequate virologic suppression by antiviral therapy. At 24 weeks, virologic response should be categorized as complete, partial, or inadequate, according to the following definitions: -complete, HBV DNA level 60 IU/mL; -partial, HBV DNA level 60 to 2000 IU/mL; and inadequate, HBV DNA level 2000 IU/mL
 and at 24 weeks to confirm adequate virologic suppression by antiviral therapy. At 24 weeks, virologic response should be categorized as complete, partial, or inadequate, according to the following definitions: -complete, HBV DNA level 60 IU/mL; -partial, HBV DNA level 60 to 2000 IU/mL; and inadequate, HBV DNA level 2000 IU/mL.")
52
Recommendation for all cases of HBV resistance
The recommendation for all cases of HBV resistance is to use add-on therapy with a drug in another class, while continuing therapy with the original drug, or to switch to another drug within that same class but one that is more potent

53
Management of Antiviral-Resistant HBV
Prevention ● Avoid unnecessary treatment ● Initiate treatment with potent antiviral that has low rate of drug resistance or with combination therapy ● Switch to alternative therapy in patients with primary non-response Monitoring ● Test for serum HBV DNA (PCR assay) every 3-6 months during treatment ● Check for medication compliance in patients with virologic breakthrough ● Confirm antiviral resistance with genotypic testing
 every 3-6 months during treatment ● Check for medication compliance in patients with virologic breakthrough ● Confirm antiviral resistance with genotypic testing")
54
Management of Antiviral-Resistant HBV
Treatment Lamivudine-resistance → Add adefovir or tenofovir Stop lamivudine, switch to Truvada in HIV Adefovir-resistance → Add lamivudine Stop adefovir, switch to Truvada in HIV Switch to or add entecavir Entecavir-resistance → Switch to tenofovir or Truvada Telbivudine-resistance→ Add adefovir or tenofovir Stop telbivudine, switch to Truvada

55
Treatment of Cirrhotic (HBeAg-Positive or HBeAg-Negative)
HBV DNA Cirrhosis Treatment strategy <2000 Compensated Might choose to treat or observe Entecavir or tenofovir preferred >2000 Compensated Entecavir or tenofovir are first-line options Long-term treatment required, and combination therapy might be preferred

56
Treatment of Cirrhotic (HBeAg-Positive or HBeAg-Negative)
HBV DNA Cirrhosis Treatment strategy Any detectable Decompensated Combination with lamivudine, or possibly entecavir, plus tenofovir preferred Long-term treatment required, and combinationtherapy might be preferred Wait list for liver transplantation

Similar presentations










 indistinguishable from other hepatitis causes and is quite variable from asymptomatic.>")
, Hepatovirus Picornavirus, enterovirus 72 27 nm 1 serotype only, although there are 4 genotypes.>")







